I'm often asked by patients, family members, referring physicians, or clinical trial sponors: "So how do you guys pick which clinical trials to do, anyway?" There are hundreds of trials in hematologic malignancy ongoing... how to choose? Here are some thoughts. Image: @NIH 
We have 30-50 active protocols open in our Adult Leukemia Program @DanaFarber at any given time (albeit not all are open to new accrual), and sponsors approach us about new studies every week, so we have to be selective. Institutionally there are >700 trials, which is amazing./1
The largest group of Leukemia Program studies target #AML – the most common neoplasm in patients referred to us, and where huge needs remain. But there are also trials for ALL, MDS, MPN, CML, aggressive mastocytosis, hairy cell leukemia, even rare BPDCN thanks to @lane_andy /2
(Transplant-specific protocols go through the Transplant Program w/ @DrCCutler; we collaborate closely with them. CLL is a separate program @danafarber; at some institutions, CLL is included in “leukemia” department because of its name, even though it is more akin to lymphoma.)/3
There are 7 clinically oriented faculty in Leukemia program now as well as a number of faculty who see patients & also have labs eg @ColemanLindsley. Naturally we sometimes disagree about which trials seem most promising & which are a good "fit", so we discuss & work that out./4

There are really 4 major considerations in what trials are right for a program to take on, in addition to having a "mix" of early and later-phase trials across disease areas. I think most academic medical centers take these same factors into consideration. /5

First & foremost, does the trial meet a need for our patients? A trial with broad eligibility criteria - a "Statue of Liberty" trial, open to all - that focuses on a common patient population in a space where we don’t already have several open/planned trials: highly attractive./6

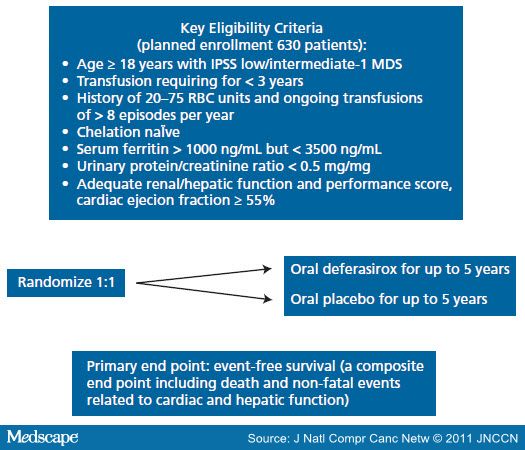
In contrast, a study that has very restrictive entry criteria is a tough "sell". That's why we didn’t participate in TELESTO MDS study, for example, even though question is important. Eligibility criteria (@MedscapeOnc image) were narrow & not all clinicians were in equipoise./7
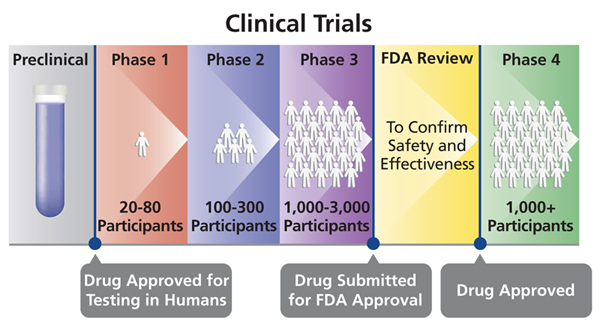
Second: is the study molecule interesting, & potentially safe & effective? This one is *really* hard to judge because every drug has a mechanism that seemed plausible to someone, else they wouldn’t have bothered to write a protocol. (Image:@BostonGlobe @broadinstitute drug hub)/8

That being said, some molecules have a leg up in bioplausibility: they may target common/highly recurrent mutations, have shown a huge effect in pre-clinical models - or maybe there's clinical experience already with similar molecules. Investors watch this too. @adamfeuerstein /9
Third, is the trial design reasonable? "The devil is in the details." Extremely complex trials with multiple randomizations/dose adj are tough. Trials that require many long days for PK/PD assessments may be OK for phase 1s, but there are limits on how many centers can do./10

@VPrasadMDMPH has addressed many trial design issues including various dodgy ways of making results a foregone conclusion. We have an amazing biostastician Donna Neuberg who has deep insight into appropriate trial design & the clinical landscape. People like her are treasures./11
Placebo-controlled monotherapy trials that lack cross-over are tough. (Placebo vs study drug as an add-on to standard therapy is different.) Transfusion-dependent patients often don’t want to go through screening & trek into centers for >24 wks to get a placebo, for example./12

That tension between what is most acceptable to patients and their caregivers and what is most "scientifically rigorous" underscores a lot of debate about human interventional trial design and is too complicated to get into here, but it is important./13
Related to the “reasonable design” is where else the trial is going to be open. We worry about conventional Phase I 3+3 dose escalation trials if the sponsor is planning to open at 14 other sites, because we may never get enough slots for our patients to make it worthwhile./14
Any trial is a *huge* amount of work to open/run. Clinical research & regulatory/contracts teams work really hard, and it isn’t fair to ask them to do hundreds of hours of work for a trial we’re never going to be able to enroll to or is likely to accrue before we get it open./15

Last, does the trial have any “academic value”? A trial that one of our junior faculty members wrote or is playing a key role in, especially an investigator-sponsored study that ties in to her laboratory focus or positions her to get a new grant, is going to get top priority./16
In contrast, a 50+-center industry-sponsored Phase 3 where one group member *might* be 7th or 13th author if we accrue well, would only be a consideration if it was really interesting and well designed and if we also needed such a study to offer to a particular patient cohort./17
In general, the individual sponsor doesn’t matter much for industry trials, with a few exceptions. There are a small no. of companies that have such a terrible reputation, or that we have had problems with before, where we think twice before working with them. This is rare! /18
Most sponsors are highly collaborative. And to be fair, perhaps there are sponsors out there who don't like us for whatever reason and prefer to do a trial at another center. All institutions have strengths & areas of focus; a trial that works in one place may not in another./19
Geography of the sponsor has limited influence. For early stage trials, it can be easier to work with biotechs that are local, but is fine if the sponsor is in the Bay Area or in Sweden or wherever - that's what Zoom and Skype and their ilk are for./20
@theNCI cooperative group trials often ask critical questions, as @DrHBurstein has outlined before. We are big accruers to @ALLIANCE_org & Intergroup studies. But unfortunately many institutions lose money or just break even on these, since NCI trial reimbursement is low./21
So many institutions set limits on how many cooperative group studies they can do, compared to industry-sponsored trials that "pay their own way". I hope this changes in the future. @theNCI is increasingly doing trials in 'community' settings, which is critical for patients./22
At the end of the day we all want trials that are going to work & make things better for patients. (Thread inspired by @rosslevinemd; I'll leave the "how to give a chalk talk", "how to hire people for your lab" etc to him and stick to history or clinical matters like this.😉)/End