
How can you deal with a virus that has the capability of even switching its entry route?
Laboratory experiments demonstrate that #Omicron has switched its route of entry in to human cells. 1/
Laboratory experiments demonstrate that #Omicron has switched its route of entry in to human cells. 1/
This is likely to influence #Omicron spread and the types of cells it can hijack. 2/
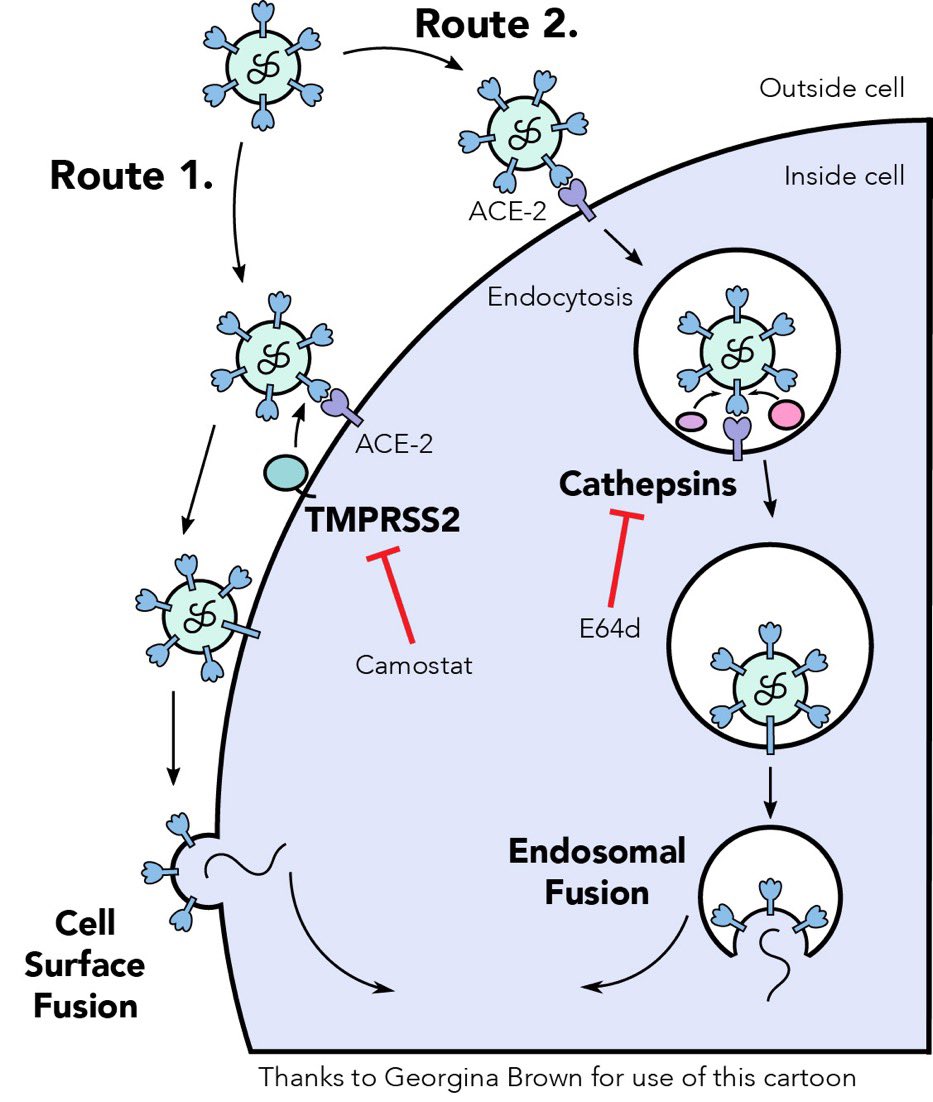
#SARS2 can enter cells via two routes, both routes require spike activation by proteases.
Route 1: Cell surface fusion, triggered by #TMPRRS2.
Route 2: endosomal fusion, triggered by cathepsins.
So far SARS2 has favoured Route 1.
3/
Route 1: Cell surface fusion, triggered by #TMPRRS2.
Route 2: endosomal fusion, triggered by cathepsins.
So far SARS2 has favoured Route 1.
3/
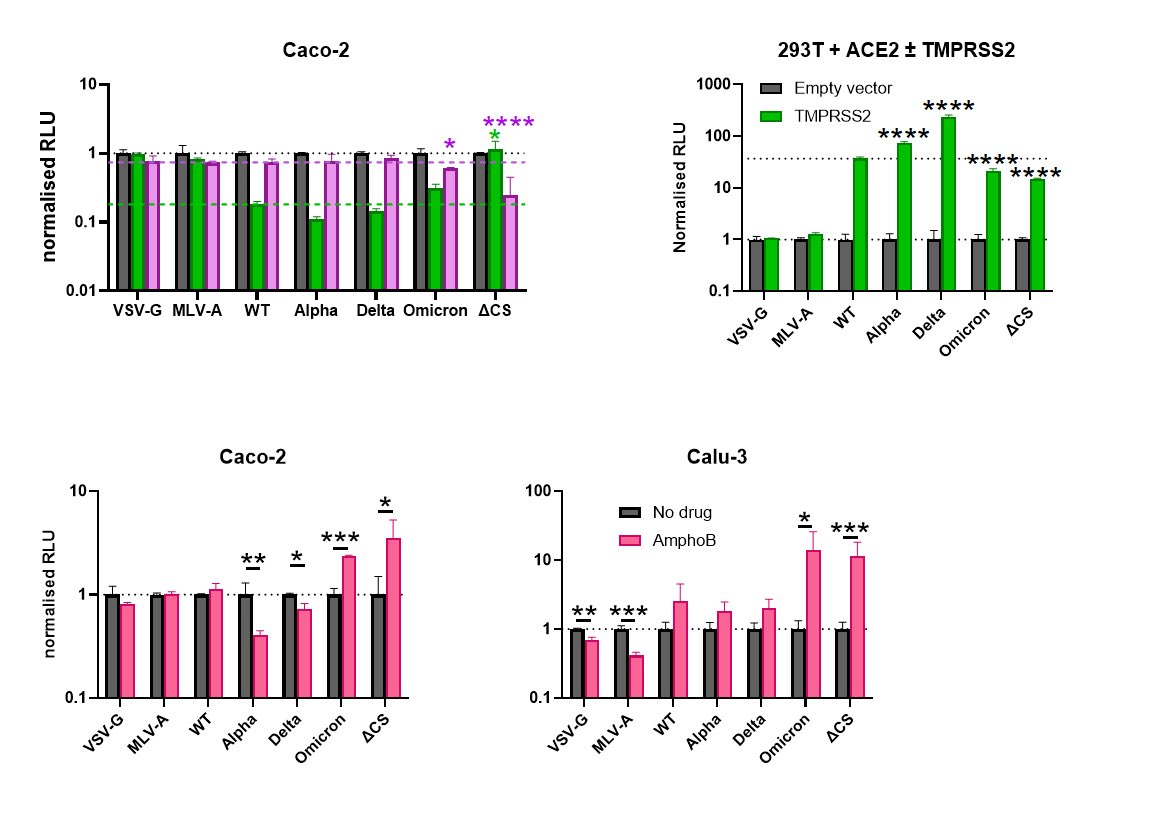
There is strong evidence of a dramatic switch in #Omicron entry route from cell surface to endosomal fusion. 4/
Omicron has shifted from a TMPRSS-2-dependent fusion at the cell surface, to a cathepsin-dependent endosomal fusion. So, the preferred entry mechanism of Omicron is different now (ie, it's a big big big change). 5/
Another consequence of this switch is that #Omicron can no longer mediate TMPRSS2-dependent fusion of infected cells with adjacent non-infected cells. So reduced fusogenicity may not hamper its infectivity! 6/
Omicron may be deficient at syncytium formation but it can move to other cells better than previous thru enhanced endosome fusion.
This sort of thing could affect tissue tropism, the tendency of a particular variant to invade a particular organ or not. 7/
This sort of thing could affect tissue tropism, the tendency of a particular variant to invade a particular organ or not. 7/
These discoveries may have implications for the tissue preference of #Omicron and for viral transmission. 8/
https://twitter.com/grovelab/status/1476584183434784770?s=21
These results were confirmed by other researchers too with the freshest results by @PeacockFlu and team. 9/
@PeacockFlu proposes a model where Omicron has become less specialised in its entry route and become more of a 'generalist' - this allows it to efficiently infect a greater number of cells in the upper respiratory tract and may mean it even has a lower infectious dose? 10/

@PeacockFlu also concludes that Omicron Spike is more able to use the endosomal entry route than previous variants, being less sensitive to TMPRSS2-mediated entry and more sensitive to inhibitors of endosomal entry. 11/
https://twitter.com/peacockflu/status/1477227925124616192?s=21
We all know about the ‘furin cleavage site’ (FCS) at S1/S2 junction. Similar to this FCS, the 637 cathepsin site is located in a flexible loop region, which would allow cleavage. 12/
https://twitter.com/_b_meyer/status/1477254346245128198?s=21

It will be important to tease out what the drop in TMPRSS-2 cleavage & the increase of importance for cathepsin-dependent entry causes in #Omicron. If it is due to epistatic effects by several mutations the reversion is likely a multi-step process. 13/
And if this could change back to a TMPRSS-2 use and likely associated pathogenicity in a much easier way?? this is purely speculative at this point.
14/
14/
The new findings on Omicron’s preferred way of entry to the host cell led to new sketches 👇
• • •
Missing some Tweet in this thread? You can try to
force a refresh






