1/ #MedTwitter, thanks for joining us last week for our case #tweetorial (bit.ly/38rGrZs)! We have more clinical reasoning practice for you today!
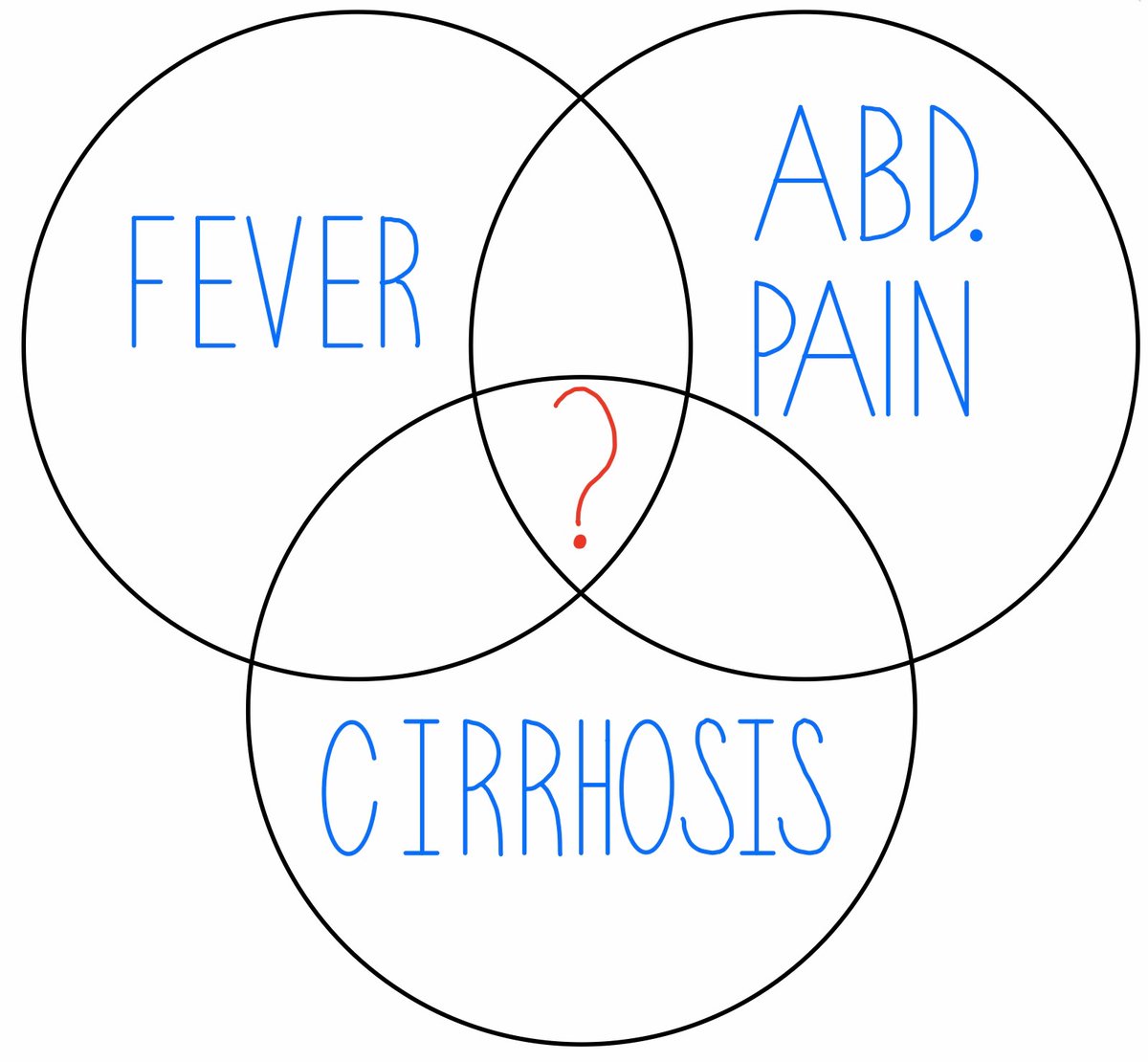
67F w/ HTN, HFpEF & RA (on chronic prednisone & PCP PPx) p/w 3 days of progressive dyspnea, malaise & productive cough.
67F w/ HTN, HFpEF & RA (on chronic prednisone & PCP PPx) p/w 3 days of progressive dyspnea, malaise & productive cough.
2/ As you get more information, what clinical reasoning tool can you use to determine how the data you gather increases or decreases the probability of the diseases you’re considering?
3/ ANS: Likelihood ratio. LRs help us decide how much each test result increases or decreases the probability of a specific disease.
For example, her history of HF has an LR of ~5 for HF as the cause of her dyspnea, increasing the probability of a HF exacerbation by ~30%.
For example, her history of HF has an LR of ~5 for HF as the cause of her dyspnea, increasing the probability of a HF exacerbation by ~30%.

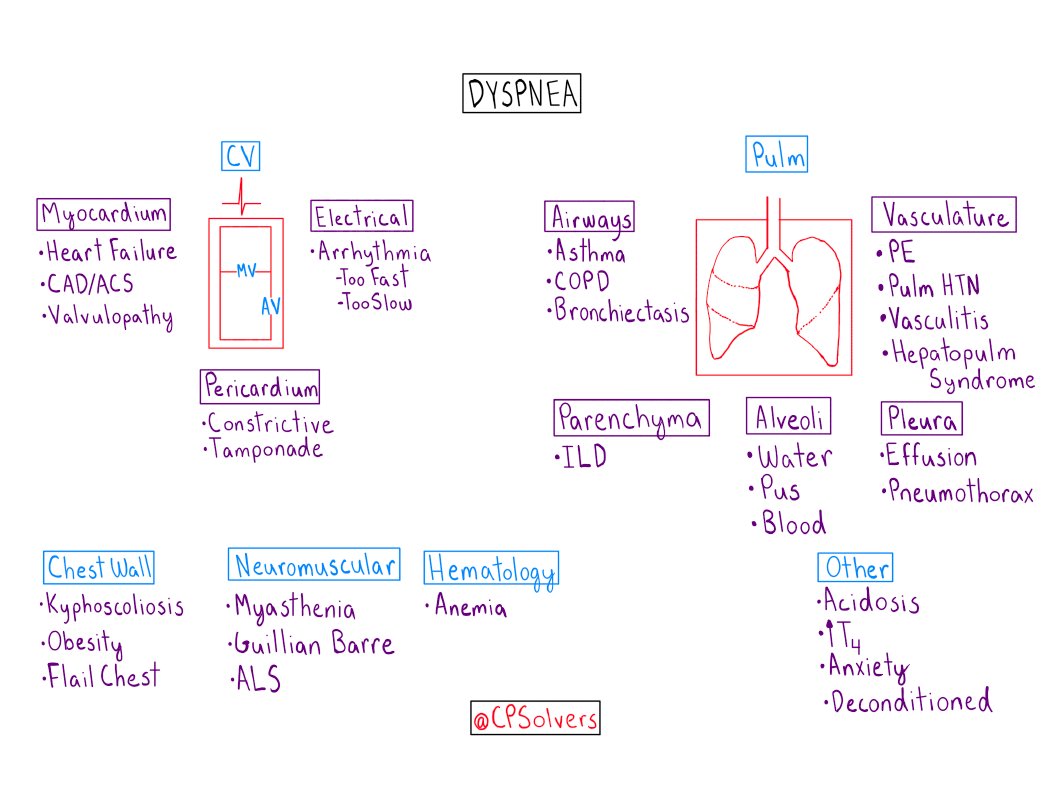
4/ Given her medical history and symptoms, which diagnosis are you most suspicious of as the cause of her current illness?
5/ At this point, all of these are worth considering, along with many others.
Epidemiology (e.g. the base rate of PNA), background info (e.g. HFpEF & ongoing immunosuppression), and lack of obvious risk factors for DVT/PE may also shift HF and PNA higher in your mind.
Epidemiology (e.g. the base rate of PNA), background info (e.g. HFpEF & ongoing immunosuppression), and lack of obvious risk factors for DVT/PE may also shift HF and PNA higher in your mind.
6/ On exam, her temperature is 99.2F, HR is 112, BP 137/62, and SaO2 86% on room air.
She has⬆️work of breathing. JVP is not visible while sitting up at 45 deg. No S3 or S4. Coarse crackles are present in the bilateral, middle lung fields. She has no lower extremity edema.
She has⬆️work of breathing. JVP is not visible while sitting up at 45 deg. No S3 or S4. Coarse crackles are present in the bilateral, middle lung fields. She has no lower extremity edema.
7/ Her labs show a WBC of 10.7 with neutrophil predominance. Na of 136, BUN of 22, Cr 1.03 (baseline). BNP is 52.
CXR is shown below (Image courtesy of Dr Roberto Schubert, Radiopaedia.org, rID: 17327)
CXR is shown below (Image courtesy of Dr Roberto Schubert, Radiopaedia.org, rID: 17327)

8/ How have the physical exam and labs influenced the probability of different diseases?
Please share your reasoning with us by replying to this tweet in addition to answering below!
Please share your reasoning with us by replying to this tweet in addition to answering below!
9/ ANS: HF down, PNA up.
It can be extremely difficult to tease out PNA from HF. Often, the exam, CXR, and BNP help make the dx.
She has many findings that point against HF as the cause of her dyspnea.
Which one(s) made the biggest difference for you?
It can be extremely difficult to tease out PNA from HF. Often, the exam, CXR, and BNP help make the dx.
She has many findings that point against HF as the cause of her dyspnea.
Which one(s) made the biggest difference for you?
10/ ANS: B&C. The absence of cardiomegaly and the BNP < 100 most strongly suggest against a HF exacerbation as the cause of dyspnea with LRs of ~0.3 & ~0.1 respectively.
An LR of 0.3 decreases the pretest probability by ~25%, and an LR of 0.1 by ~45%. (Image: Dr. Steven McGee)
An LR of 0.3 decreases the pretest probability by ~25%, and an LR of 0.1 by ~45%. (Image: Dr. Steven McGee)

11/ Her neutrophil-predominant leukocytosis and multi-focal consolidations support the diagnosis of an acute, inflammatory pulmonary syndrome.
An acute pulmonary infection (e.g. community acquired pneumonia) is a very common cause of that clinical syndrome.
An acute pulmonary infection (e.g. community acquired pneumonia) is a very common cause of that clinical syndrome.
12/ While she is afebrile, the lack of fevers, especially in the setting immunosuppression via prednisone, does not meaningfully decrease the probability of an infectious process.
13/ Finally, remember the power of your own clinical judgment.
There are many unquantifiable factors in this case (e.g., the appearance of the consolidations on CXR, the fact that she is on chronic prednisone) that change the way we weigh diagnostic probabilities.
There are many unquantifiable factors in this case (e.g., the appearance of the consolidations on CXR, the fact that she is on chronic prednisone) that change the way we weigh diagnostic probabilities.
14/ LRs, while helpful, are just one tool you can use to SUPPORT your clinical judgment, not REPLACE it.
15/ She is given a working diagnosis of PNA and started on a 5 day course of antibiotics. Her hypoxia, cough, and malaise all resolve and she is discharged home.
16/ That covers it, Clinical Problem Solvers!
Thank you for reasoning with us, and be sure to check out @jackpenner’s article to review and reinforce these concepts! bit.ly/2Stzh1e
Thank you for reasoning with us, and be sure to check out @jackpenner’s article to review and reinforce these concepts! bit.ly/2Stzh1e