1/
ERYTHEMA MULTIFORME – a #dermatology #tweetorial/#medthread!
#MedEd #FOAMEd #dermatologia #dermtwitter #medtwitter #derm pc: @dermnetnz
Let's warm up with a question for all y'all tweeps out there!
What is the most common trigger for erythema multiforme (EM) in adults?
ERYTHEMA MULTIFORME – a #dermatology #tweetorial/#medthread!
#MedEd #FOAMEd #dermatologia #dermtwitter #medtwitter #derm pc: @dermnetnz
Let's warm up with a question for all y'all tweeps out there!
What is the most common trigger for erythema multiforme (EM) in adults?
2/
EM is an immunologic syndrome usually triggered by infection in adults. We usually consider HSV and mycoplasma. A simple history for cold sores or genital ulcers can be telling, but mycoplasma can go undetected symptomatically.
What primary lesions do you expect in EM?
EM is an immunologic syndrome usually triggered by infection in adults. We usually consider HSV and mycoplasma. A simple history for cold sores or genital ulcers can be telling, but mycoplasma can go undetected symptomatically.
What primary lesions do you expect in EM?
3/
EM is usually made up of papular (raised) targets. Pic1 is of EM; you can see the 3 zones in a typical target (red rim, then white, then red center). Versus SJS/TEN (pic2), where macular targetoid (2 zones of red rim, dusky center & flat).
2nd photo: my.clevelandclinic.org/health/disease…
EM is usually made up of papular (raised) targets. Pic1 is of EM; you can see the 3 zones in a typical target (red rim, then white, then red center). Versus SJS/TEN (pic2), where macular targetoid (2 zones of red rim, dusky center & flat).
2nd photo: my.clevelandclinic.org/health/disease…


4/
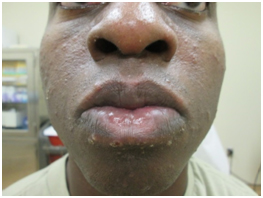
Aside from the primary lesion, distribution can be helpful with EM. Acral involvement is common, and there can be mucosal involvement (photo). In fact, mucosal involvement means you are dealing with EM Major, whereas no (or very mild) mucosal disease = EM Minor.
Aside from the primary lesion, distribution can be helpful with EM. Acral involvement is common, and there can be mucosal involvement (photo). In fact, mucosal involvement means you are dealing with EM Major, whereas no (or very mild) mucosal disease = EM Minor.

5/
EM and SJS can be tough to distinguish. In fact, only 15-20 years ago, it was all thought to be on a spectrum (where EM could --> SJS). However, they are now considered to be two different disease processes, and if a patient has EM, he/she shouldn’t progress to SJS/TEN.
EM and SJS can be tough to distinguish. In fact, only 15-20 years ago, it was all thought to be on a spectrum (where EM could --> SJS). However, they are now considered to be two different disease processes, and if a patient has EM, he/she shouldn’t progress to SJS/TEN.
6/
So how should we treat EM? Treating the underlying cause is most important. However, what if we can’t find a trigger? Supportive care is the name of the game. While magic mouthwash and topical steroids can help, systemic steroids are often used to hasten improvement.
7
So how should we treat EM? Treating the underlying cause is most important. However, what if we can’t find a trigger? Supportive care is the name of the game. While magic mouthwash and topical steroids can help, systemic steroids are often used to hasten improvement.
7
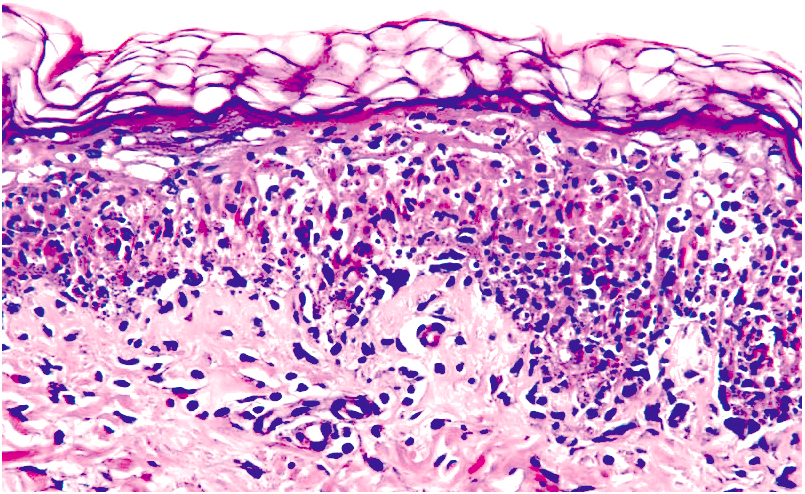
7/
A quick #dermpath note. EM usually has interface dermatitis with dyskeratotic keratinocytes. Importantly, EM can be difficult to distinguish from SJS or fixed drug eruption pathologically so the clinical exam is paramount to the accurate diagnosis.
pc: pathologyoutlines.com/topic/skinnont…
A quick #dermpath note. EM usually has interface dermatitis with dyskeratotic keratinocytes. Importantly, EM can be difficult to distinguish from SJS or fixed drug eruption pathologically so the clinical exam is paramount to the accurate diagnosis.
pc: pathologyoutlines.com/topic/skinnont…
8/
One last topic related to EM – the differential diagnosis. Perhaps most commonly mistaken with EM is hand foot mouth disease (HFMD). HFMD should be vesicular on a red base, & EM I think of as papules. However, intense inflammation can also vesiculate, so it can be confusing!
One last topic related to EM – the differential diagnosis. Perhaps most commonly mistaken with EM is hand foot mouth disease (HFMD). HFMD should be vesicular on a red base, & EM I think of as papules. However, intense inflammation can also vesiculate, so it can be confusing!
9/
Furthermore, if there’s mucosal involvement, HFMD I think of as causing punctate lesions, not overall sloughing of the membranes (tweet 4). While this isn’t a perfect rule, it can be helpful to differentiate these diseases with similar distributions
pc:oatext.com/coxsackie-A6-i…
Furthermore, if there’s mucosal involvement, HFMD I think of as causing punctate lesions, not overall sloughing of the membranes (tweet 4). While this isn’t a perfect rule, it can be helpful to differentiate these diseases with similar distributions
pc:oatext.com/coxsackie-A6-i…
10/
Let’s summarize:
- EM is usually characterized by papular typical target lesions.
- EM is commonly triggered by infections.
- Treatment focuses on supportive care as well as treating the underlying cause.
Thanks for joining me on this #tweetorial!
Let’s summarize:
- EM is usually characterized by papular typical target lesions.
- EM is commonly triggered by infections.
- Treatment focuses on supportive care as well as treating the underlying cause.
Thanks for joining me on this #tweetorial!