Doing a 🧵 of @EM_RESUS’s thread with screenshots.
We see a lot of screenshots of what is wrong in #SciComm.
What went right here? How can one doc transmit knowledge & confidence to another so well via a series of tweets?
We see a lot of screenshots of what is wrong in #SciComm.
What went right here? How can one doc transmit knowledge & confidence to another so well via a series of tweets?
https://twitter.com/EM_RESUS/status/1268585193809551361
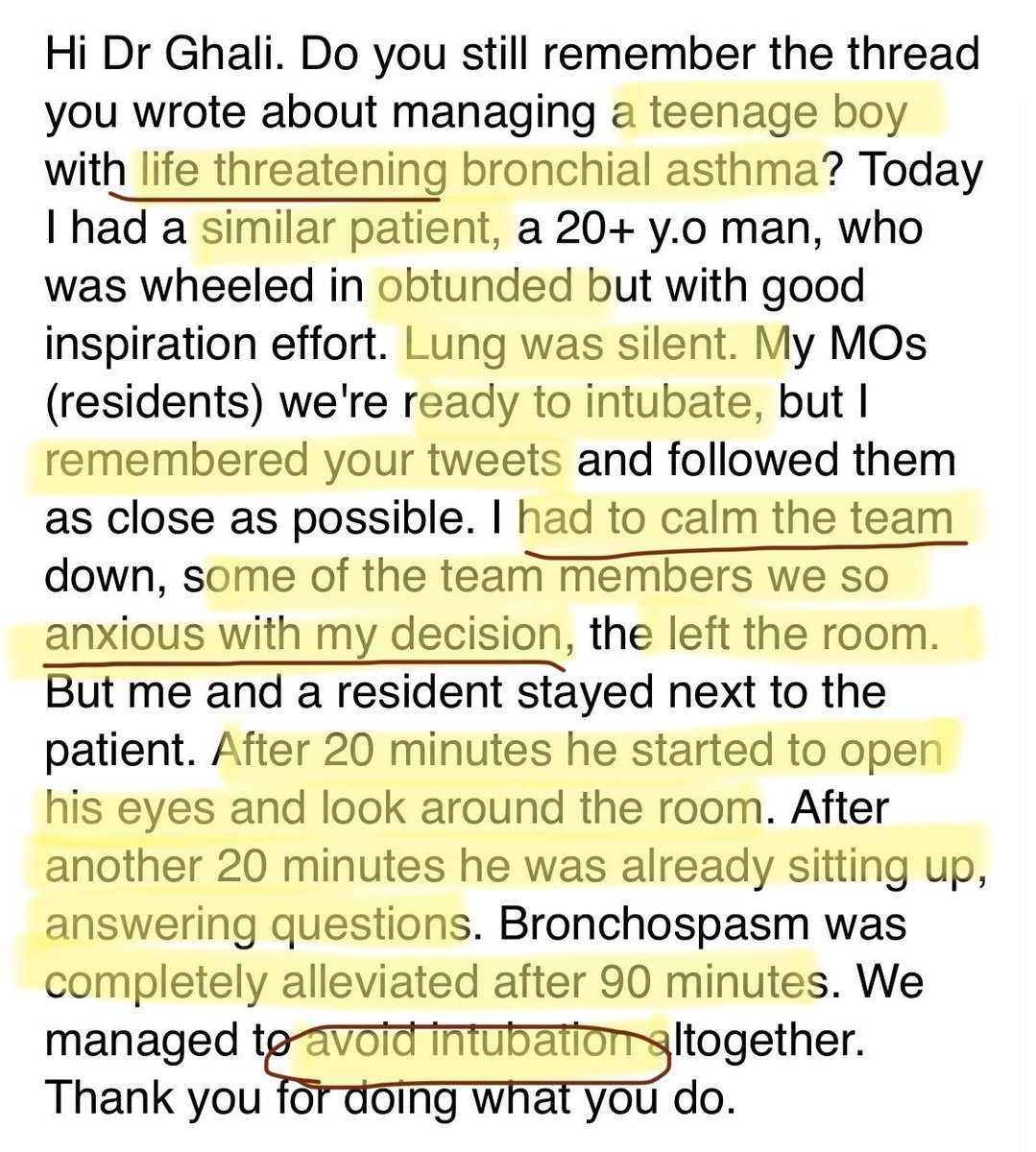
First: what was the outcome of the #SciComm? Intention matters little as communitarian happens on the terms of the listener/reader. How was your #communication received/understood?
A doc:
recognized similar scenario
calmed team
avoided overaggression
achieved a similar result
A doc:
recognized similar scenario
calmed team
avoided overaggression
achieved a similar result
The fact that the #MedEd teaching allowed an EQ & #leadership outcome (staying course despite others’ anxiety), not merely medical knowledge/journal club, is striking. How was this achieved? Let’s look at the thread. How do you transmit courage AND knowledge via tweets in a 🧵?
How does he start?
NOT with #data
NOT with a diagnosis
NOT a journal club
With a human being
A visual description
A family
Emotions
If in #emergencymedicine you recognize this right away
It triggers a memory or few
You will recognize it when you see/feel it
#SciComm
NOT with #data
NOT with a diagnosis
NOT a journal club
With a human being
A visual description
A family
Emotions
If in #emergencymedicine you recognize this right away
It triggers a memory or few
You will recognize it when you see/feel it
#SciComm

Next set of tweets. More visuals. Emotional tension, the pressure to “save” (via intervention).
You are still in the room in this scenario. This is masterful narrative medicine without violating patient privacy.
Only one data point.
Walks you through YOUR emotions, reassures.
You are still in the room in this scenario. This is masterful narrative medicine without violating patient privacy.
Only one data point.
Walks you through YOUR emotions, reassures.

After acknowledging what you’re feeling & your human reaction or bias to action, slows down your brain to “System 2”
Now, physiology
Engages your intellect & memory of how lungs work & what positive pressure ventilation does (in this case, harm/death)
Then: correct action
Now, physiology
Engages your intellect & memory of how lungs work & what positive pressure ventilation does (in this case, harm/death)
Then: correct action


This is boom, boom, boom actions. Meds.
But still, human acknowledgement of nurses.
And where he wants you to remember, says it several times. Doses given of individual doses & total.
And explanation is why combineb or why give steroids early
This aids retention.
But still, human acknowledgement of nurses.
And where he wants you to remember, says it several times. Doses given of individual doses & total.
And explanation is why combineb or why give steroids early
This aids retention.

Same as above

This is a turning point clinically and you see the descriptive nature come back. What are you seeing, hearing, & why?
You transition out of only “do” mode
and because you did NOT overreact, did NOT paralyze & sedate & intubate
you can observe mental status
connect as a human
You transition out of only “do” mode
and because you did NOT overreact, did NOT paralyze & sedate & intubate
you can observe mental status
connect as a human

This is SO important. A busy #emergencymedicine doctor could leave at this point and the patient could crash then the doc blamed for not intubating. Instead, you are reminded that mental status includes anxiety that could affect clinical status.
Then reinforces the main point.
Then reinforces the main point.

Given that 🧵, yes, it achieved success as #SciComm to communicate high quality, compassionate, humane, family-centered care that helps the doc (feeling the need to play hero) to manage self & stay logical, aware, make good choices under pressure & despite dissent/disagreement.
To summarize what @EM_RESUS did well in 🧵
-describes human aspects
-walks you thru your bias to action to “take control of the airway”
-activates System 2 thinking to engage on physiology/mechanisms
-repeats critical points
-clear precise med/BIPAP instructions
-end with human
-describes human aspects
-walks you thru your bias to action to “take control of the airway”
-activates System 2 thinking to engage on physiology/mechanisms
-repeats critical points
-clear precise med/BIPAP instructions
-end with human
Entire tweets in the 🧵with no/limited data ➡️get you to focus on what important.
Any parrot can memorize. An octopus has dexterity ..so ok..you can intubate? Whoopdidoo. None of that saves lives.
Being able to *see*, *hear*, assess, consider & respond (not react) saves lives.
Any parrot can memorize. An octopus has dexterity ..so ok..you can intubate? Whoopdidoo. None of that saves lives.
Being able to *see*, *hear*, assess, consider & respond (not react) saves lives.
& when others around you have anxiety & want heroic action, resisting bias to action or need to feel in “control” is HARD
stay confident, stay aware of the physiology/anatomy, calm others
➡️don’t kill the patient with aggressive over intervention/your anxiety
=#quality care
stay confident, stay aware of the physiology/anatomy, calm others
➡️don’t kill the patient with aggressive over intervention/your anxiety
=#quality care



As I’ve been asked, yes, please do share & use this 🧵 based off a 🧵 in any way that you see fit
Tweets are public property
Can be used by anyone
If this helps you teach attendings or senior residents how to teach interns/juniors, go for it. I’m adding to @EM_RESUS #MedEd🧵
Tweets are public property
Can be used by anyone
If this helps you teach attendings or senior residents how to teach interns/juniors, go for it. I’m adding to @EM_RESUS #MedEd🧵
• • •
Missing some Tweet in this thread? You can try to
force a refresh