,
27 tweets,
9 min read
Read on Twitter
1/n A webinar from @CDC_Genomics on Mendelian randomization (MR) highlights some under-appreciated aspects of MR; this thread outlines these
2/n The key interpretive assumption in MR is of gene-environment equivalence: that perturbations caused by genotype have the same downstream effects as if they were caused by modifiable exposures (at 7 mins 40 seconds)
3/n Thus if LDL cholesterol is low due to genotype this will have the same downstream effects (e.g. on coronary heart disease, CHD) as LDL cholesterol will have if it is low due to diet or taking statins (or other cholesterol lowering drugs) 
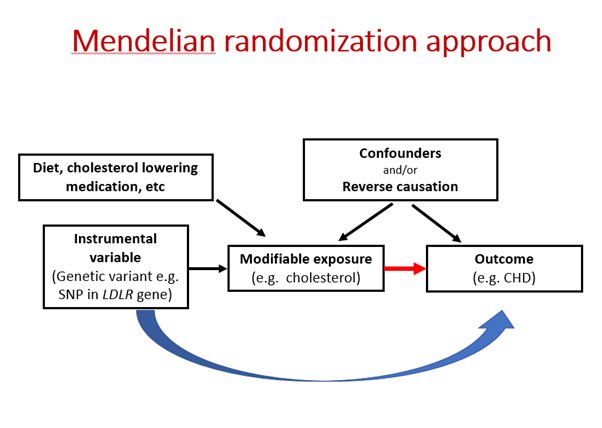
4/n Of course the genetic variants could have influences on CHD not thru LDL cholesterol (this is horizontal pleiotropy, discussed later in the webinar) and the “exposures” could have other effects (eg if you lower LDL thru starvation that will have other effects not thru LDL)
5/n Whether the assumption is reasonable to make depends on other evidence supporting (or undermining) its validity. Thus in the comic-book example of cutting off a leg to lower BMI the effect of amputation on BMI would not be mimicked by genetic variation
6/n The genetic variants influence BMI through a range of mechanisms involving energy balance (food intake, energy expenditure and storage) and thus largely (but not wholly) model how external interventions would modify BMI and downstream risks of e.g. CHD
7/n This speaks to the dispute between @MiguelHernan & @yudapearl on attributing cause to well-defined interventions or to states like BMI and blood pressure ncbi.nlm.nih.gov/pubmed/18695657 (where amputation raised as an objection) & ftp.cs.ucla.edu/pub/stat_ser/r…
8/n As usual, with biological knowledge & common sense the stark dichotomy is navigable & for a pragmatic epidemiology (or indeed epistemology) what you learn about states (e.g. BMI, blood pressure, LDL) feeds into evidence about which interventions are likely to be beneficial
9/n (spoiler alert: amputation for obesity management and exsanguination for hypertension are unlikely to help .. now who thought they would?)
10/n Back to the webinar: at 16.00 we see how pregnant women at antenatal clinics were expected to understand MR, helped by a picture of what looks worryingly like Margaret Thatcher

11/n At 20.00 the instrumental variables (IV) assumptions 1-3 outlined; 1 can be tested but 2 and 3 merely subjected to sensitivity analyses. Proposing a test for IV2 or IV3 is sometimes done, and either deserves a Nobel prize, or is wrong ..
12/n .. so far they have all been wrong and the invite to Stockholm for e.g. @mvholmes hasn't arrived yet 😉jamanetwork.com/journals/jamac…
13/n A frequently seen problem in MR studies is adjusting for the intermediate risk factor (sometimes presented as a "test" of the exclusion restriction) - this both doesn't work AND introduces confounding of the genotype-outcome association (at 20.58)

14/n To generate effect estimates (e.g. risk of CHD increases by X per unit change in LDL) from MR additional assumptions are required – they are less widely recognised in the MR literature than IV1-3, and are collectively sometimes known as IV4 assumptions (at 24.20)
15/n These have been helpfully reviewed by Sonja Swanson @ja_labrecque_ @_MiguelHernan et al at various places (eg ncbi.nlm.nih.gov/pubmed/28379526 ncbi.nlm.nih.gov/pubmed/28590373
link.springer.com/content/pdf/10… )
link.springer.com/content/pdf/10… )
16/n Sometimes it has been suggested that IV4 violations are a “dirty secret” and the implications are so serious that this “changes everything you learned” etc
17/n But such tweets may be a trifle over-excited; such violations would be expected to differ across the often many genetic instruments, and then would be revealed by the sensitivity analyses, which essentially interrogate the degree of heterogeneity of the IV effect estimates
18/n Furthermore, violation of the IV4 assumptions would lead to differences in variance of the intermediate phenotype, or outcome, or both, across levels of the genetic IVs (except with implausible perfect cross-over situations)
19/n for application of this exploration of variance in the RCT setting, see excellent paper by Jordi Cortes, @stephensenn et al f1000research.com/articles/7-30/…
20/n R.A. Fisher (in a 1938 letter) highlighted this issue with respect to the randomized studies he had introduced & in his letter said criticisms on the basis of interactions had come mostly from those who had “lack of contact with the practical experimental situation”
21/n this resonates today with sweeping statements regarding the impact of such (generally not demonstrated) potential violations in MR (a recent exception, hopefully heralding a more data-based approach, is Sonja Swanson and @ja_labrecque excellent ncbi.nlm.nih.gov/pubmed/30239571 )
22/n Interpretation of IV estimates in MR at 30.20, with many caveats

23/n With all these caveats why generate IV estimates at all? (at 35.50) Interpreted appropriately they carry some information, and most importantly are the basis of many of the sensitivity analyses for MR
24/n MR is sometimes used to infer the effects of diseases on outcomes, as in the below, on schizophrenia having an apparent causal effect on cannabis use (at 45.25)

25/n but MR studies as they have been done to date cannot do this - the interpretation is to the effects of the liability to the disease, not to the disease itself

26/n Findings from MR studies should be triangulated with evidence from other study designs to inform appropriate causal inference (at 47.45), examples of such triangulation involving MR are in ncbi.nlm.nih.gov/pubmed/28108528 and box 3 of academic.oup.com/ije/article/45…
27/n More on MR at the conference in Bristol 17th-19th July 2019 mendelianrandomization.org.uk