Acute allergic-like reactions to intravascular iodinated contrast: Who's at risk and how do you reduce the risk?
A #TWEETORIAL for #radres and referring clinicians alike
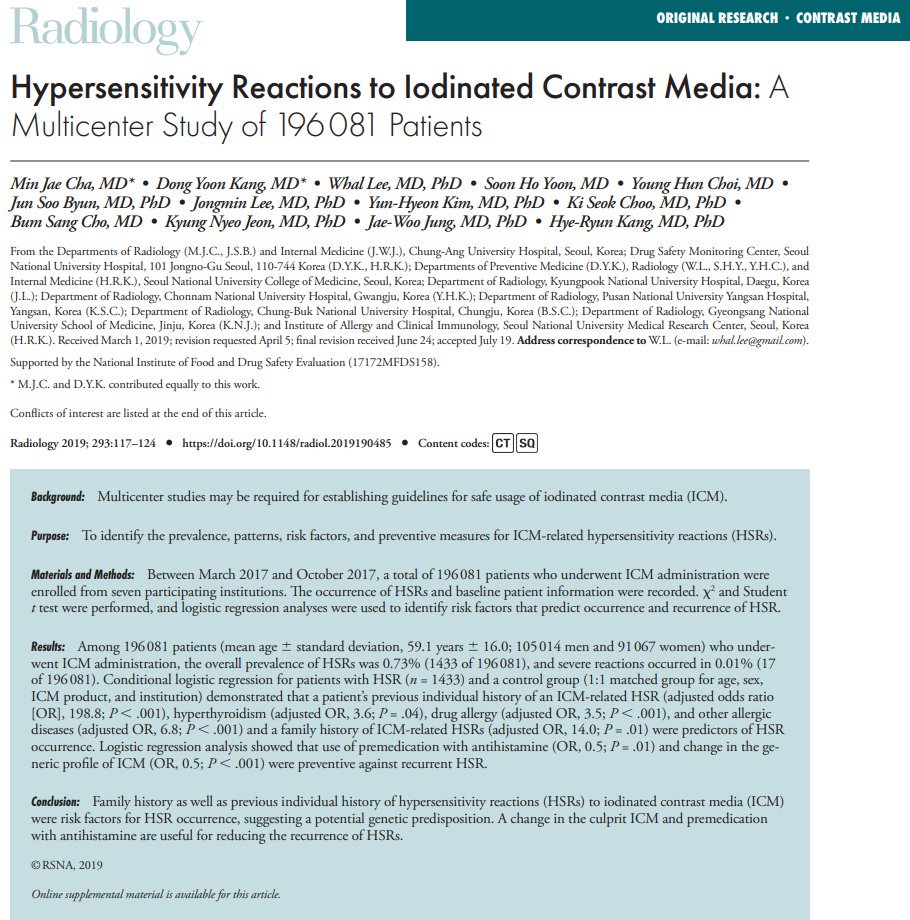
Inspired by a recent paper in @Radiology_RSNA by Cha MJ, Kang DY, et al. pubs.rsna.org/doi/10.1148/ra… 1/40ish
A #TWEETORIAL for #radres and referring clinicians alike
Inspired by a recent paper in @Radiology_RSNA by Cha MJ, Kang DY, et al. pubs.rsna.org/doi/10.1148/ra… 1/40ish
@radiology_rsna First some background:
DEFINING ALLERGIC-LIKE REACTIONS
Which of the following is most likely to represent an allergic-like contrast reaction?
DEFINING ALLERGIC-LIKE REACTIONS
Which of the following is most likely to represent an allergic-like contrast reaction?
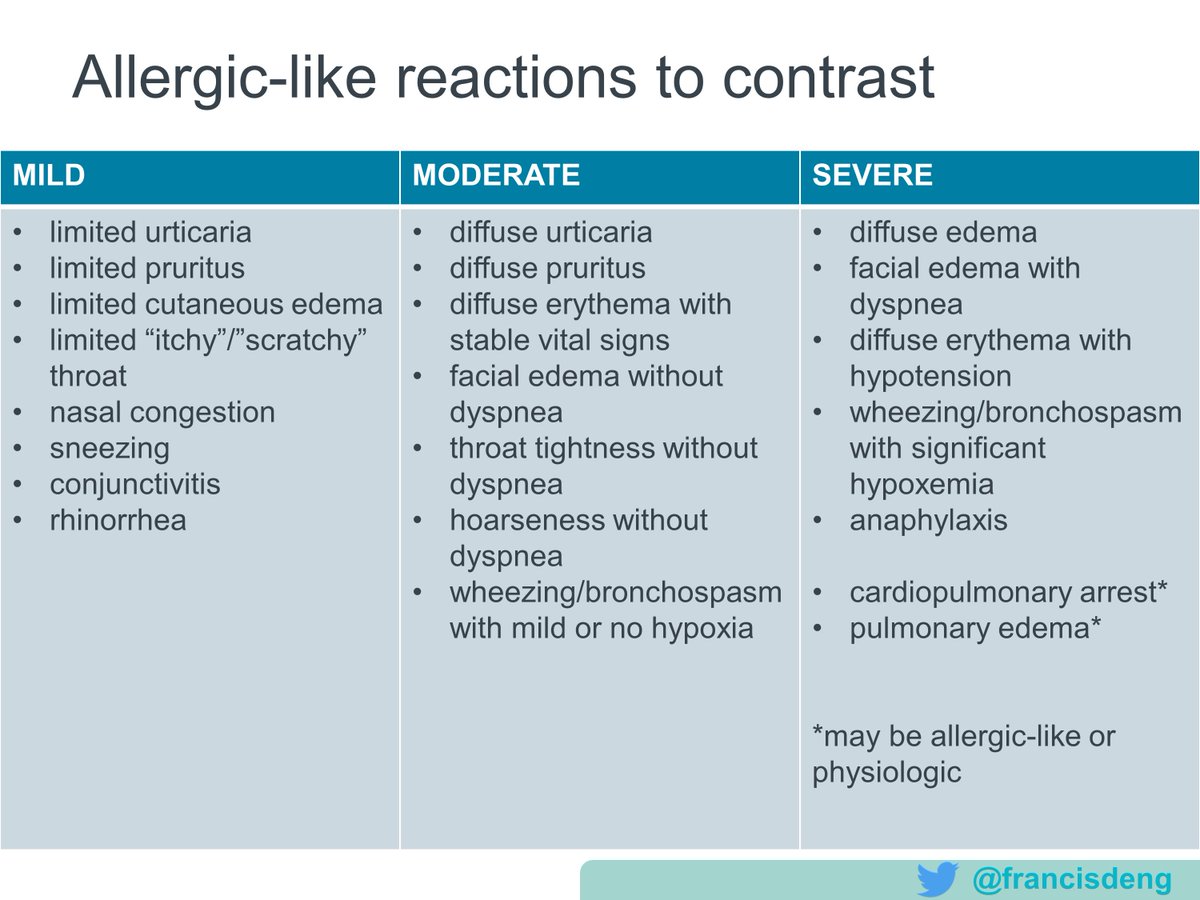
@radiology_rsna Not all acute adverse reactions to contrast are allergic-like. Allergic-like reactions include hives, pruritus, nasal congestion, wheezing, anaphylaxis. Reactions are subcategorized by severity.
Mild: self-limited
Moderate: commonly requiring treatment
Severe: life-threatening
Mild: self-limited
Moderate: commonly requiring treatment
Severe: life-threatening
@radiology_rsna Here is a list of allergic-like reactions from the American College of Radiology Manual on Contrast Media, which were the focus of the study by Cha et al. They called them hypersensitivity reactions.
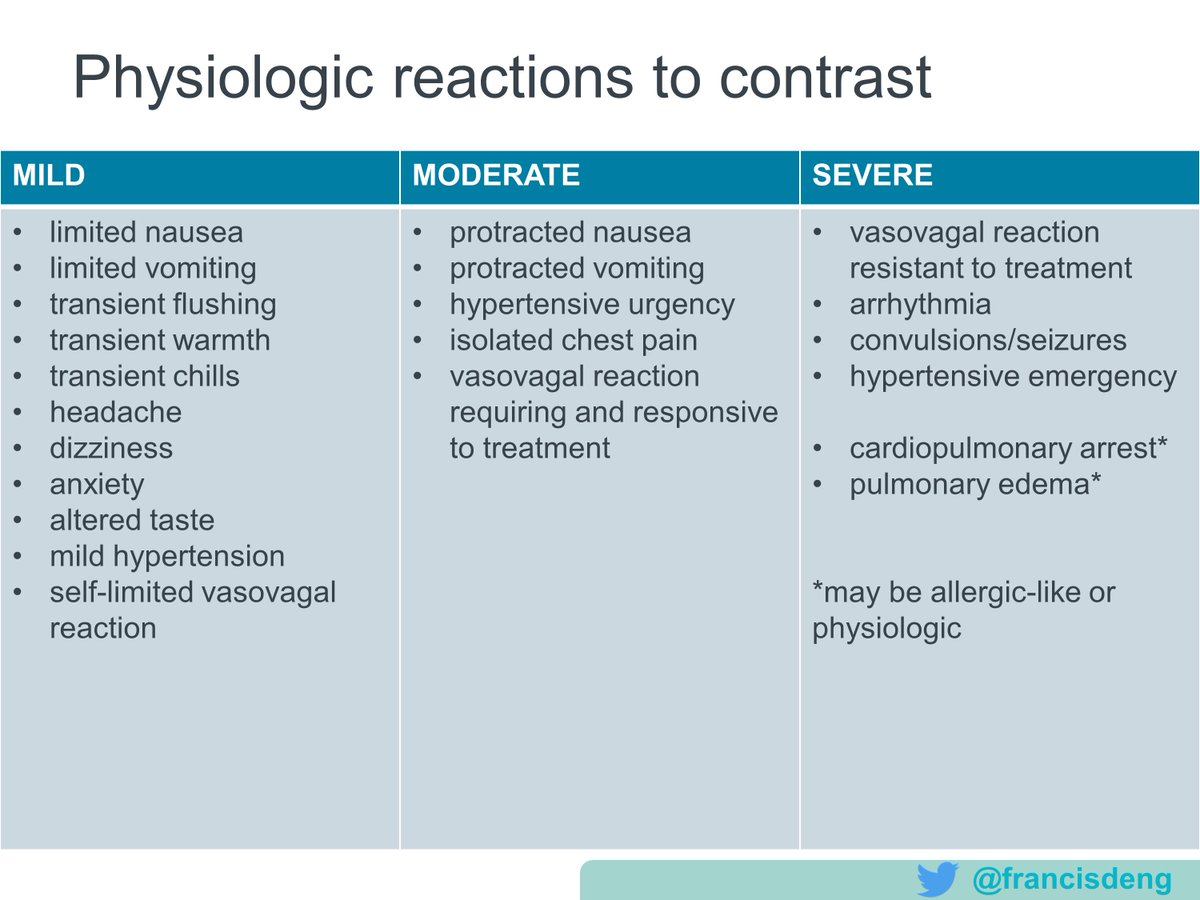
@radiology_rsna Ideally allergic-like reactions should be distinguished from physiologic reactions, although Cha et al "also closely monitored" reports of select physiologic reactions because of overlap in clinical practice.
Here is a list of physiologic reactions.
Here is a list of physiologic reactions.
@radiology_rsna Why does the distinction matter?
1) Patients with allergic-like reactions may require/benefit from premedication prior to future exposures, while those with physiologic reactions do not.
1) Patients with allergic-like reactions may require/benefit from premedication prior to future exposures, while those with physiologic reactions do not.
@radiology_rsna Many patients who received intravascular high osmolality contrast, used decades ago, had physiologic reactions related to osmotoxicity. These should not prevent a patient today from receiving low osmolality contrast agents, which have much lower rates of such reactions.
@radiology_rsna DEFINING ACUTE
When do these reactions occur?
Nearly all life-threatening reactions happen immediately, within 20 minutes of contrast administration.
When do these reactions occur?
Nearly all life-threatening reactions happen immediately, within 20 minutes of contrast administration.
@radiology_rsna Delayed reactions can occur up to a week after, usually a few hours to days. Fortunately, delayed reactions are most commonly hives or other rash, rarely serious. After a mild delayed cutaneous reaction, preventative measures are not advocated for future contrast exposures.
@radiology_rsna DEFINING INTRAVASCULAR IODINATED CONTRAST
Which contrast agents are we talking about?
These days we use nonionic, tri-iodinated benzene rings with three variable side chains, in solutions that are 1-3x serum osmolality (called "low osmolality").
Which contrast agents are we talking about?
These days we use nonionic, tri-iodinated benzene rings with three variable side chains, in solutions that are 1-3x serum osmolality (called "low osmolality").
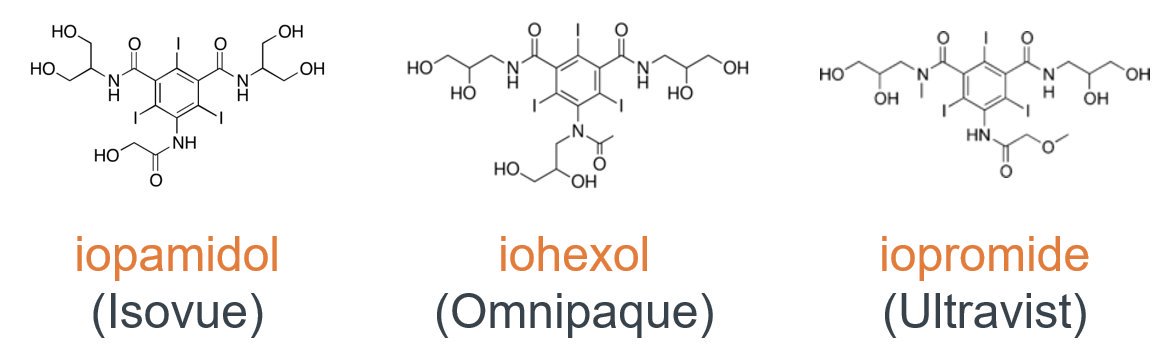
@radiology_rsna Some iodinated contrast generic names:
iopamidol
iopromide
iohexol
ioversol
io𝘥𝘪xanol (a 𝘥𝘪mer and iso-osmolal)
ioxilan
iobitridol
iomeprol
iopamidol
iopromide
iohexol
ioversol
io𝘥𝘪xanol (a 𝘥𝘪mer and iso-osmolal)
ioxilan
iobitridol
iomeprol
@radiology_rsna Why do contrast names matter? When documenting a contrast reaction, one should specify the culprit agent (we'll see why later).
TRIVIA: Which of these is an iodinated contrast agent brand name (included in this paper)?
TRIVIA: Which of these is an iodinated contrast agent brand name (included in this paper)?
@radiology_rsna Optiray is ioversol. Optimark is the gadolinium-based contrast agent gadoversetamide (being phased out). The other two are Pokémon.
The point is, brand names are hard. In contrast (get it?), the generic names for current intravascular iodinated agents all start with "io-"!
The point is, brand names are hard. In contrast (get it?), the generic names for current intravascular iodinated agents all start with "io-"!


@radiology_rsna Side note 1: An astute reader knows diatrizoate [Gastrografin] is also an iodinated contrast agent, but these days it is only administered via GI/GU routes given its high osmolality.
@radiology_rsna Side note 2: These agents often have a number, eg, Isovue 370. That's concentration of iodine (mg/ml) of the product. This is not so important as there is no clear relationship between reaction risk and iodine concentration within the commercially available range of each agent.
@radiology_rsna IMPORTANT‼️: Do not call iodinated contrast agents "iodine". There is no such thing as an "iodine" allergy. Nor is there allergenic overlap with povidone-iodine (Betadine), iodized table salt, radioiodine, shellfish or other seafood.
@radiology_rsna Also realize that documenting only "contrast allergy" is nonspecific and may hamper your patient from getting a different type of contrast-enhanced study in the future, like gadolinium-based contrast for MRI.
@radiology_rsna RISK OF REACTION
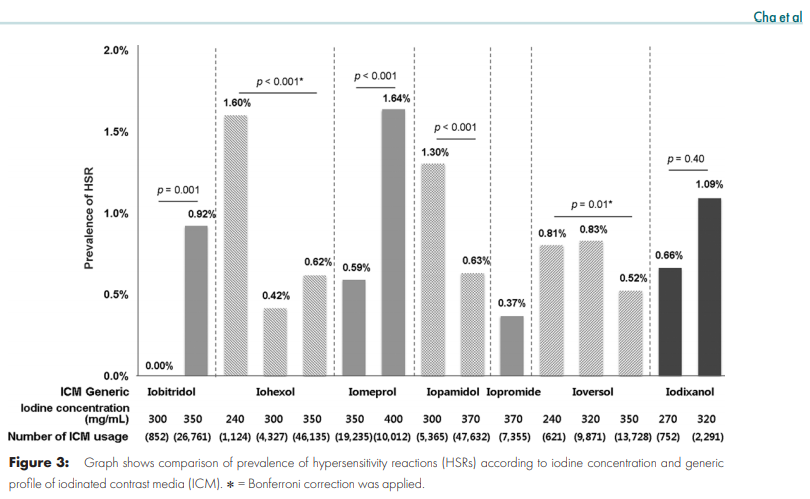
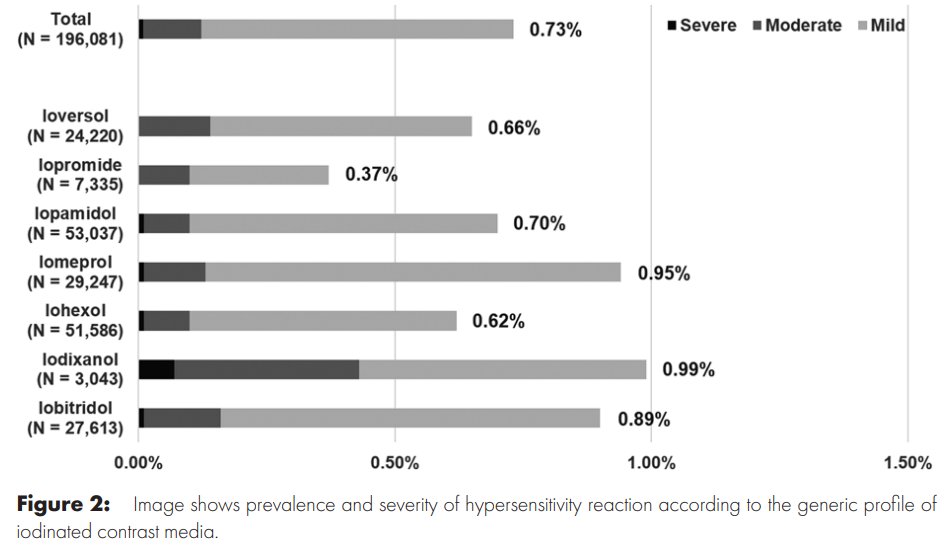
Cha et al. studied a registry of 196,081 patients who had contrast-enhanced CT at 7 institutions in Korea over 8 months. Here's some rounded figures based on this and other papers, which triangulate the teaching points.
Cha et al. studied a registry of 196,081 patients who had contrast-enhanced CT at 7 institutions in Korea over 8 months. Here's some rounded figures based on this and other papers, which triangulate the teaching points.
@radiology_rsna Which of the following is closest to the rate of allergic-like reactions upon exposure to intravascular iodinated contrast?
@radiology_rsna The prevalence of allergic-like reactions to (modern, low osmolality) intravascular iodinated contrast is less than 1% (about 1-7 in 1000 depending on your source).
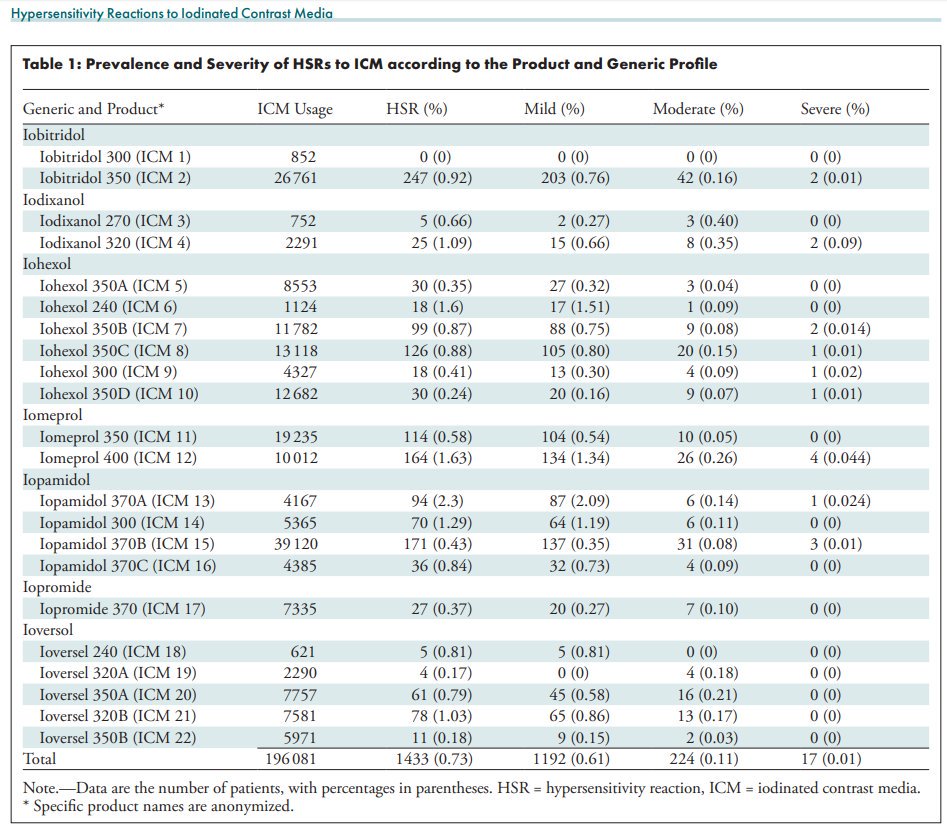
@radiology_rsna Of allergic-like reactions to iodinated contrast, most (70-90%) are mild, some (10-20%) are moderate, and rare ones (1-5%) are severe.
@radiology_rsna The strongest risk factor for an allergic-like reaction to iodinated contrast is a prior personal history of such, even though most people who have a reaction never had one before that.
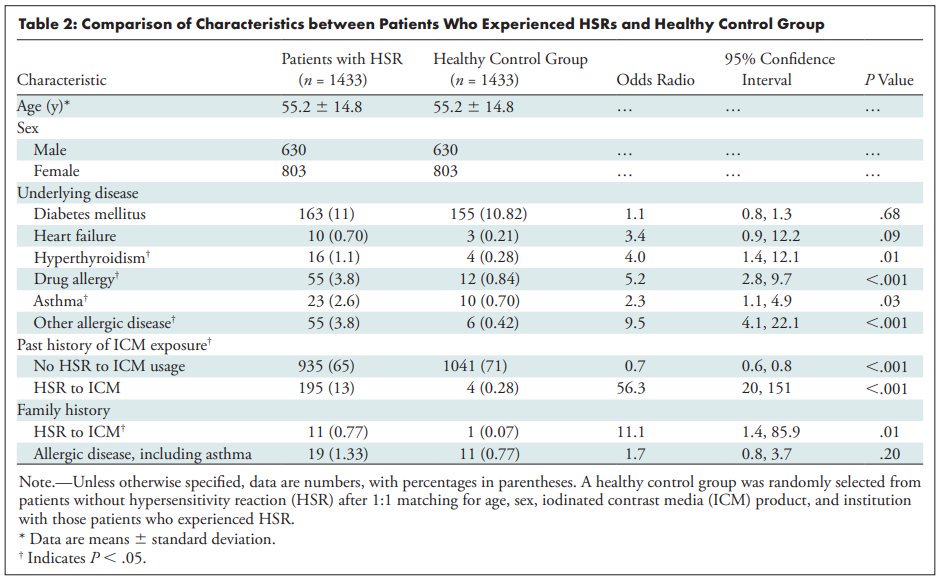
@radiology_rsna Other risk factors include family history of iodinated contrast reaction; female sex; and personal history of other allergies or asthma.
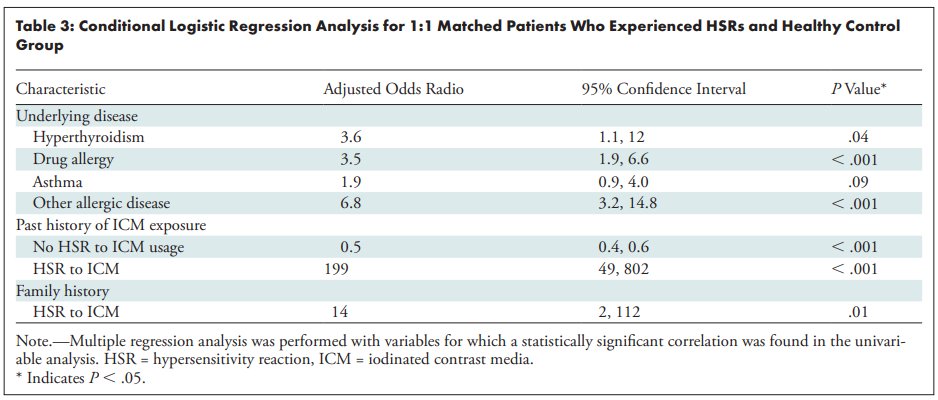
@radiology_rsna In current practice, however, the PRIMARY risk factor that is considered when deciding whether to undertake preventive measures is the prior history of an allergic-like reaction.
@radiology_rsna The SEVERITY of that reaction is also important when determining the strength of preventive measures to undertake. Why? Most recurrent reactions have a severity similar to that of the index reaction.
See Davenport et al. in Radiology 2009 dx.doi.org/10.1148/radiol…
See Davenport et al. in Radiology 2009 dx.doi.org/10.1148/radiol…
@radiology_rsna Is skin testing usually helpful for predicting who will have a contrast reaction?
@radiology_rsna TWEETORIAL to be continued after a trans-Atlantic flight!
@radiology_rsna The term "allergic-like" is used because the presentation is similar to other drug allergies, and histamine and other mediators are released from granulocytes, but it's usually not IgE-mediated. Skin testing does not reliably predict reactions.
See doi.org/10.1016/j.jaip…
See doi.org/10.1016/j.jaip…
@radiology_rsna Is a test dose/injection recommended for predicting who will have a contrast reaction?
@radiology_rsna Intravenous pretesting (test injection) is not predictive of contrast reaction to a standard injection. They are not recommended to screen for patients at high risk for contrast reaction.
See Yamaguchi et al. Radiology 1991 doi.org/10.1148/radiol…
See Yamaguchi et al. Radiology 1991 doi.org/10.1148/radiol…
@radiology_rsna PREVENTIVE MEASURES
In patients who had an allergic-like reaction to iodinated contrast, there are three preventive measures to consider prior to another exam:
1) Avoidance
2) Premedication
3) Agent switching
In patients who had an allergic-like reaction to iodinated contrast, there are three preventive measures to consider prior to another exam:
1) Avoidance
2) Premedication
3) Agent switching
@radiology_rsna 1) The only surefire way to prevent an adverse drug reaction is to not administer the drug. Consider a noncontrast exam or alternative imaging modalities, but you must also weigh the diagnostic value lost. Consult a radiologist!
@radiology_rsna 2) Premedication with corticosteroids and/or antihistamines reduces the risk of acute allergic-like reactions to iodinated contrast. The benefit should be weighed against the risk, which includes delay in diagnosis and extended length of stay.
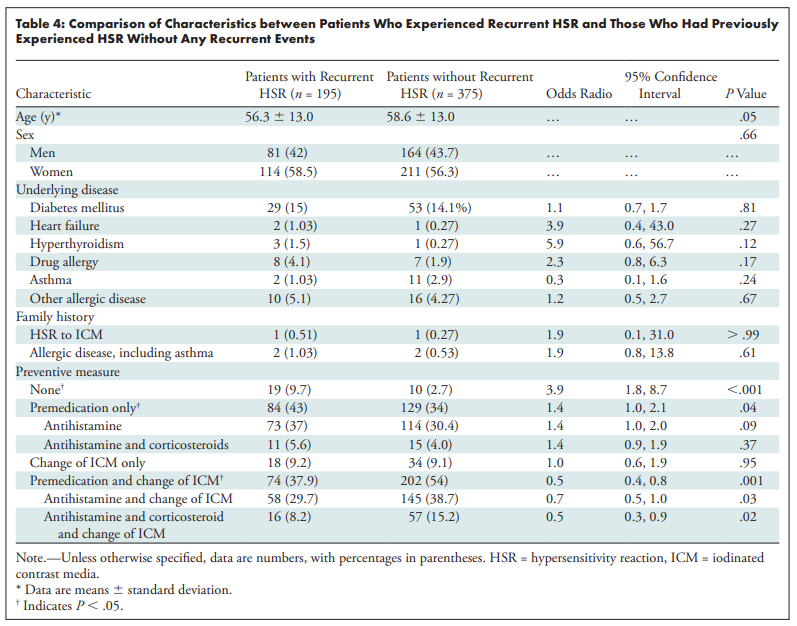
@radiology_rsna 3) Changing the contrast agent to a different one from the same class (eg, iodixanol rather than iopamidol) reduces the likelihood of a recurrent allergic-like reaction, as effectively as premedication or more.

@radiology_rsna The agent-switching strategy is only possible if the original culprit was known and another agent is available.
This is why contrast names are important. If you know the culprit agent, don't pick the general entry your EHR offers like "Iodinated Contrast- Oral and Iv Dye".
This is why contrast names are important. If you know the culprit agent, don't pick the general entry your EHR offers like "Iodinated Contrast- Oral and Iv Dye".
@radiology_rsna Case 1
Pt with hx hives+hypoxia+hypotension after iopamidol; needs CT in ED: ?appendicitis. What's most reasonable:
A)CT now w rectal diatrizoate, IV iopamidol
B)CT now w rectal barium, w/o IV
C)5h premed, CT w rectal+IV diatrizoate
D)13h premed, CT w rectal barium, IV ioversol
Pt with hx hives+hypoxia+hypotension after iopamidol; needs CT in ED: ?appendicitis. What's most reasonable:
A)CT now w rectal diatrizoate, IV iopamidol
B)CT now w rectal barium, w/o IV
C)5h premed, CT w rectal+IV diatrizoate
D)13h premed, CT w rectal barium, IV ioversol
@radiology_rsna Case 2
Elderly inpt w remote hx of "feeling hot" and "throwing up" following "IVP dye" in 1980. CT needed: ?acute PE. What do you do before CT pulm angio?
A) Test injection (small IV dose)
B) 13h premedication regimen
C) Allergy consult: ?skin testing
D) Nothing special
Elderly inpt w remote hx of "feeling hot" and "throwing up" following "IVP dye" in 1980. CT needed: ?acute PE. What do you do before CT pulm angio?
A) Test injection (small IV dose)
B) 13h premedication regimen
C) Allergy consult: ?skin testing
D) Nothing special
@radiology_rsna Case 3A
Pt has throat scratchiness + sneezing 15 min after 90 mL IV iopamidol 370 mg iodine/mL. Sx resolve spontaneously within 15 min. What allergy entry do you add?
A)Iopamidol
B)Iodinated Contrast- Oral and Iv Dye
C)Iodine and Iodine-containing Substances
D)None
Pt has throat scratchiness + sneezing 15 min after 90 mL IV iopamidol 370 mg iodine/mL. Sx resolve spontaneously within 15 min. What allergy entry do you add?
A)Iopamidol
B)Iodinated Contrast- Oral and Iv Dye
C)Iodine and Iodine-containing Substances
D)None
@radiology_rsna Case 3B
In the same patient as above, which of the following is the best severity of reaction to document?
In the same patient as above, which of the following is the best severity of reaction to document?
@radiology_rsna MY ANSWERS
Case 1: The patient had a severe allergic-like reaction, a relative contraindication to reexposure to iodinated contrast. An alternative technique without iodinated contrast (B) (or US or MR) is appropriate and avoids diagnostic delay and risk of breakthrough reaction.
Case 1: The patient had a severe allergic-like reaction, a relative contraindication to reexposure to iodinated contrast. An alternative technique without iodinated contrast (B) (or US or MR) is appropriate and avoids diagnostic delay and risk of breakthrough reaction.
@radiology_rsna Case 1 cont:
A) Without premedication or agent switching, there is an unacceptable risk of recurrent reaction -- first, do no harm.
D) With a long premedication regimen, the delay in diagnosis increases the risks of appendicitis complications (but balance varies by scenario)
A) Without premedication or agent switching, there is an unacceptable risk of recurrent reaction -- first, do no harm.
D) With a long premedication regimen, the delay in diagnosis increases the risks of appendicitis complications (but balance varies by scenario)
@radiology_rsna Case 1 cont:
C) An aggressive clinician and patient might accept the risk of breakthrough reaction despite prior severe reaction (depends on local standards) but I tipped the scale: diatrizoate (Gastrografin) shouldn't be administered IV due to higher risk of adverse reactions.
C) An aggressive clinician and patient might accept the risk of breakthrough reaction despite prior severe reaction (depends on local standards) but I tipped the scale: diatrizoate (Gastrografin) shouldn't be administered IV due to higher risk of adverse reactions.
@radiology_rsna Case 2:
The patient most likely had a mild physiologic reaction to a high osmolality contrast agent. They would not be regarded as high risk for allergic-like reaction to low osmolality contrast. No special preventive action is needed (D), avoiding diagnostic delay.
The patient most likely had a mild physiologic reaction to a high osmolality contrast agent. They would not be regarded as high risk for allergic-like reaction to low osmolality contrast. No special preventive action is needed (D), avoiding diagnostic delay.
@radiology_rsna Case 2 cont:
A) The use of test injections is not evidence-based.
B) A full premedication regimen would only be indicated for prior allergic-like reaction and if the diagnosis does not need to be made on an emergency basis.
A) The use of test injections is not evidence-based.
B) A full premedication regimen would only be indicated for prior allergic-like reaction and if the diagnosis does not need to be made on an emergency basis.
@radiology_rsna Case 2 cont:
C) An allergist might help you sort out the story to see if it seemed allergic-like, but skin testing for contrast media is not currently an evidence-based practice
C) An allergist might help you sort out the story to see if it seemed allergic-like, but skin testing for contrast media is not currently an evidence-based practice
@radiology_rsna Case 3:
My assessment is that the patient had a mild, self-limited allergic-like reaction to iodinated contrast. The culprit and reaction should be documented in detail, including the name of the agent when it is known.
Case 3A: answer is A
Case 3B: answer is A
My assessment is that the patient had a mild, self-limited allergic-like reaction to iodinated contrast. The culprit and reaction should be documented in detail, including the name of the agent when it is known.
Case 3A: answer is A
Case 3B: answer is A
@radiology_rsna Thanks for reading to the end of my first tweetorial. If you want to see more, please RT/like the top tweet. Criticism also welcome.
Maybe in a future tweetorial, we'll dive into the evidence on premedication + agent-switching. How much benefit? What's the risk of breakthrough?
Maybe in a future tweetorial, we'll dive into the evidence on premedication + agent-switching. How much benefit? What's the risk of breakthrough?
@radiology_rsna @threadreaderapp unroll