𝗖𝗼𝘃𝗶𝗱-𝟭𝟵: 𝗻𝗼𝘁𝗲𝘀 𝗼𝗻 𝗮 𝗽𝗮𝗻𝗱𝗲𝗺𝗶𝗰
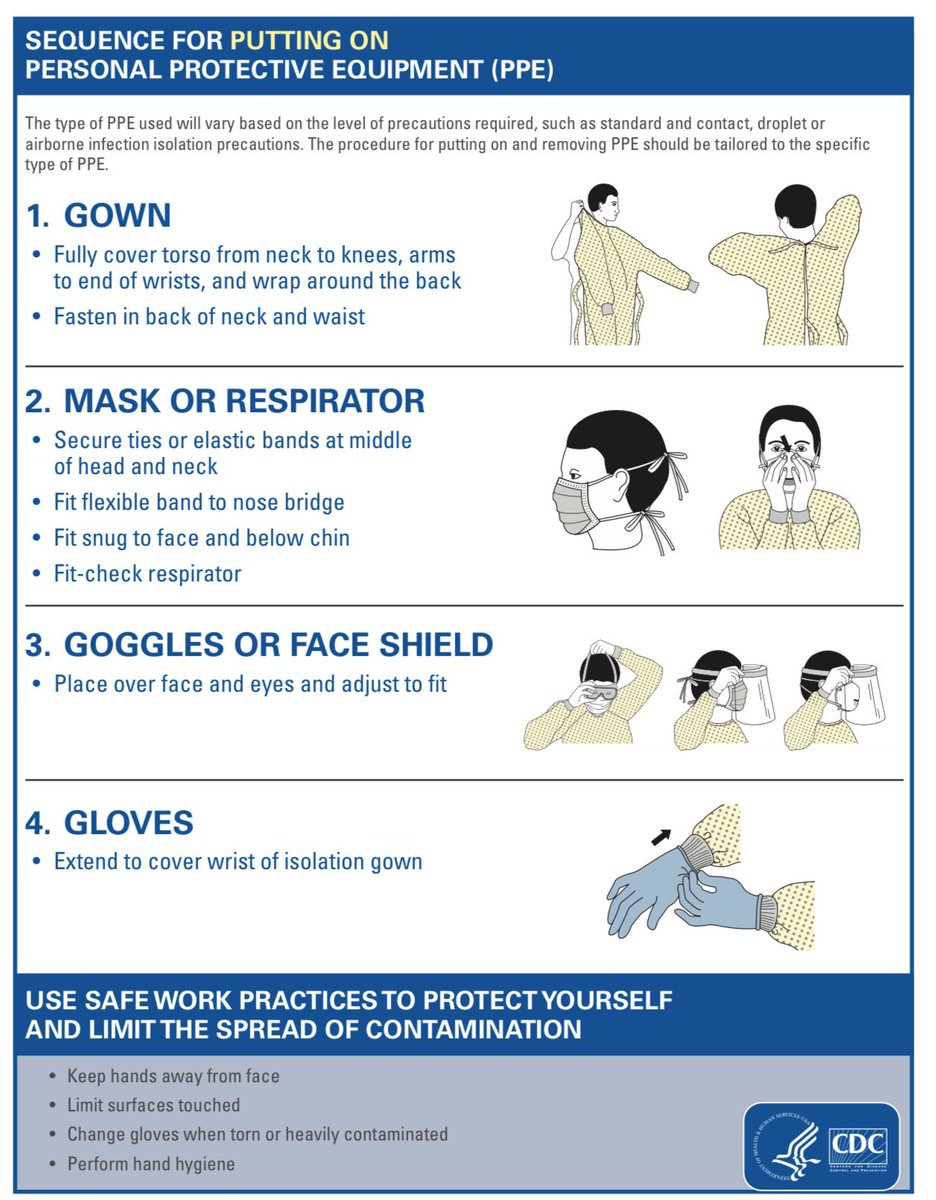
1/17 1️⃣ Prevention: healthcare
Standard, contact, droplet, eye protection, airborne (N95) in aerosol-generating procedures, until Sx resolve & 2 (-) swabs 24H apart
CDC: bit.ly/2Wb0VCy
WHO: bit.ly/2UcMwTA
1/17 1️⃣ Prevention: healthcare
Standard, contact, droplet, eye protection, airborne (N95) in aerosol-generating procedures, until Sx resolve & 2 (-) swabs 24H apart
CDC: bit.ly/2Wb0VCy
WHO: bit.ly/2UcMwTA
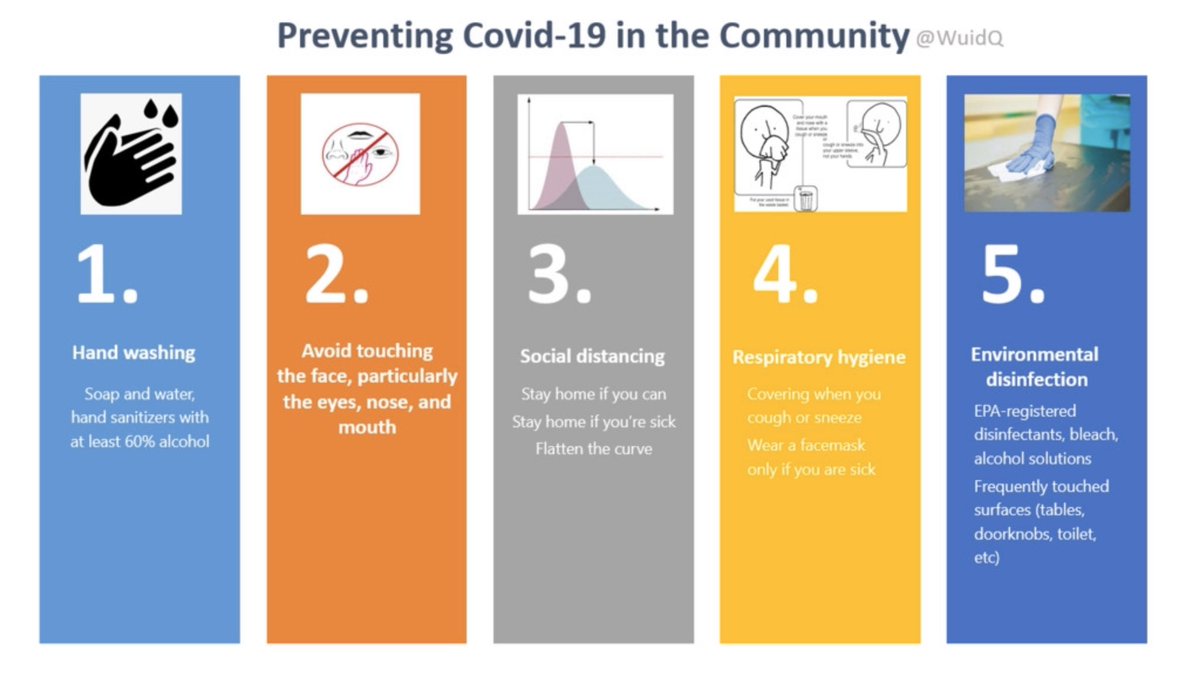
2/17 1️⃣ Prevention: community
Vaccine development ongoing
5 things you can do to protect yourself 👇 [Fig 1]
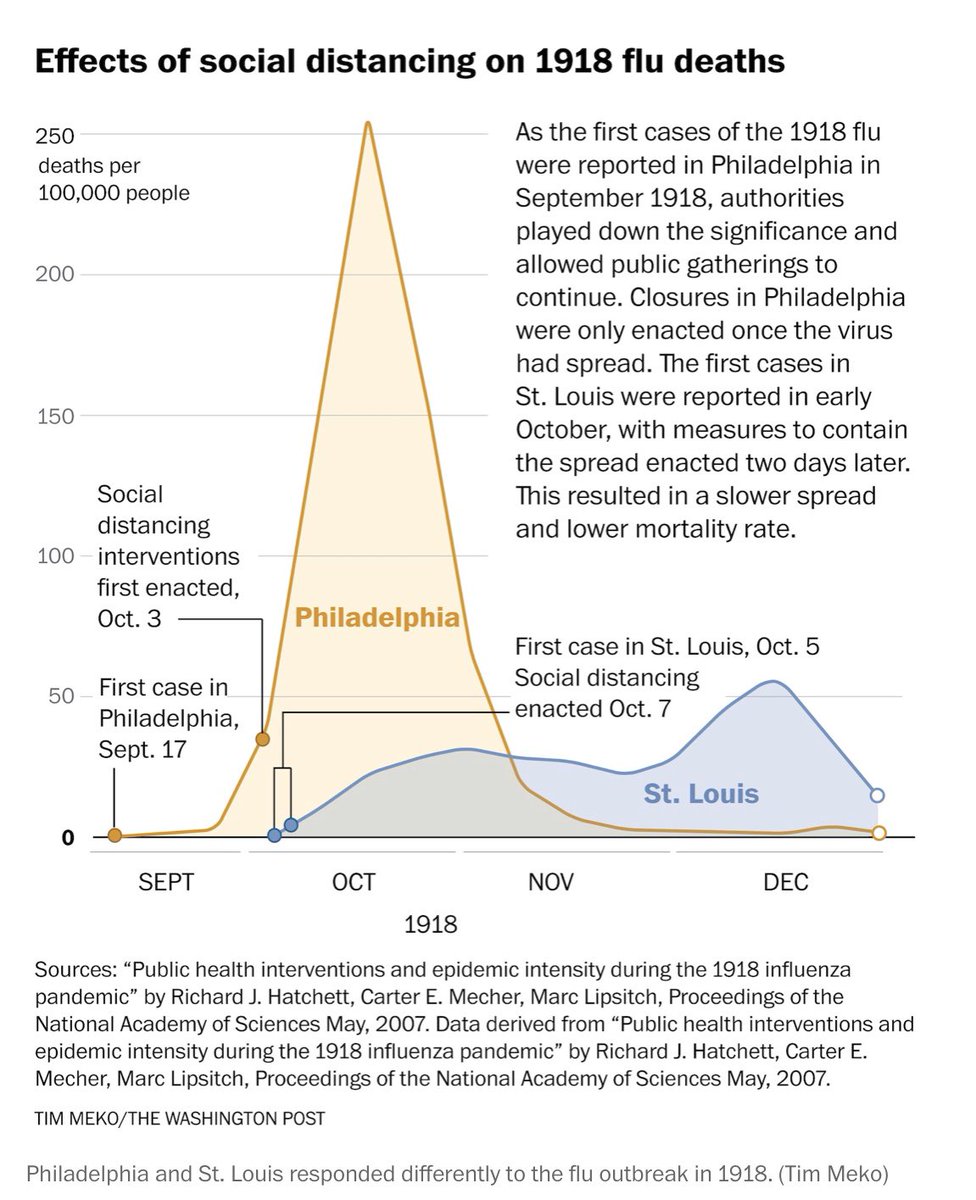
Flattening the curve is not just a mathematical modeling; history has shown its importance 👇[Fig 2] wapo.st/2WeypQp
CDC: bit.ly/2QiCTSj
Vaccine development ongoing
5 things you can do to protect yourself 👇 [Fig 1]
Flattening the curve is not just a mathematical modeling; history has shown its importance 👇[Fig 2] wapo.st/2WeypQp
CDC: bit.ly/2QiCTSj
3/17 2️⃣ Clinical features
Incubation: median 4 days (2-7 days ); up to 14 days
98% develop Sx within 12 days bit.ly/2w3dzJi
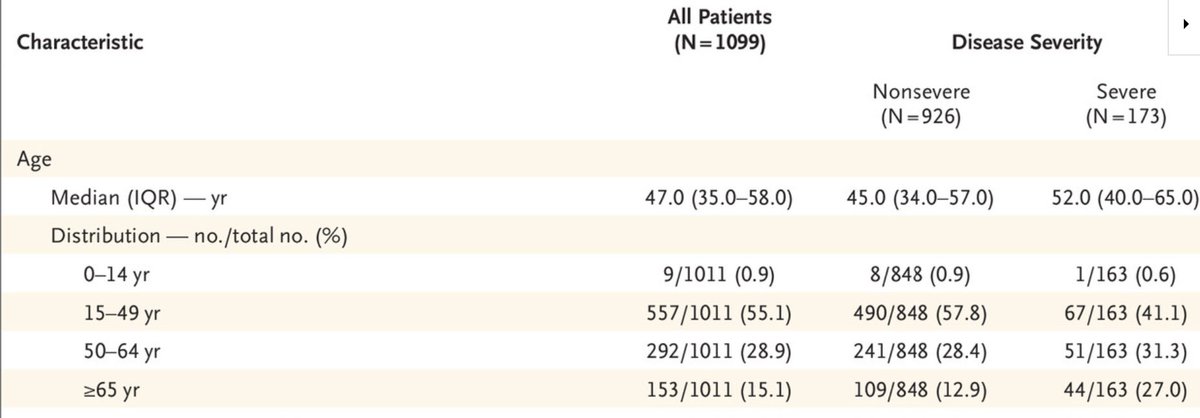
Everyone, regardless of age, is SUSCEPTIBLE and can be a vector of infection👇 >50% of cases are in people <50 yrs. bit.ly/38UbRY2
Incubation: median 4 days (2-7 days ); up to 14 days
98% develop Sx within 12 days bit.ly/2w3dzJi
Everyone, regardless of age, is SUSCEPTIBLE and can be a vector of infection👇 >50% of cases are in people <50 yrs. bit.ly/38UbRY2
4/17 2️⃣ Clinical features
▪️Fever, almost universal Sx bit.ly/38UbRY2
⚡️Can be + in only 50% of pts at presentation
▪️Cough, 2nd most common (dry; only 1/3 +sputum)
▪️More gradual onset than influenza; can develop pneumonia
after the 1st week
▪️Fever, almost universal Sx bit.ly/38UbRY2
⚡️Can be + in only 50% of pts at presentation
▪️Cough, 2nd most common (dry; only 1/3 +sputum)
▪️More gradual onset than influenza; can develop pneumonia
after the 1st week
5/17 2️⃣ Clinical features
Note that nasal congestion is uncommon (5%).
Diarrhea (4%), sore throat (14%), HA (14%) can be present
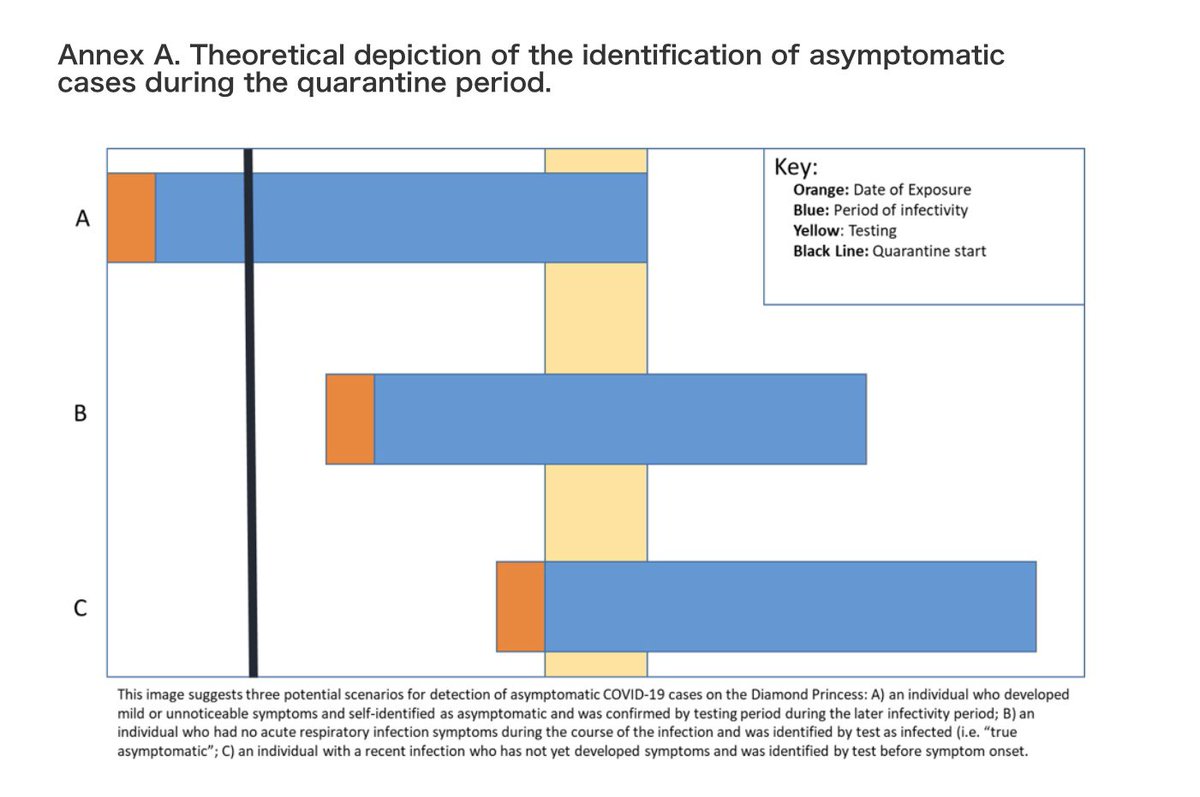
Asymptomatic infection, unknown👇More data needed.
✔️ Diamond Princess cases: 51% were asymptomatic
[Figure: bit.ly/2TWl1Pt]
Note that nasal congestion is uncommon (5%).
Diarrhea (4%), sore throat (14%), HA (14%) can be present
Asymptomatic infection, unknown👇More data needed.
✔️ Diamond Princess cases: 51% were asymptomatic
[Figure: bit.ly/2TWl1Pt]
6/17 2️⃣ Clinical features
▪️ Nonspecific lab findings
▪️ Lymphopenia, most common finding (63%)
▪️ Can have high WBC or low WBC
▪️ Procalcitonin normal at presentation (70%)
▪️ Nonspecific lab findings
▪️ Lymphopenia, most common finding (63%)
▪️ Can have high WBC or low WBC
▪️ Procalcitonin normal at presentation (70%)
7/17 2️⃣ Clinical features
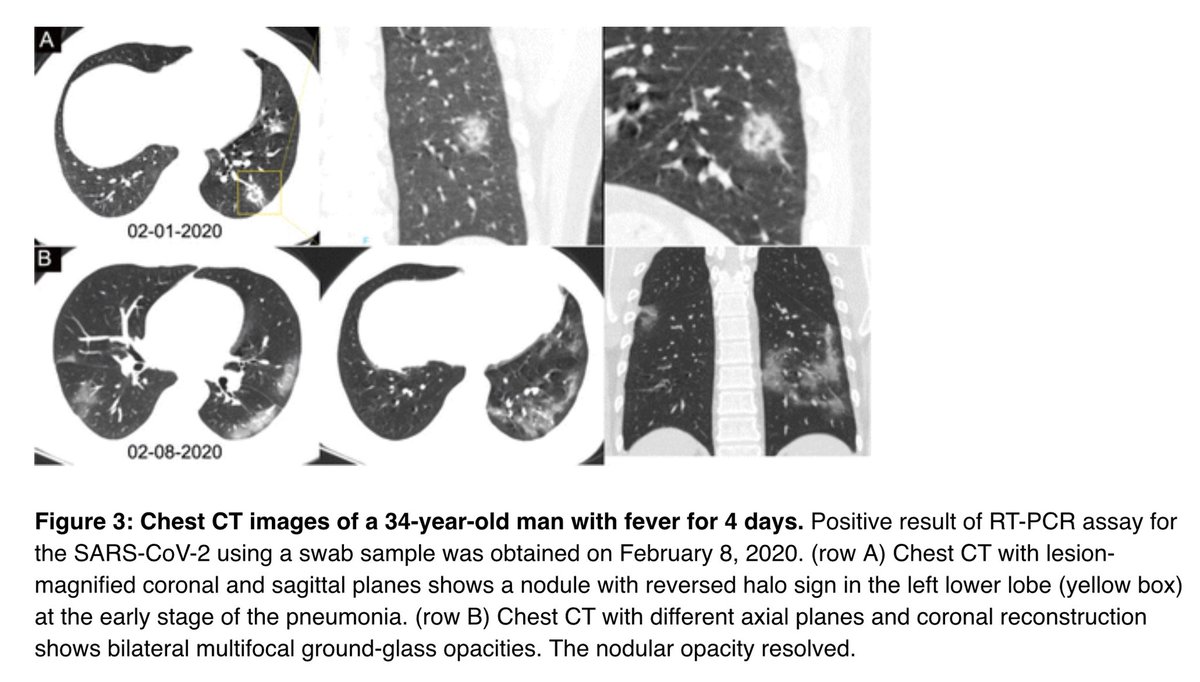
Imaging findings, also nonspecific
✔️Ground glass opacities usually b/l, peripheral,
lower lobe
✔️Less common: pleural effusion, air bronchogram,
lymphadenopathy
✔️Reverse halo sign in 11% 👇bit.ly/2vwya8w
Imaging findings, also nonspecific
✔️Ground glass opacities usually b/l, peripheral,
lower lobe
✔️Less common: pleural effusion, air bronchogram,
lymphadenopathy
✔️Reverse halo sign in 11% 👇bit.ly/2vwya8w
8/17 2️⃣ Clinical features
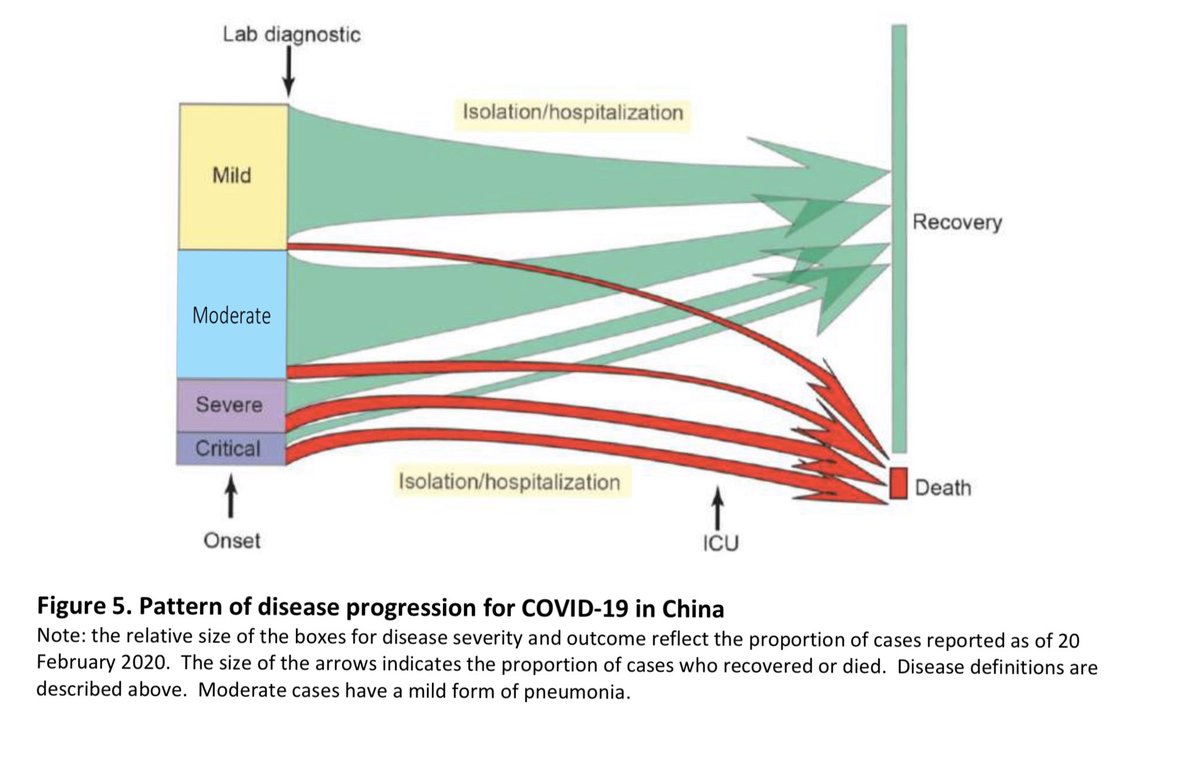
Spectrum 👇 [Fig: bit.ly/2TVLfBy]
✔️ 80% mild/no PNA
✔️ 14% severe (RR >30, hypoxia)
✔️ 5% critical (resp failure, shock)
Spectrum 👇 [Fig: bit.ly/2TVLfBy]
✔️ 80% mild/no PNA
✔️ 14% severe (RR >30, hypoxia)
✔️ 5% critical (resp failure, shock)
9/17 2️⃣ Clinical features
Among 138 hospitalized pts: bit.ly/2U9rchS
✔️ 26% required ICU
✔️ 16% developed ARDS
✔️ 12% required mechanical ventilation
✔️ 3% (n = 4) required ECMO
Among 138 hospitalized pts: bit.ly/2U9rchS
✔️ 26% required ICU
✔️ 16% developed ARDS
✔️ 12% required mechanical ventilation
✔️ 3% (n = 4) required ECMO
10/17 2️⃣ Clinical features
Recovery 2 wks, 3-6 wks in critically ill
Mortality 2.3% but higher in certain groups:
✔️ 15% >80 yrs, 8% 70-79% yrs, 50% critical illness
✔️ CVD > DM, HTN, chronic resp dx, cancer
bit.ly/2TUz47T, bit.ly/2TVLfBy
Recovery 2 wks, 3-6 wks in critically ill
Mortality 2.3% but higher in certain groups:
✔️ 15% >80 yrs, 8% 70-79% yrs, 50% critical illness
✔️ CVD > DM, HTN, chronic resp dx, cancer
bit.ly/2TUz47T, bit.ly/2TVLfBy
11/17 3️⃣ Transmission
Need more studies. Via droplets (6 ft). Stable in aerosols/fomites; may play a role in transmission. bit.ly/3di1DnI
⚡️Aerosol (3h), copper (4h), cardboard (24h)
⚡️Plastic/steel (2-3 days)
Asymptomatic transmission ? bit.ly/2WyebS3
Need more studies. Via droplets (6 ft). Stable in aerosols/fomites; may play a role in transmission. bit.ly/3di1DnI
⚡️Aerosol (3h), copper (4h), cardboard (24h)
⚡️Plastic/steel (2-3 days)
Asymptomatic transmission ? bit.ly/2WyebS3
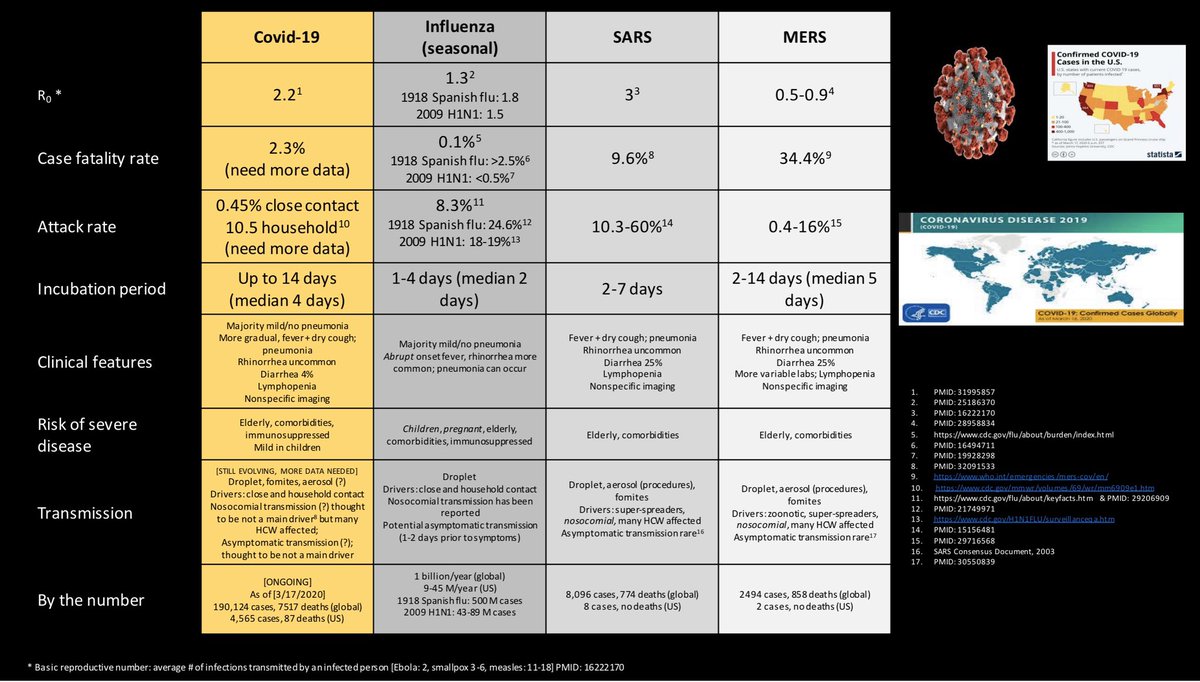
12/17 4️⃣ Comparisons w/ flu, SARS, MERS
Data presented👇based on lit review. Need more data for COVID.
⚡️Covid shares features of flu & SARS/MERS
⚡️Covid spreads like flu (exc asymptomatic tx?) but w/ higher
mortality
⚡️ Covid (?superspread bit.ly/3di1DnI)
Data presented👇based on lit review. Need more data for COVID.
⚡️Covid shares features of flu & SARS/MERS
⚡️Covid spreads like flu (exc asymptomatic tx?) but w/ higher
mortality
⚡️ Covid (?superspread bit.ly/3di1DnI)
13/17 5️⃣ Testing
Fever and/or cough/dyspnea w/ epi link prior 14 d:
✔️ close contact (6 ft; no PPE)
✔️ residence/travel high risk areas
Also can be considered in severe lower resp illness w/o alternative dx, even in the absence of epi link
Fever and/or cough/dyspnea w/ epi link prior 14 d:
✔️ close contact (6 ft; no PPE)
✔️ residence/travel high risk areas
Also can be considered in severe lower resp illness w/o alternative dx, even in the absence of epi link
14/17 5️⃣ Testing
CDC recommends prioritizing (limited testing resources):
✔️ hospitalized pts
✔️ high risk pts (immunosuppressed, >65 y, comorb)
✔️ high risk exposure (travel, being a HCW)
Need to do infection control measures when COVID supsected
bit.ly/3b724iu
CDC recommends prioritizing (limited testing resources):
✔️ hospitalized pts
✔️ high risk pts (immunosuppressed, >65 y, comorb)
✔️ high risk exposure (travel, being a HCW)
Need to do infection control measures when COVID supsected
bit.ly/3b724iu
15/17 6️⃣ Treatment
Triage (home vs hospital)
Largely supportive care
Investigational drugs (RCTs ongoing):
⚡️ Remdesivir
⚡️ Chloroquine, hydroxychloroquine
⚡️ Ritonavir/lopinavir
⚡️ Tocilizumab (IL-6 inhibitor)
Triage (home vs hospital)
Largely supportive care
Investigational drugs (RCTs ongoing):
⚡️ Remdesivir
⚡️ Chloroquine, hydroxychloroquine
⚡️ Ritonavir/lopinavir
⚡️ Tocilizumab (IL-6 inhibitor)
16/17 7️⃣ Virology
A betacoronavirus, same genus as SARS & MERS
❗️SARS-CoV-2: name of virus
‼️ COVID-19: name of disease
Enters via ACE-2 in lungs, GI, kidneys
⚡️No current evidence to show harmful effect of ACEI or ARB
on COVID-19 bit.ly/3b5EUcC
A betacoronavirus, same genus as SARS & MERS
❗️SARS-CoV-2: name of virus
‼️ COVID-19: name of disease
Enters via ACE-2 in lungs, GI, kidneys
⚡️No current evidence to show harmful effect of ACEI or ARB
on COVID-19 bit.ly/3b5EUcC
17/17 8️⃣ Epidemiology
Rapidly changing. Lots of hot spots to date. Here are my favorite sites to get uptodate info on epi:
Hopkins: bit.ly/2UeMI4R
WHO: bit.ly/38ScSQg
Live: bit.ly/3a2aLL1
Rapidly changing. Lots of hot spots to date. Here are my favorite sites to get uptodate info on epi:
Hopkins: bit.ly/2UeMI4R
WHO: bit.ly/38ScSQg
Live: bit.ly/3a2aLL1
17/N
In the spirit of volunteerism, our students at @WUSTLmed have come up with very useful literature review of #COVID19. Will share this with you as it comes in realtime.
@CGhaznavi @JenniferSpicer4 @BradCutrellMD @TxID_Edu
In the spirit of volunteerism, our students at @WUSTLmed have come up with very useful literature review of #COVID19. Will share this with you as it comes in realtime.
@CGhaznavi @JenniferSpicer4 @BradCutrellMD @TxID_Edu
17/N
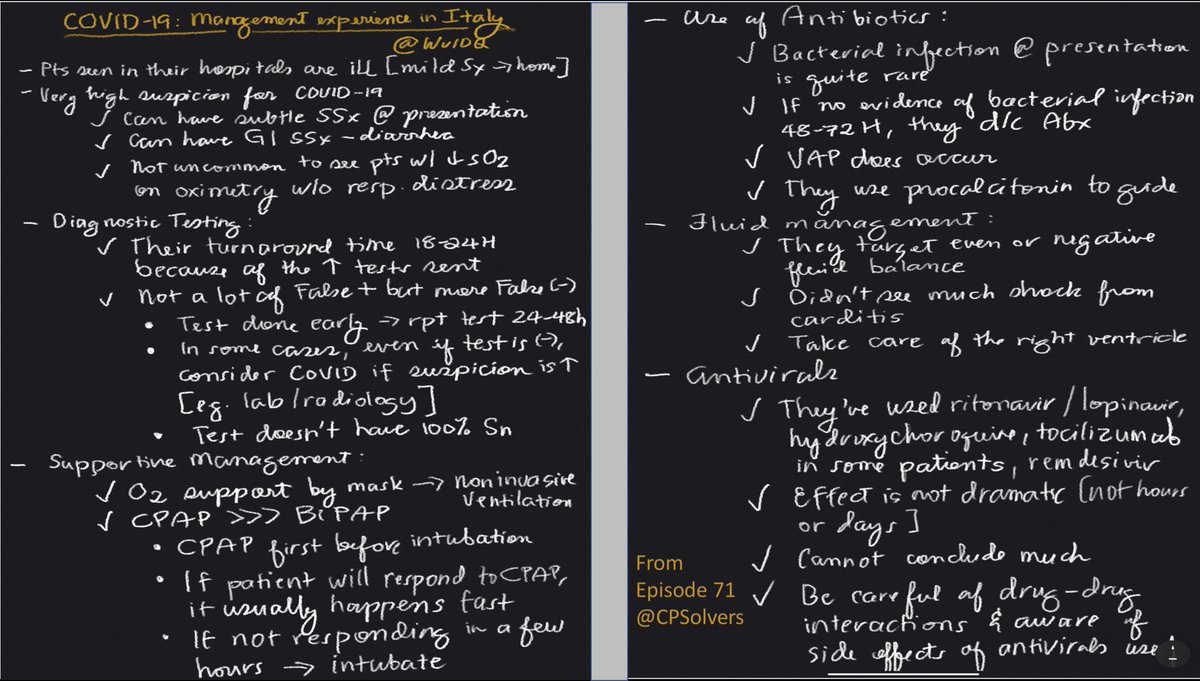
Highly recommended podcast from @CPSolvers. Episode 71:
@DxRxEdu @rabihmgeha interview @GiacomoMonti & @ripamrc on their #COVID19 experience in Milan, Italy.
My notes from this episode👇 @MohitHarshMD @RakheeBhayaniMD @h_babcock @JenniferSpicer4
Highly recommended podcast from @CPSolvers. Episode 71:
@DxRxEdu @rabihmgeha interview @GiacomoMonti & @ripamrc on their #COVID19 experience in Milan, Italy.
My notes from this episode👇 @MohitHarshMD @RakheeBhayaniMD @h_babcock @JenniferSpicer4