,
55 tweets,
23 min read
Read on Twitter
#MedTwitter has been discussing “Take Two Aspirin + Call Me By My Pronouns,” an op-ed claiming social justice is taking time from sci ed + decreasing the quality of #MedEd.
So here’s my take:
“Take Two Aspirin + Read a Curriculum”
THREAD.
#MedTwitter #SoMeDocs #DoubleDocs
So here’s my take:
“Take Two Aspirin + Read a Curriculum”
THREAD.
#MedTwitter #SoMeDocs #DoubleDocs
As always, I start threads with my POV: #LatinasInMedicine #DoubleDocs student in year 2 of #medschool. I have interests in both #MedEd + #HealthJustice. I am about to finish my term as diversity rep on our med student govt. I care a lot about advocacy.
Let’s take a moment to learn about the author: Stanley Goldfarb is a nephrologist, *former* assoc dean of curriculum at UPenn Med. He graduated from med school in 1969. Ffolks who studied at UPenn have brought up negative experiences with Dr. Goldfarb.
Alright, let’s go point by point and examine Dr. Goldfarb’s argument.
Starting w title, we can see that Dr. Goldfarb has an issue w pronoun conversations. Using proper pronouns when referring to someone is a sign of respect, which we should be showing to all of our patients...
Starting w title, we can see that Dr. Goldfarb has an issue w pronoun conversations. Using proper pronouns when referring to someone is a sign of respect, which we should be showing to all of our patients...
... It also creates space for the patient to share information about their gender identity if they would like. This could be information that may be relevant to their care. Or it might inform who you refer them to. But most of all it shows patients they can trust you.
The subtitle to the piece reads “At ‘woke’ medical schools, curricula are increasingly focused on social justice rather than treating illness.” The fact that woke is in quotations tells you a lot already.
By using “rather than” there is an implication that it is somehow impossible to have a curriculum that introduces topics around social justice + advocacy without it being detrimental to caring for disease.
This is a false dichotomy (as many on #MedTwitter have pointed out). If anything we learn way more basic science (quantity + range of material) in #medschool now than they did in 1960s based on the amount that has been learned in basic sci + clinical care in the past fifty years.
Dr. Goldfarb starts off the piece with claiming that it was inappropriate for the American College of Physicians to make a statement about gun control which is “out of its lane.”
#ThisIsOurLane #GunReformNow #PutKids1st
#ThisIsOurLane #GunReformNow #PutKids1st
Turns out ACP was joined by other organizations (AMA, AAFP, ACS, AAP, APA, APHA) in pointing out numerous ways in which gun safety IS a healthcare issue: doi.org/10.7326/M19-24…
Also notable is that Dr. Goldfarb is past president of the Philadelphia College of Physicians which is the Philadelphia chapter of the ACP.
Seems out of place considering the piece is about medical education. But then you see that he uses it as a way to hook the general audience reader into caring about #MedEd. He is trying to incite outrage.
He then pivots to an anecdote about how a faculty member “chastised” him for not including mention of climate change being related to health in the UPenn Med curriculum. (Seems like there is a lot of personal resentment in these chosen examples...🤷🏽♀️).
There is plenty of research out there about this, but I’ll point to this NIH fact sheet about climate change and health (past, present + future) as a brief summary: report.nih.gov/nihfactsheets/…
#ClimateStrike
#ClimateStrike
Then comes the main question of the piece...Since when is the only purpose of medicine to cure patients? Should medical school not be preparing us to prevent disease? Or to help patients manage their experience of illness? 🤔

Then he comes after the real culprit: “a new wave of education specialists.” Yes, as we learn more about medicine and how we can better support our patients, new topics come up to teach the next generation—topics like social justice!
Dr. Goldfarb seems annoyed with the desire to make medicine less elitist...But is it not a good thing to have providers who do not feel superior to their patients? Perhaps this would help with things like bias and mistrust in the medical system/care....

Next is the claim that teaching medical students about health disparities + diversity are “worthwhile goals” but take away from learning sci. Not sure where the evidence for this is bc we are learning plenty of science (again > students in the 1960s) and it is def rigorous. #SDOH
The next line is especially interesting bc it reads as a sort of ‘call to action’ to general public that they should be concerned that med students are learning to see patients as full ppl + communities as interconnected parts of health. Interesting that this is = “politicized”
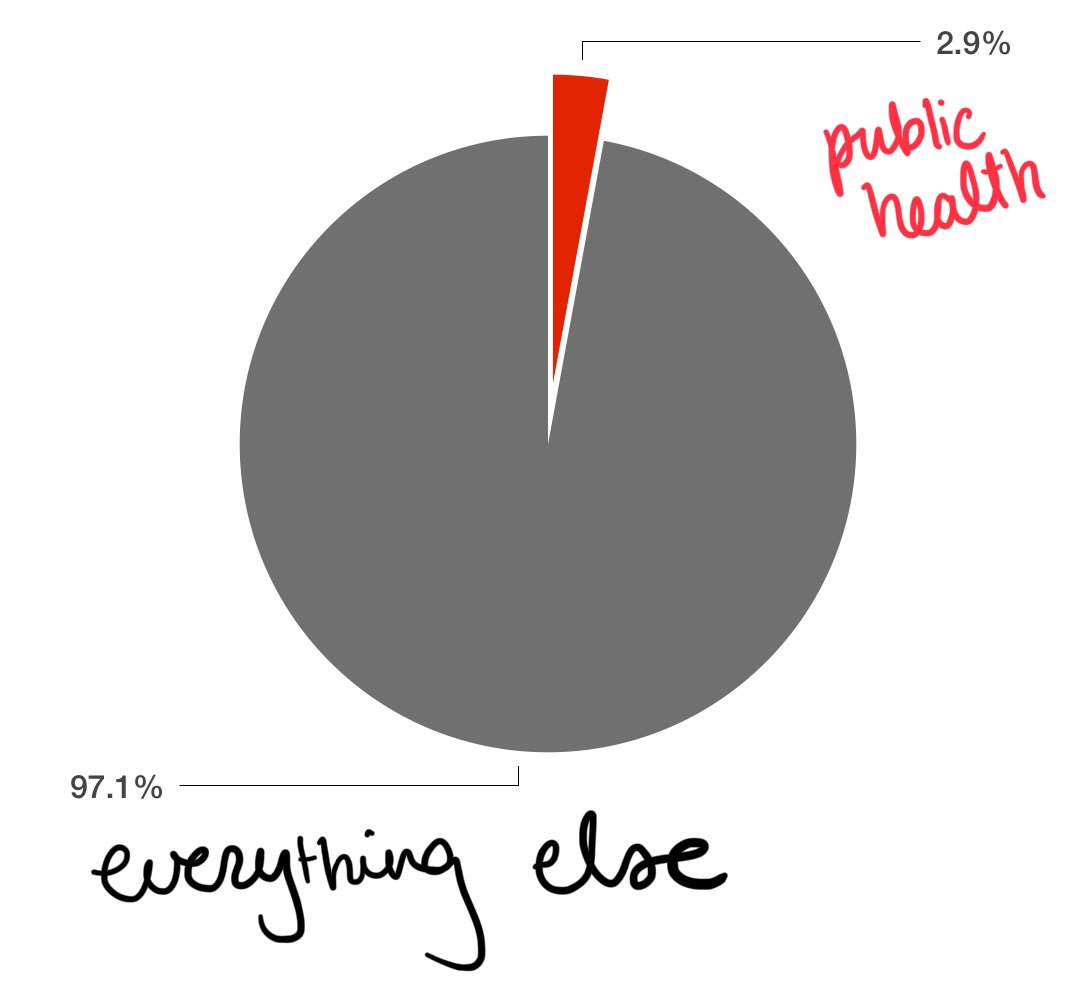
To give an example from my personal experience, last semester (Jan-June 2019) our class had
🔹22 weeks of class
🔹~445 total classes (lectures + small group)
🔹13 were related to public health, maybe even social justice.
That’s 0.029% of our content last semester.
🔹22 weeks of class
🔹~445 total classes (lectures + small group)
🔹13 were related to public health, maybe even social justice.
That’s 0.029% of our content last semester.

If all of last semester = 1 hour of instruction, we would have received 1.75 min on public health, #SDOH, advocacy, bias, healthcare disparities... I received more ed time on surg options for urogenital problems than on navigating religious difference in the exam room for e.g.
Not to say that I don’t think surgical interventions in urogenital conditions is not important (it is), but I am very unlikely to need a lot of those details in my future career 🤷🏽♀️
Maybe there are schools who are spending even more time than us (if so, would really like to know what your curriculum looks like!) but I doubt even for those you could make the claim that “social justice is taking over” to the detriment of science.
I would also like to add that this assumes that public health, epidemiology, policy, and other kinds of research are any less “scientific” or unimportant to the practice of medicine. Flat out wrong. Thanks, @traependergrast!
Next is a paragraph that sounds like longing for the good old days of #MedEd.
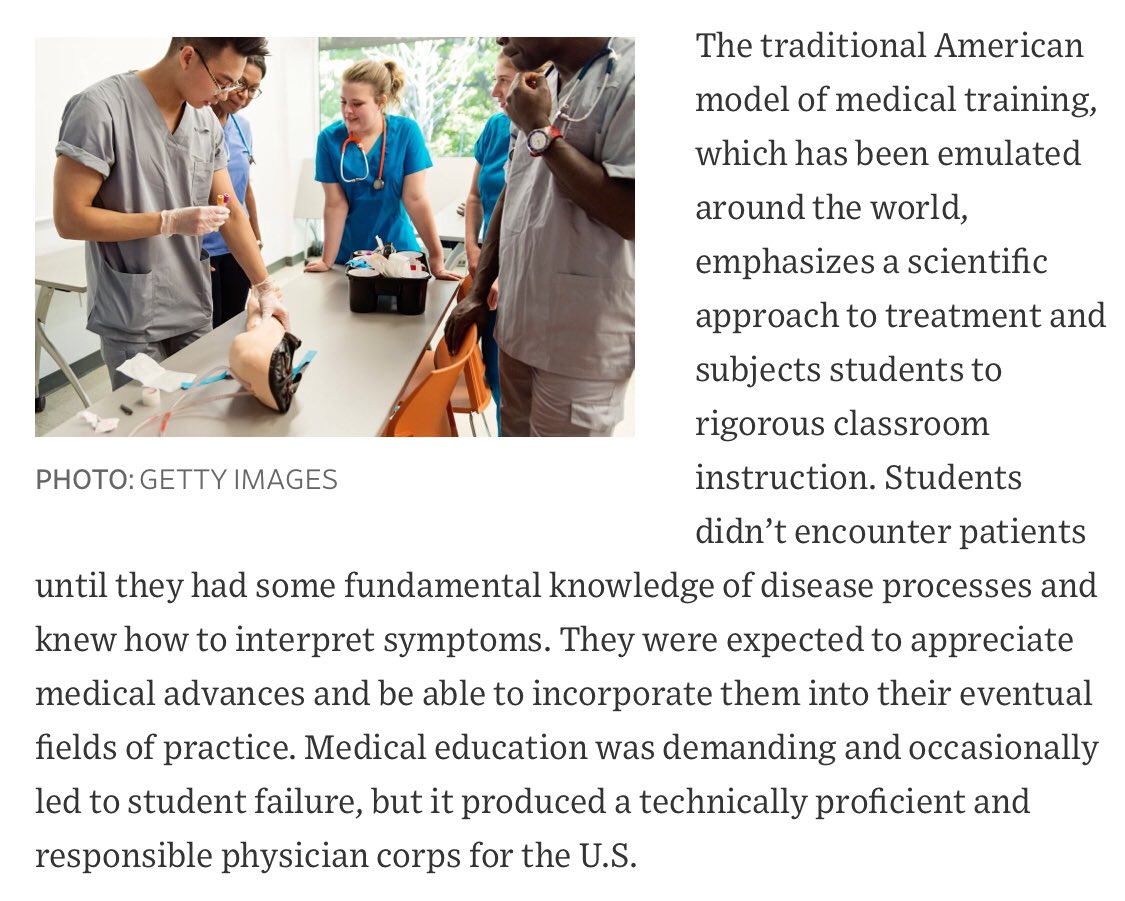
However, where is the evidence that today’s doctors are less proficient and responsible? Has he seen the rise of USMLE Step 1 scores? (Sorry @jbcarmody i know this is an imperfect metric) Are recently graduated doctors really “worse” than before?
As for not interacting with patients until we had all the facts down, this goes against so much evidence in pedagogy + #MedEd teaching. Also depends on what your goals are: should medical students be receiving only training in regurgitating science facts?
For me it has been crucial to incorporate the patient experience into learning about diseases and conditions. It makes me care more about side effects or difficulties and want to know these things in order to better help the patient.
Am I reading this paragraph incorrectly or does he think the purpose of medicine is not to provide equal opportunity to being + staying healthy in society?

The following paragraph is a rant about how #MedEd is emphasizing sociology/social work issues (Remember, we are a team in healthcare). Apparently the goal is to turn us into primary care physicians, but the tone makes it sound like that is a bad thing + to be frowned upon...
As physicians at the bare minimum we should be equipped to be able to recognize sociology/social work in action so that we can CALL A SOCIAL WORKER. Or alter our practice of medicine to fit that patient’s needs.
Also ping to @ml_barnett’s point:
Also ping to @ml_barnett’s point:
Apparently Dr. Goldfarb is not aware of the #MedEd literature in the past few decades bc curricula are using “Theories of learning w virtually no experimental basis.” Med students are not individually mastering material according to him + there is too much teamwork 🤷🏽♀️
Dr. Goldfarb starts to wrap up with concern about all of this going too far. The inclusion of ‘tangential’ + “progressive causes” will be downfall of medicine. Pretty doom + gloom considering our generation just wants folks to get = access to care + not die from gun injuries...

The last paragraph provides an unsatisfying conclusion. Specialists spend countless years training after medical school focused exactly on the topic that they are *specializing* in. Medical school provides a generalized framework of knowledge for future physicians.

Could we probably use a few more specialists? Of course. Should even specialists care about advocacy, social justice, public health, etc. YES.
Some of us might even go on + specialize in social justice Some folks get an MD + then go focus on business or healthcare consulting or policy or education. Yet I doubt learning about cytochrome P450s + hormonal pathways hinders them from picking up new skills moving forward.
Social justice + advocacy is part of med whether folks would like it to be or not. And we should be making sure that students receive adequate training to engage further w topics they may encounter in their future careers.
If anything we should want physicians who are well-informed even if it is not their area of ultimate expertise.
Why? Because
Spending hrs getting insurance to approve treatment for a patient is advocacy.
Talking to patients about gun safety is advocacy.
Using an interpreter to make sure an encounter is clear is advocacy.
Spending hrs getting insurance to approve treatment for a patient is advocacy.
Talking to patients about gun safety is advocacy.
Using an interpreter to make sure an encounter is clear is advocacy.
Knowing where your patient lives + what environmental exposures may be affecting them is advocacy.
Connecting a patient to victim services is advocacy.
Ensuring that your exam rooms have tables that are accessible to those in wheelchairs or w movement restrictions is advocacy.
Connecting a patient to victim services is advocacy.
Ensuring that your exam rooms have tables that are accessible to those in wheelchairs or w movement restrictions is advocacy.
Sharing your expertise on issues relating to health with policymakers is advocacy.
Recognizing med + social risk factors for future disease + having a convo about prevention is advocacy.
Respecting a patient’s belief structures + inviting a chaplain into convo is advocacy.
Recognizing med + social risk factors for future disease + having a convo about prevention is advocacy.
Respecting a patient’s belief structures + inviting a chaplain into convo is advocacy.
And as a future physician I would like to be aware and prepared to handle anything that might come up in my patients’ lives. Be it medical, social, or whatever.
That’s all I have got for now, folks!
Please share your comments and let me know where you agree/disagree/want to add nuance.
You can access this thread (and my other threads) in document form at tiny.cc/ThreadsByBri
Please share your comments and let me know where you agree/disagree/want to add nuance.
You can access this thread (and my other threads) in document form at tiny.cc/ThreadsByBri
Following tweets will link to other responses about Dr. Goldfarb’s piece.
WSJ Editorial Board: Corrupting Medical Education
wsj.com/articles/corru…
*sigh*
WSJ Editorial Board: Corrupting Medical Education
wsj.com/articles/corru…
*sigh*
First tweet I saw about the piece, from @EricTopol:
Thoughtful reflections by @RoxanaDaneshjou:
Response by UPenn faculty members:
inquirer.com/health/social-…
inquirer.com/health/social-…
@londyloo started a thread of advocates in medicine/healthcare to follow:
Some humor by @rozehnalmd:
Errata: Thanks to @DrGaellon for pointing out my % was wrong 🤦🏽♀️
I’m human + apparently know way more about SNARE proteins + reflex arcs atm (neurobio, told you we learn basic sci) than arithmetic
Correct: 2.5%, which is STILL 1.74 min in following tweet.
I’m human + apparently know way more about SNARE proteins + reflex arcs atm (neurobio, told you we learn basic sci) than arithmetic
Correct: 2.5%, which is STILL 1.74 min in following tweet.
Errata: CPP =/= Philadelphia chapter of ACP. So many acronyms and I managed to jumble them all up! Thanks for fact-checking that one, @BobDohertyACP, Senior VP over at ACP.
Dr. Goldfarb’s daughter offered this insight:
Clearly something led the editors to think that this title/subtitle would
A) match the body of the article
B) catch folk’s attn
so I’m pretty sure what I point out still stand even if he didn’t write them
Clearly something led the editors to think that this title/subtitle would
A) match the body of the article
B) catch folk’s attn
so I’m pretty sure what I point out still stand even if he didn’t write them