I do think medicine needs a Catholic Church-style reckoning. I know that might sound like an odd analogy but when you stop talking about bad apples and realize the problem is fundamental and systemic, that it destroys lives... #DoctorsAreDickheads #medtwitter
...and that the reverence we have for the individuals that comprise the system helps no one (not our doctors, not the patients they are sworn to protect), only then can you hope to fix it. But you have to kill your old illusions first. #DoctorsAreDickheads #medtwitter
(I don’t know how or when that will happen.)
There are few relationships left in our society as unequal as the doctor-patient relationship. Medicine is one of the last institutions built on such an extreme power imbalance. Around such relationships there is a lot of potential for abuse. #medtwitter #DoctorsAreDickheads
And speaking as an ex-social scientists, one of the biggest downsides of hierarchical relationships is information asymmetry. Specifically the more powerful actor never really knows what is going on with the less powerful actor either because a) they don’t care
or b) the one with less power shapes, withholds, edits information as a survival strategy, often because surviving means telling the more powerful actor what they want to hear.
And so there is a lot of talk about doctor-patient trust and the voice of the patient but in the context of a relationship that is fundamentally designed to engender mistrust, abuse, and low quality information.
The outcome is not in the hearts of men it’s in the design of the system. Which is why #DoctorsAreDickheads is not quite right and #NotAllDoctors is so besides the point.
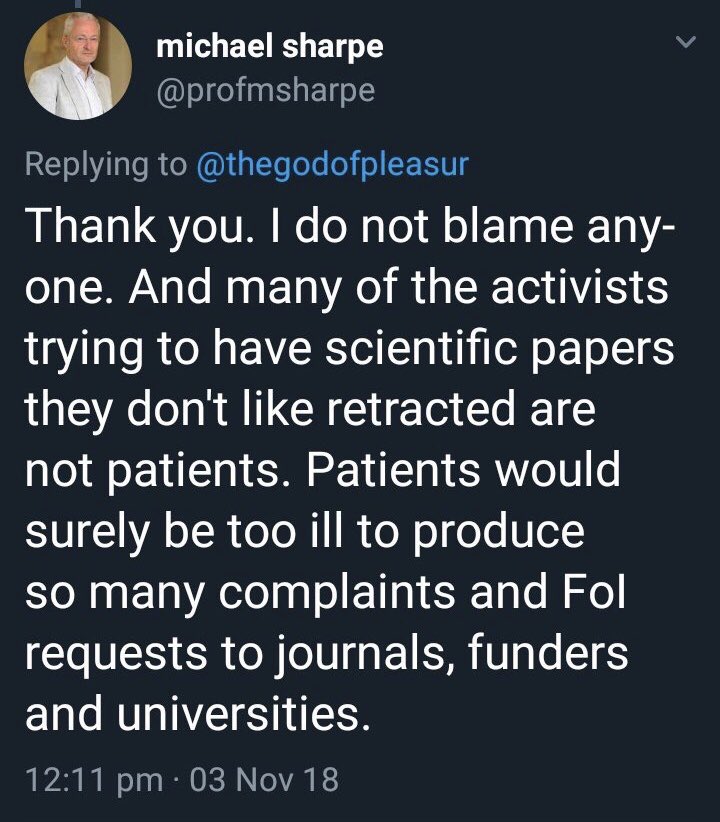
And you see it in all the #DoctorsAreDickheads stories: doctors gaslighting patients and rejecting the information they are providing, patients editing their stories, years or decades of misdiagnosis, preventable disability or death, zero repercussions or feedback mechanisms.
So here are some things that what *should* help (and there are many medical systems implementing at least some of these mechanisms).
1) reducing information asymmetry: open notes (with collaborative writing in-office, how many times has a doctor translated a symptom in his head and come out with something way off?), email/private messaging
...immediate access to all data without request including original imaging (which doesn’t need to be on CDs anymore! Please find another way). You see everything in real time, just like your doctor does.
2) improving feedback mechanisms: immediate (internal) customer satisfaction ratings, exit interviews when patients and don’t come back to see you (hint: X times out of 10 it’s not because they magically got better).
Aside: I do wonder why external ratings or so poor. Like, why don’t more people use health grades? There are actually a lot of healthcare ratings on yelp, but more of small private practices than large university hospitals/specialists.
3) A quasi-independent, ombudsman-like figure: someone to help you navigate sticky situations like “I can’t breathe WHEN I AM AWAKE and have no quality of life but my neuro wants me to do a sleep study and see her in three months
and hasn’t ordered any of the appropriate imaging to diagnose me b/c she has no idea what is going on but two doctors have suggested a highly probably diagnosis and here are their notes is how do we get on that? So I don’t have to sleep sitting up for the next 90 days.
4) make better use of home data collection: wearables, likhert sx tracking, daily dairies. Some clinics are prescribing wearables, but more often than not, doctors DENY the data these devices collect as unreliable or kid-you-not, blame the symptom on the device.
A cardiologist recently told me (knowing my four year-diagnosis of #POTS) that the reason my HR went to 158 when I tried sitting up while in a hospital was because the Apple Watch I was wearing was giving me anxiety about my HR, causing my HR to go up. #DoctorsAreDickheads
(I had no idea it was that high and only knew it b/c an alarm went off at the nurse’s station *on their heart monitors* and a nurse came running in). The physical therapists who were at the time still thought it was a good idea for me to stand up...
5) medical education that is hierarchy reducing: I have no idea what precisely this should look like, not having been to med school...
...but surely getting As in a history of science or medicine class, an intro to probability class (or whatever improves one’s understanding of causation) and a disability studies class should be just as important as part of med school admissions as that organic chemistry class?
6) recognize the ghost in the machine problem: we need to do some hard work to combat magical thinking among doctors. They take science classes but some of the fundamental habits of mind that come from the disciplines of science just don’t stick. I don’t know why.
Medical providers need STOP PSYCHOLOGIZING away their own inadequacies because they are killing their patients. It’s OK that you’re inadequate. You aren’t suppposed to know everything. Somewhere out there, someone does, so fight to help your patient find that person.
But the idea that we have this mind that can move mountains and do magical things belongs in the thinking of the Greeks, Middle Age theologians or Puritans or Freud, which where it came from, and not in 21st century medicine.
If you cannot offer a objective proof within the case of the given patient or design an experiment that could offer proof for a sample of the population, it has NO PLACE IN MEDICINE. So non-psychiatrists, stop giving out psych misdiagnoses like candy.
7) Everything need to become MUCH cheaper. Why does a brain MRI cost thousands of dollars 41 years after its invention? Why is there essentially 2 major national labs?
Why is there almost no competition and such little innovation such that everything costs so much and is kind of disappointing? In this age when all of our other gadgets are so freaking cool?
Part of the “there, there dear” dismissal of patients is ego protection, but part of it is time + cost management. You have to justify the tests you run. Diagnosis shouldn’t have to be rationed. We should be able to look and seek until we find out what is actually wrong with you.
8) We need to augment humans: we already do this with electronic record-keeping, Google, Up-to-Date, but the potential for software/AI to bridge the gap between what it is possible to know and an individual’s capacity for pattern-recognition is vast, particularly w/ visual data.
I don’t see a solution that isn’t at least in part technology-driven. And some of that technology can be low-fi.
Example: why is the collection of your history almost always solely narrative? Where are the structured symptom surveys that ask you about sx that could be diagnostic but you’d *never* think to report? But could allow for the collection and comparability of data on a vast scale?
9) The patient needs to become the customer: I don’t know who the customer is in healthcare. Insurance companies, in part. Government, in part. Doctors are service providers but unless they are independent operators, in the scheme of things, they don’t have much power, either.
But there is nothing that looks like market, customer service-driven outcomes in most of medicine. No wonder why the purported customer is so unhappy. Until this changes, 1-8 are just icing.
Lastly: I am really grateful to have the care team I have around me today. It took seven years to find and build that team. It should not have taken that long, and I had make a film and learn a lot about medicine and my disease to find them.
It is definitely #NotAllDoctors but the system is set up to obstruct your efforts to find the person who has the knowledge and experience to help you, when it should be focused on helping patients and doctors find the most effective match.