
Of note – this thread does not apply to intubation, bronch and clearly aerosol generating procedures (AGPs).
2/
2/
First, let's be 100% clear, we are only discussing this bc we are in a crisis, and applying “crisis standards of care.” What’s the crisis? Not a new virus.
The crisis is the #PPE shortage that many U.S. medical centers face
(due to abject failure of federal leadership).
3/
The crisis is the #PPE shortage that many U.S. medical centers face
(due to abject failure of federal leadership).
3/
Second, why should you listen to me?
I am following @CDC and @WHO. We docs lecture #antivaxxers and other purveyors of snake oil saying “believe the experts”... well, CDC & WHO are the experts.
5/
I am following @CDC and @WHO. We docs lecture #antivaxxers and other purveyors of snake oil saying “believe the experts”... well, CDC & WHO are the experts.
5/
While not formally trained in infection prevention, I spent 3y as PI of grant looking at best practices in infection prevention in EDs. Spoke w IP leads, and front line workers at >10 US hospitals. >50 interviews, >20 focus groups. Learned best practices. #qualitativeresearch
6/
6/
for more see one IP publication...
A systematic review “Infection Prevention in the Emergency Department” w/ Dr. Stephen Liang
7/
ncbi.nlm.nih.gov/pmc/articles/P…
A systematic review “Infection Prevention in the Emergency Department” w/ Dr. Stephen Liang
7/
ncbi.nlm.nih.gov/pmc/articles/P…
So “Does #COVID19 spread by airborne transmission, like TB (tiny particles spread thru air over great distances & time) OR respiratory droplets, like Flu, released w cough/sneeze, but fall out of air bc of gravity, becoming fomites that spread when we touch eyes/nose/mouth”
8/
8/
2ndary question is “What procedures might aerosolize #COVID19, meaning airborne precautions should be followed. Specifically, does collecting an nasopharyngeal swab to test for COVID19 create aerosols as this is most common procedure?”
9/
9/
Rule #1 about the “evidence”. there is no evidence as we typically speak of it…the disease is 3 months old! That’s longer than it takes to get through peer review in normal times. There are a handful of studies, of varying quality, some not through typical peer-review.
11/
11/
Rule #3 There is difference btw demonstrating viral RNA in air & demonstrating infectivity of humans/cells. Swipe a surface or collect air, amplify RNA w/ PCR, & u proved that viral RNA was present. BUT to show infectivity you must take that swab & infect cells (cell culture)
13/
13/
What would ideal evidence look like? Cluster RCT of hospitals using droplet vs aerosol precautions, comparing HCW infections. Reasonable study: observation study comparing diff countries or facilities w diff policies & comparing HCW infections. These won't happen for awhile.
14/
14/
study #1
March 16 @AnnalsofIM “COVID-19 & Risk to Health Care Workers: A Case Report”
15/
annals.org/aim/fullarticl…
March 16 @AnnalsofIM “COVID-19 & Risk to Health Care Workers: A Case Report”
15/
annals.org/aim/fullarticl…
1 patient w severe pneumonia, later determined to have #COVID19 “41 health care workers were identified as having exposure to aerosol-generating procedures (AGP) for at least 10 mins at a distance of <2m from patient.”
16/
16/
Methods:
“All 41 health care workers were placed under home isolation for 2 weeks, with daily monitoring for [Sx]. In addition, they had NP swabs scheduled on day 1 of home isolation, & 2nd swab on day 14 after exposure.”
17/
“All 41 health care workers were placed under home isolation for 2 weeks, with daily monitoring for [Sx]. In addition, they had NP swabs scheduled on day 1 of home isolation, & 2nd swab on day 14 after exposure.”
17/
So what happened???
“NONE of the exposed health care workers developed symptoms, and all PCR tests were negative
18/
“NONE of the exposed health care workers developed symptoms, and all PCR tests were negative
18/
“85% of HCWs were exposed during AGP exposed while wearing surgical mask & remainder were wearing N95 masks. That none of the HCWs in this situation acquired infection suggests that surgical masks, hand hygiene, & other standard procedures protected them from being infected"
19/
19/

"Our observation is consistent with previous studies that have been unable to show that N95 masks were superior to surgical masks for preventing influenza infection in health care workers”
??? remain
20/
??? remain
20/
Study #2
March 17, @NEJM letter “Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1”
This was NOT a clinic study. It was an experiment in a lab.
21/
nejm.org/doi/full/10.10…
March 17, @NEJM letter “Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1”
This was NOT a clinic study. It was an experiment in a lab.
21/
nejm.org/doi/full/10.10…
“Aerosols containing #COVID19 were generated with the use of a three-jet Collison nebulizer and fed into a Goldberg drum to create an aerosolized environment”” SARS-CoV-2 remained viable in aerosols throughout the duration of our experiment (3 hours)”
22/
22/
“Our results indicate that aerosol and fomite transmission of SARS-CoV-2 is PLAUSIBLE, since the virus can remain viable and infectious in aerosols for hours and on surfaces up to days (depending on the inoculum shed).”
23/
23/
Key word: “plausible” It is also possible that the viral RNA caught in aerosols is not enough to infect actual humans. This study did not test cell culture for viral infection. So it is 2 steps removed from whether surgical mask is sufficient or N95 is needed.
??? remain
24/
??? remain
24/
to be continued...
25/
25/
Study #3
March 26, “Transmission Potential of SARS-CoV-2 in Viral Shedding Observed at the University of Nebraska Medical Center”
NOTE: ***pre-print = no peer review, meaning anything besides methods is sorta like this thread***
26/
medrxiv.org/content/10.110…
March 26, “Transmission Potential of SARS-CoV-2 in Viral Shedding Observed at the University of Nebraska Medical Center”
NOTE: ***pre-print = no peer review, meaning anything besides methods is sorta like this thread***
26/
medrxiv.org/content/10.110…
“One Sentence Summary: SARS-CoV-2 is shed during respiration, toileting, and fomite contact, indicating that infection may occur in both direct and indirect contact.”
…let’s dig deeper
27/
…let’s dig deeper
27/
Studied 13 patients with COVID19 “managed in the Nebraska Biocontainment Unit (NBU)”
For airborne transmission they collected “high volume air samples, and low volume personal air samples”
What about infectivity? They did cell-culture
28/
For airborne transmission they collected “high volume air samples, and low volume personal air samples”
What about infectivity? They did cell-culture
28/
“Air samples that were +for viral RNA by PCR were examined for viral propagation in cells. Cytopathic effect WAS NOT OBSERVED in any sample, to date, & immunofluorescence & western blot HAVE NOT, so far, indicated presence of viral antigens suggesting viral replication.
29/
29/
The abstract is “conclusiony”
including suggesting airborne spread
"Disease spread through both direct (droplet & person-to-person) as well as indirect contact (contaminated objects & airborne transmission) are indicated, supporting the use of airborne isolation precautions.”
30/
including suggesting airborne spread
"Disease spread through both direct (droplet & person-to-person) as well as indirect contact (contaminated objects & airborne transmission) are indicated, supporting the use of airborne isolation precautions.”
30/

KEY TAKEAWAY: virus all over the #COVID19 ward
“Taken together, these data indicate significant environmental contamination in rooms where patients infected w SARS-CoV-2 are housed & cared for, regardless of the degree of symptoms or acuity of illness.”
need cleaning & HH!
31/
“Taken together, these data indicate significant environmental contamination in rooms where patients infected w SARS-CoV-2 are housed & cared for, regardless of the degree of symptoms or acuity of illness.”
need cleaning & HH!
31/
Summary of 3 studies. The clinical evidence on masks is from a case report of 1 patient & 41 HCWs.
The 2 studies suggesting airborne transmission showed RNA particles can be amplified from air, but didn't infect live cells or humans.
Verdict: not enough evidence=uncertainty
32/
The 2 studies suggesting airborne transmission showed RNA particles can be amplified from air, but didn't infect live cells or humans.
Verdict: not enough evidence=uncertainty
32/
What else do we have?
@AtulGawande wrote an article “Keeping the Coronavirus from Infecting Health-Care Workers: What Singapore’s and Hong Kong’s success is teaching us about the pandemic” in which he reviewed the infection prevention practices in Singapore & HK.
key passage:
33/
@AtulGawande wrote an article “Keeping the Coronavirus from Infecting Health-Care Workers: What Singapore’s and Hong Kong’s success is teaching us about the pandemic” in which he reviewed the infection prevention practices in Singapore & HK.
key passage:
33/
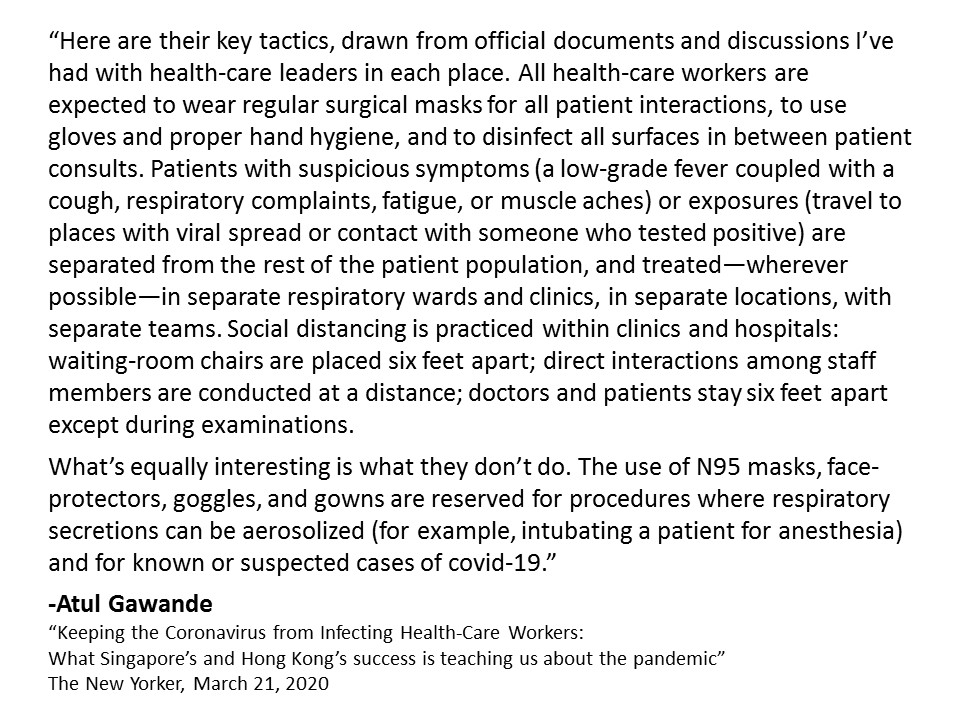
I read this & came away more reassured that #COVID19 is unlikely to spread by airborne transmission. But, he didn’t answer the ? about what they did in Singapore and HK when collecting an NP swab.
Why so important? Bc in U.S. we are conserving N95 masks, so WE DON”T RUN OUT.
34/
Why so important? Bc in U.S. we are conserving N95 masks, so WE DON”T RUN OUT.
34/
I know that many major and well-respected U.S. health systems are not considering NP swab collection aerosolizing, so the HCW collecting NP swab wears a surgical mask, NOT an N95.
35/
35/
Also emailed colleagues in Singapore and Hong Kong (email is amazing) and asked: “Do you wear N95s for collecting NP swabs?” Both said yes, but they think its more than needed.
37/
37/
“Although NPS is not considering AGP, we, in HK, have stepped up to use N95 for NPS from the very beginning. We know WHO recommends surgical mask is good enough but psychology of our HCW is also taken into consideration”
GREAT QUOTE! HCW psychology key
but what N95 shortage?
38/
GREAT QUOTE! HCW psychology key
but what N95 shortage?
38/
So when faced w/ limited supply of N95 masks, I would prefer to only use them now for aerosol generating procedures so we will have a supply in weeks to come, when the pandemic will be worse & we will have more sick patients. When we get more masks, we will change protocols.
39/
39/
Finally – I understand HCWs are angry and nervous. I am also.
We want someone to blame.
There are people to blame --the federal leaders who did not do their jobs preparing our country, and delayed us locally in doing ours.
40/
We want someone to blame.
There are people to blame --the federal leaders who did not do their jobs preparing our country, and delayed us locally in doing ours.
40/
We don’t have N95 masks b/c Trump team didn’t do their job.
So we are now left to choose between Bad option A and Bad option B. (HT @GovRaimondo)
#getusPPE
41/
So we are now left to choose between Bad option A and Bad option B. (HT @GovRaimondo)
#getusPPE
41/
In closing, I am choosing to believe the experts @WHO
When me get more masks, I will re-examine.
end/
When me get more masks, I will re-examine.
end/
@threadreaderapp unroll
glad to see others feel similarly.
good short article about what to do if you face N95 article
"This One Is for the Health Workers at the Front Lines"
good short article about what to do if you face N95 article
"This One Is for the Health Workers at the Front Lines"











