
1/ Thread on our paper reporting unfair accumulation of malnutrition in particular intersectional social gps & geographies in India; we id 4 clusters of dts (hotspots); instead of separately for stunting, wasting & underweight, we use CIAF; > comprehensive 
2/ Paper co-authored with @SabujosephK & @yogishcb & Sangeetha Joice; equityhealthj.biomedcentral.com/articles/10.11…
3/ High stunting (>46 m children) & wasting (>25 m) in India; 5th highest prevalence of u-weight & 3rd highest prevalence of wasting; unfair patterning of child malnutrition by caste, sex, religion, location and socio-economic position already well characterised;
4/ This perverse pattern of unfairly high rates in already socially disadvantaged communities contributes to inter-generational inequities that these groups face; these underlying social drivers are likely causal as well as get aggravated further by childhood malnutrition;
5/ inequitable physical, mental & cognitive effects on children; malnutrition well characterised by caste, economic position, gender and location (urban/rural), but how is it at their intersections? For eg. how does economic position interact with caste wrt child malnutrition?
6/ And what about many other such intersectional groups? Some intersectional analysis is available & hotspots identified but these have been done for anthropometric failures individually (stunting, wasting & u/weight);


7/ Joe et al use Wt-for-age (which includes elements of stunting & wasting); Or for eg. Simantini Bandhopadhyay's intersectional analysis using stunting; here too, the underlying theoretical framing of need for intersectional groups is well outlined;
8/ they (like us) rely on the work of Gita Sen & Aditi Iyer (on which more later) to identify gps; ID of geo-spatial clusters & inter/intra dt level inequalities of child malnutrition has also been done; Khan et al on spatial heterogeneity & correlates;


9/ Liou et al on g/s wealth disparity patterns wrt malnutrition; Menon et al's decomposition analysis & Singh et al; Khan & Mohanty's paper carries separate maps showing geo distribution of stunting, wasting & u/weight; they also visualise bivariate relationships b/w (a)…

10/ …poverty vs stunting (b) poverty vs underweight (c) poverty vs wasting across districts of India; Liou examine distributions of within-state district-wide wealth disparity (the absolute % point diff b/w the highest and lowest wealth quintiles) in several parameters;
11/ While stunting->chronic, wasting->acute, u/w is a composite of both phenomena; they're distinct biological phenomena & a composite ind'l measure prbably not useful; at population level, a comprehensive measure of anthropometric failure useful to id unfair accumulations
12/ Hence , we use Svedberg's composite index of anthro failure (CIAF) as an aggregated population level indicator of stunting, wasting & u/w with 6 gps: A- no failure, B- only wasted, C- u/w and wasted, D- stunted, wasted and u/w, E- stunted and u/w, F- only stunted.

13/ To these, Nandy et al.added Y- only u/w; allows for id children with multiple anthropometric failures at population level; children with 3 co-occurring failures obv have highest mortality & morbidity risk; so, in our paper we characterise CIAF across intersectional gps;
14/ Given that policies & programs such as POSHAN & state Govts look at districts as actionable entities with their own governance, the use of CIAF analysis could help with better identifying critical districts/geographies;
15/ Methods: CIAF constructed from child anthropometric data in NFHS4; concentration curve plotted to examine economic inequality in caste; chloropleth maps using GeoDa & descriptive analysis of district-level CIAF prevalence; also categorised districts as high, medium & low;
16/ Using the high, med & low district cats for 3 & 2 failures, we further id critical, very serious & serious; our categorisation likely composite of intersectional sub-groups & multiple failures (CIAF) which we must compare with other such lists created in earlier works
17/ On intersectional gps, we followed Sen et. al.; they point how the lack of conceptualisation of intersectionality causes several questions to not even be asked; their work in Koppal (Karnataka) has shown how to apply these groups in practice; see pubmed.ncbi.nlm.nih.gov/21741737/

18/ We reduced some to binaries; eg. wealth quintiles recoded to poor & non-poor; for caste, SC & ST coded separately while OBC and other castes grouped as Other. From these re-coded cats, 24 intersecting sub-gps; prevalence of CIAF for each calculated.
19/ The adjusted OR of CIAF among each of these intersectional groups were calculated using logistic regression keeping Other-Non-Poor-Urban-Male as the reference.
20/ non-overlapping 95% CI of OR used to infer significance in the difference between gps (based on non-overlapping CI); overall CIAF of 55.32% among children (cf. 38.4% stunting, 35.7% u/w & 21% wasting NFHS-4.
21/ 22.15% of children suffer from 1 failure, whereas 26.55% have simultaneous 2 failures & 6.62% have all 3! stunting & u/w (18.33%) is the highest reported type of failure.
22/ ST Poor children disadvantaged both in rural & urban areas compared to SC Poor and Other Poor; ST Poor Male Rural children have the highest simultaneous 3 forms (12.60%), whereas the ST Poor Male urban children have the highest undernourished (71.90%).
23/ In CIAF too, economic position is strongly linked to nutritional status; large diff in CIAF b/w children from poor & non-poor; non-poor advantage irrespective of gender, caste, and place of residences; highest proportion of ST children with simultaneous 3 failures
24/ But ST children lowest rate of inequality by wealth indicating uniform poorness in this gp?
25/ In OBC & general, spread of households across all economic positions is seen (unequal growth in fact creates these inequalities within groups!) & hence inequalities higher (cf ST & SC);
26/ CC of SC demonstrated shifting trend; poorest wealth quintile of SC & ST start together but with improving economic position in SC group makes a departure; improved Econ position? mitigating nutritional adversities similar to OBC & general among uppper socio-econ SC.

27/ CIAF by intersectional sub-groups unsurprisingly not uniform; Econ. position difference in all 3 failures among ST children is significant only in rural areas, whereas among the urban areas this difference disappears irrespective of gender.

28/ Among SC, except urban male, all gps report econ position-based diff; Among OBC & Gen econ position-based diff is consistently significant irrespective of gender & location; takes male-ness & urban-ness to have population level protective effect on caste inequality;
29/ In caste-based comparison of all-3 failures, ST & SC difference only in poor male rural; difference between ST and GEN is consistently significant in rural areas irrespective of gender difference; for poor male rural children, caste continues to matter wrt all-3 failures;…
30/ …Caste-based inequality continues in CIAF; for poor male rural, non-poor female rural, non-poor female urban, non-poor male rural, caste inequality in CIAF glaring;

31/ Rural girls disadvantage irrespective of econ position in all three failure; no significant diff b/w rural & urban coudl be demonstrated; In dts identified as critical, nearly half (> 45%) of children reported at least two simultaneous failures.
32/ Among critical dts, the Dangs district from Gujarat reported a shocking 60% of children with at least two failures. From Bihar & Jharkhand two districts each & from Chhattisgarh, Karnataka, MP, Rajasthan, Uttar Pradesh, & WB 1 district each was reported as critical


33/ Among the very serious districts, Pashchimi Singhbhum district in Jharkhand with 64.7% of children with at least 2 failures nearly met criteria for critical (u/w & wasting prevalence 11.5%; all-3-failures 21.2%; and stunting & u/w 32%).

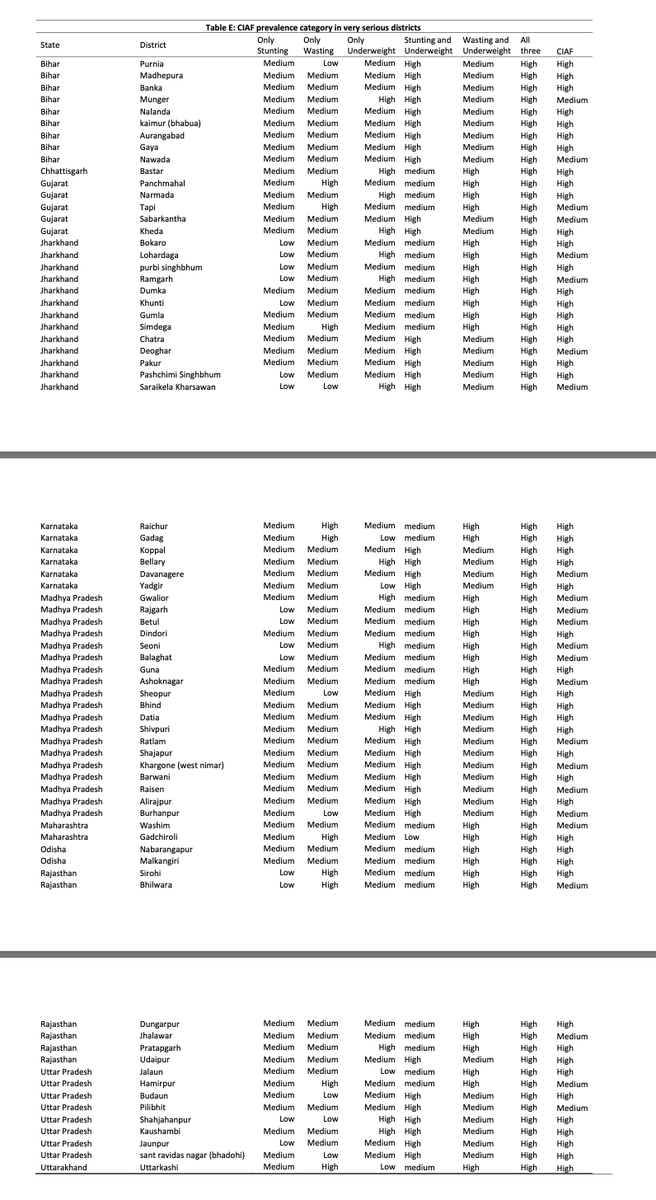
34/ The highest number of very serious districts are reported from MP (19 dts!), followed by Jharkhand (13 dts). Gujarat has the highest number of serious districts (8 districts) followed by Odisha (4 dts)


35/ Overall spatial distribution of critical, very serious and serious district-level prevalence shows geographical clustering in 4 undernutrition hotspots spanning 12 high burden states.

36/ In south India, a cluster of eight districts in north Karnataka forms the undernutrition hotspot. The 2nd hotspot is 11 districts along the state boundaries of Chhattisgarh (4), Odisha (6)and Maharashtra (1).
37/ The 3rd hotspot is spread across borders between WB, Bihar & Jharkhand consisting of 28 districts, of which 11 from Bihar, 3 from WB & 14 from Jharkhand. The fourth hotspot is 53 districts spanning across MP (23), Rajasthan (7), Gujarat (17), Maharashtra (4) & UP (2).
38/ Clustering of undernutrition across CIAF-based hotspots of 2 & 3 dimensional anthropometric failures confirms the need for strategies that target larger eco-geographical zones across districts & states.
39/ Consider inter-sectoral approaches involving agroforestry & food security targeted at disadvantaged intersectional groups; Earlier studies have identified 225 undernutrition hotspot districts based on separate undernutrition measures (either stunting, wasting or u/w).
40/ we apply comprehensive measures of undernutrition and assess co-occurring failures, id 111 districts that appeared to be most in need of action. we also classify these 111 districts into critical, very serious and seriously affected districts based on the urgency of action.
41/ The districts we identify possibly have higher disadvantages due to the clustering of multiple failures.
42/ Interestingly, 6 districts identified as serious (Mahesana and Amreli in Gujarat, Ratlam, Harda, and Shahdol in Madhya Pradesh, and Bankura West Bengal) were not among the undernutrition hotspots identified in previous studies.
43/ All the critical and very seriously affected districts in our study have been identified in the single-axis analysis by Khan & Mohanty.
44/ Our study hotspots are mostly clustered in hot and semi-arid climate and is also associated with subsistence cultivation of millets & poverty-driven lack of dietary diversity & other social factors; requiring interdisciplinary approaches to identify drivers of clustering.…
45/ …In another effort we try to explain eco-geo pattern linking subsistence millet cultivation to malnutrition thru poverty-driven(?) sole dependence on subsistence millets (hence lack of protein & diversity); but limited data & concerns by reviewers! wellcomeopenresearch.org/articles/5-118
46/ Although hotspot id is helpful for national-level priority setting, there are several districts in better-off states which continue to have vulnerable groups and undernutrition pockets within districts.
47/ For eg, in Kerala, the nutritional status among ST is better than national avg of ST frm NFHS 4; however, there is still high prevalence of undernutrition reported 82.9, 83.6, and 82% of stunting, underweight & wasting; see our paper on this ijph.in/article.asp?is…
48/ Uniform ST poorness limits understanding role of econ position in improving child nutrition; over-reliance on market/individual choice might break up the solidarity that somewhat protects from adverse social structures; (our review on this here) journals.sagepub.com/doi/full/10.11…
49/ Also ST population mostly in rural & remote forested areas, significantly higher risk of ST children from rural areas by economic position, caste and gender in undernutrition point towards urgent and more focused intervention among ST children from rural households.
50/ The risk factors of child undernutrition: poverty, drinking water & toilet, illiteracy, & poor access to healthcare are worse among ST; several ongoing "free schemes" are clearly not working & require meaningful community engagement; see equityhealthj.biomedcentral.com/articles/10.11…
51/ Shifting CC in all three failures for SC seems to suggest better social mobility compared with the ST.
52/ Consistent with these, previous studies reported that although both SC & ST communities are disadvantaged, SC data shows higher mobility in income, education, employment status, and political representation.
53/ The intersectional analysis shows that nutritional inequality between ST and SC is clustered in rural areas.
54/ While economic position based nutritional inequality is more consistently significant in both urban & rural areas for SC and other caste, caste-based nutritional inequality is clustered in rural areas.
55/ This could mean that in urban context, households could(?) overcome caste-based disadvantages, whereas economic impediments persist in achieving child nourishment in both rural and urban areas.
56/ Rapid urbanisation, combined with rural to urban migrations, mainly of the rural poor, has been associated with increasing inequalities in Indian cities.
57/ Increased clustering of urban poor (by caste?) in slums characterised by limited access to public health and nutrition services and amenities along with other known risk factors for undernutrition such as a high density of population, poor quality drinking water,…
58/ …inadequate sanitation facilities, and unhygienic conditions could be the plausible explanation for diminishing the apparent urban advantage for the poor among SC and other castes.
59/ Further, urban poverty too is not uniformly distributed across states; there is a high concentration of urban poor in the poorer states in central and north India, possibly contributing to the greater hotspots in these states.
60/ Inter-state and regional variations in urban migration and rural-urban inequalities in child undernutrition in India may reveal different regional patterns. </end>
@threadreaderapp unroll
• • •
Missing some Tweet in this thread? You can try to
force a refresh




