,
9 tweets,
7 min read
Read on Twitter
1/x We asked @millimaninsight to analyze the financial impact of point of sale (POS) rebates in Medicare Part D, following on the HHS RFI on this notion. Once you start reading, you won’t be able to put this one down! s3.amazonaws.com/public-inspect… drugpricinglab.org/our-work/impac…
2/x. POS rebates = drug costs for pts reduced by the rebate negotiated by the PBMs, not how done today. POS rebates are also different from eliminating rebates as @SecAzar just proposed, discussed by @dusetzinaS and me @JAMA_current jamanetwork.com/journals/jama/…
3/x The analysis broke down POS rebates by drug category using data from @ssrhealth so we could see how they might affect beneficiaries with different conditions, and which categories of drugs are responsible for the largest differences in a rebate v non-rebate scenario.
4/x New idea: Hold the @phrma members’ contribution to Part D constant using a separate TrOOP accumulator for @phrma members’ contributions. Otherwise b/c patient TROOP accumulation falls @phrmas does. @millimaninsight models with 100% POS rebate it generates +$50B in 10 yrs. 
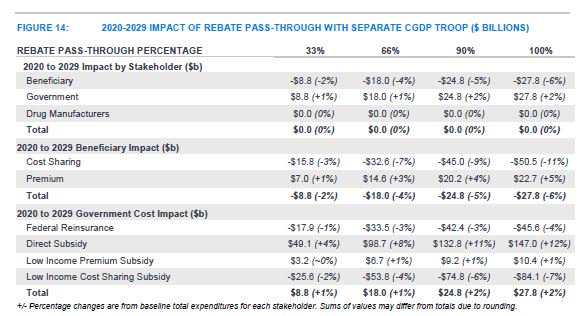
5/x Shifting to POS rebates raises costs for just over half of beneficiaries (premiums rise more than their OOP savings). Average increase around $5/month. But for top quartile beneficiaries, savings are 3-8 times as much.

6/x A lot of the action is in a few drug classes – POS rebates isolated to diabetes would cost Medicare $25B over 10 years unless they also use the alternative TrOOP approach that is presented. Doing so reduces the cost of diabetes specifci to $8B. Oncology < $3B.


7/x Flipping the scenario around, patients with these conditions stand to gain a lot. Under 100% POS rebates and the new TrOOP approach, diabetics see their costs (premium + OOP) fall $52/month; cancer patients $19.

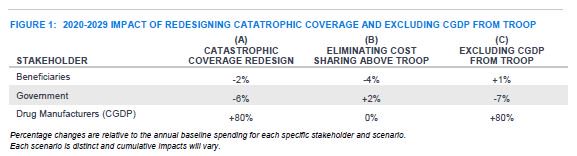
8/x We also asked @millimaninsight to model impact of the President’s budget proposal including removing the @phrma members’ contributions in the coverage gap to TrOOP, shifting reinsurance off of Medicare and onto the Part D plans, and eliminating OOP in catastrophic.
9/x You made it to the end of the tweetstorm on an actuarial analysis of a policy in the RFI stage 👏👏. You can read more about why this matters within the Part D program in an article from @DusetzinaS @contirena1 Nancy Yu and me from @JAMAInternalMed jamanetwork.com/journals/jamai…