,
11 tweets,
5 min read
Read on Twitter
1/10
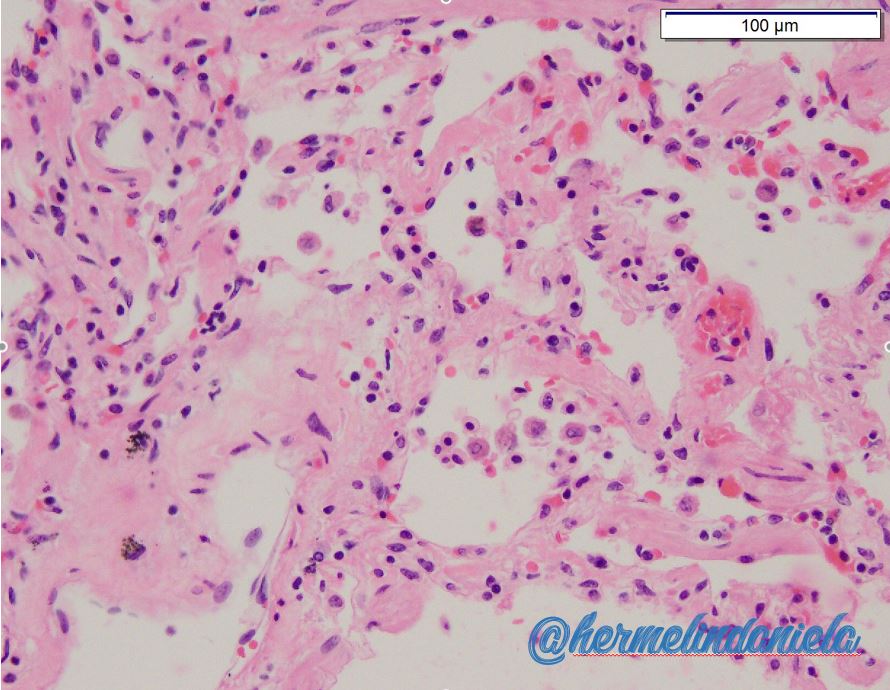
These are the lungs of a patient who died while receiving a PLT transfusion. He developed sudden respiratory distress and did not respond to O2 support. Lungs compressed by 3000 mL of transudative pleural fluid. Notice the increased neutrophils #PathTweetorial
These are the lungs of a patient who died while receiving a PLT transfusion. He developed sudden respiratory distress and did not respond to O2 support. Lungs compressed by 3000 mL of transudative pleural fluid. Notice the increased neutrophils #PathTweetorial
2/10
The above clinical scenario along with the histologic findings is consistent with which type of transfusion reaction?
#Blooducation #TransfusionReaction
The above clinical scenario along with the histologic findings is consistent with which type of transfusion reaction?
#Blooducation #TransfusionReaction
3/10
Yes, the histologic findings and clinical history is consistent with Transfusion-Related Acute Lung Injury (TRALI). Second to TACO, it is the most common cause of transfusion-related morbidities and fatalities. What causes it?
#Blooducation
Yes, the histologic findings and clinical history is consistent with Transfusion-Related Acute Lung Injury (TRALI). Second to TACO, it is the most common cause of transfusion-related morbidities and fatalities. What causes it?
#Blooducation
4/10
The working pathogenesis of TRALI is the passive transfusion of anti-neutrophil/anti-HLA or neutrophil priming substances (bioactive lipids) in the transfused unit. Ab-mediated or not, the mechanism leads to increased pulmonary capillary permeability and pulmonary edema
The working pathogenesis of TRALI is the passive transfusion of anti-neutrophil/anti-HLA or neutrophil priming substances (bioactive lipids) in the transfused unit. Ab-mediated or not, the mechanism leads to increased pulmonary capillary permeability and pulmonary edema

5/10
You got it! If the criteria for TRALI occurs during or within 6-hours after completion of the transfusion, the transfusion can be suspected. The additional criteria for TRALI includes noncardiogenic pulmonary edema, bilateral lung infiltrates on chest radiograph, and ALI 👇🏽
You got it! If the criteria for TRALI occurs during or within 6-hours after completion of the transfusion, the transfusion can be suspected. The additional criteria for TRALI includes noncardiogenic pulmonary edema, bilateral lung infiltrates on chest radiograph, and ALI 👇🏽

6/10
To further "prove" TRALI and the presence of neutrophils, CD15 was applied to the lung sections. It strongly showed the capillaries “filled” with neutrophils that clearly marginate into the interstitial and alveolar spaces.
To further "prove" TRALI and the presence of neutrophils, CD15 was applied to the lung sections. It strongly showed the capillaries “filled” with neutrophils that clearly marginate into the interstitial and alveolar spaces.



7/10
🤔Did you know?
☑️The adult cardiac output pumps 7,200 L of blood through the pulmonary circulation in 24 hours.
☑️With each liter, 10^9 neutrophils travel through the pulmonary microcirculation
☑️Pulmonary capillaries are 2-15 um in diameter, a neutrophil is 6-8 um
🤔Did you know?
☑️The adult cardiac output pumps 7,200 L of blood through the pulmonary circulation in 24 hours.
☑️With each liter, 10^9 neutrophils travel through the pulmonary microcirculation
☑️Pulmonary capillaries are 2-15 um in diameter, a neutrophil is 6-8 um
8/10
You can imagine that if "trapped" primed and activated, neutrophils in the pulmonary microvasculature could really lead to endothelial damage/leakiness and massive pulmonary edema.
You can imagine that if "trapped" primed and activated, neutrophils in the pulmonary microvasculature could really lead to endothelial damage/leakiness and massive pulmonary edema.


9/ 10
Can we prevent TRALI? Management of TRALI is supportive, but TRALI mitigation strategies minimize the preparation of high plasma-volume components from donors immunized with leukocyte antigens (previously pregnant women) 🤱🏽
Can we prevent TRALI? Management of TRALI is supportive, but TRALI mitigation strategies minimize the preparation of high plasma-volume components from donors immunized with leukocyte antigens (previously pregnant women) 🤱🏽

10/10
To learn more about this important topic, please read this amazing article by Dr. Beth Shaz Transfusion-related acute lung injury: from bedside to bench and back bloodjournal.org/content/117/5/…. Have you experienced a patient with TRALI? 🙏🏽Please add to the conversation below.
To learn more about this important topic, please read this amazing article by Dr. Beth Shaz Transfusion-related acute lung injury: from bedside to bench and back bloodjournal.org/content/117/5/…. Have you experienced a patient with TRALI? 🙏🏽Please add to the conversation below.