
1a) Welcome to a 🆕#accredited #tweetorial on the importance of time in range #TIR in #diabetes . . . with additional emphases on #primarycare and on practice in 🇨🇦.
#FOAMed #endotwitter #MedEd @MedTweetorials #nephtwitter #cardiotwitter
#FOAMed #endotwitter #MedEd @MedTweetorials #nephtwitter #cardiotwitter
1b) Hence we welcome2⃣ expert faculty from Canada: Ilana Halperin @ilanajhalperin, academic endocrinologist at @Sunnybrook and @uoftmedicine, and Noah Ivers @NoahIvers, #familydoc & researcher at Women's College Hospital @UofT 


2) Earn 0.75hr 🆓CE/#CME by following this🧵! This program is supported by an unrestricted educational grant from Sanofi Canada and is intended for #HCPs. Statement of accreditation & faculty disclosures at cardiometabolic-ce.com/disclosures/.
And so we begin . . .
And so we begin . . .
3a) @NoahIvers 👨: I was asked to do a #tweetorial on Time in Range (#TIR) in Primary Care. My initial response was sorry I think you have the wrong doctor in our house
3b) 👨: How about my wife @ilanajhalperin 👩 ?, I thought . . . After all, she has a large population of #T1D patients and is a huge advocate for the benefits of technology in that population.
4) @ilanajhalperin 👩: Actually, there is growing evidence of the benefits of continuous glucose monitoring #CGM to help improve #TIR in Type 2 Diabetes and we know most care for #T2D happens in #PrimaryCare
See 🔓 pubmed.ncbi.nlm.nih.gov/36443083/ and 🔓 ncbi.nlm.nih.gov/pmc/articles/P…
See 🔓 pubmed.ncbi.nlm.nih.gov/36443083/ and 🔓 ncbi.nlm.nih.gov/pmc/articles/P…
5) 👨: I was always taught to target #A1C - isn’t that what the guidelines say, per 🔓 guidelines.diabetes.ca/cpg/chapter-9-… ?
6) 👩: A1C is useful for diagnosing #T2D, predicting complications on a population level, but we certainly see patients with the same A1C for the same duration of time & other risk factors optimized, but different burdens of micro- and macrovascular complications.
7) 👩: This paradox is because for the same A1C the mean glucose can vary widely, for example one A1C of 7.5% could be a mean glucose of 7 and for a different patient it represents a mean glucose of 9 mmol/L. See 🔓 pubmed.ncbi.nlm.nih.gov/18540046/

8) 👨: So, what exactly do you mean by Time in Range for patients I would see in my #familypractice? Like, let’s talk about a patient who is on 2-3 meds and I am contemplating #basal #insulin because #A1C is above target. I’m usually still thinking about A1c there…
9a) 👩: Great question, I prefer to talk about Time in RangeS. From #CGM a number of glucose metrics can be derived:
9b) 👩: Time Below Range (further divided in <3.9 and very low <3.0 mmol/L) Time in Range 3.9-10mmol/l and Time Above Range (subdivided into high 10.1-13.8mmol/L and very high >13.9 mmol/L). See 🔓 pubmed.ncbi.nlm.nih.gov/31177185/
10) 👨: Ok, I get that, but let’s be honest, in primary care when I’m seeing pts w/#DM who also have knee pain + 3 other issues, I still don’t understand how I would use it in practice. When do I start thinking about this, & in those moments, how can I fit it into my workflow?
11)👩: Fair point, I think a picture will really help to make it real.
For most adults the #TIR goal is 70%, with <4% #TBR and 25% #TAR. The TIR goal is relaxed to 50% for frail adults in an effort to avoid hypoglycemia.
🔓 pubmed.ncbi.nlm.nih.gov/31177185/
For most adults the #TIR goal is 70%, with <4% #TBR and 25% #TAR. The TIR goal is relaxed to 50% for frail adults in an effort to avoid hypoglycemia.
🔓 pubmed.ncbi.nlm.nih.gov/31177185/

12a) 👩: In addition to #TIR, I like to look at measures of glucose variability and the ambulatory glucose profile (#AGP), which is a graphical representation of the glucose profile over 14 days.
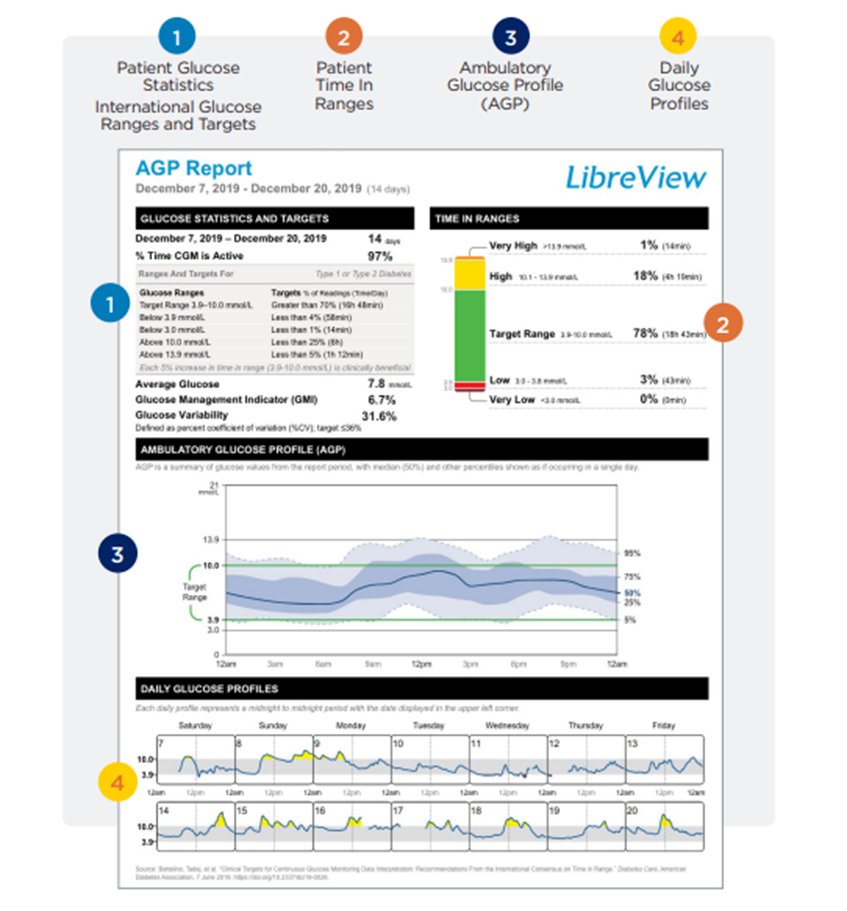
12b) 👩:T his picture allows you to visually pinpoint the time(s) of day when specific glycemic patterns exist and when glucose levels repeatedly deviate from the target range. Having knowledge of the patient's typical mealtimes, sleep, and exercise on the #AGP is helpful
13) 👩: When looking at the #AGP ask yourself
1- Is there a problem (Look for #hypoglycemia, #hyperglycemia, or both)
2- Where (when) is the problem (fasting or post prandial)
3- How to adjust therapy
See pubmed.ncbi.nlm.nih.gov/35930313/ .
1- Is there a problem (Look for #hypoglycemia, #hyperglycemia, or both)
2- Where (when) is the problem (fasting or post prandial)
3- How to adjust therapy
See pubmed.ncbi.nlm.nih.gov/35930313/ .


14) 👩: Now in this picture are 3 #AGP reports for the same “in target” #A1C. What's hiding beneath is glucose variability: expressed as coefficient of variation, when CV <36% glucose are stable and >36% glucose levels are unstable (meaning higher risk for hypoglycemia)

15) 👨: So, if my pt gives me a report from their machine saying variability is high - greater than 36% - what do I do with that? I mean, really, given all the other things I’m already needing to do in clinic? Give me some real-world examples where this would change what I do?
16a) 👩: When #variability is low you can adjust insulin using the recommendations above. When variability is high you need to discuss the patterns with the patient.
16b) 👩: There are > 30 (!) factors that contribute to glucose variability but most common issues are related to timing of rapid acting insulin administration & the impacts of food & activity. A few helpful ??s to ask pts with high variability are summarized in this graphic:

17a) 👩: Usually I just talk to my patients about how their glucose swings from high to low and back again based on how they respond to highs and lows and they look at me . . .
17b) 👩: . . . with a half smile and say “how did you know that?” I laugh and say it's a common phenomenon for everyone who uses #CGM and rapid acting #insulin.
18) 👩: The key to improving variability is being patient with both the insulin and glucose sensor. I have a publication that discuss this in more detail (pubmed.ncbi.nlm.nih.gov/33046398/). Here are my main talking points for helping patients decrease their variability:

19a) 👩: I think that all of this can seem overwhelming for a PCP and person with diabetes #PWD. So I want to leave you with some basics. Even if you don't know how to interpret an ambulatory glucose profile or adjust therapy to improve #TIR, . . .
19b) 👩: . . . the biofeedback your patients will get from using #CGM is really helpful and can have a significant impact on their glycemic outcomes!


20) 👨: This all sounds promising but what is the evidence for benefit in the population of patients I tend to see in primary care?
21) 👩: Excellent question, The Mobile Study (🔓 pubmed.ncbi.nlm.nih.gov/34077499/) looked at the use of Dexcom G6 a real time #CGM use in patients managed on basal insulin in primary care.

22a)👩: And in the extension study, those who stopped the #CGM saw their gains lost. We can hypothesize this is because the CGM continues to give people with diabetes the right nudges towards healthy behaviors.
22b) 👩: In addition, it’s possible that #PCPs and #PWDs felt safer being more aggressive with basal insulin titration when there were alerts and alarms to protect against #hypoglycemia.
23a) 👩: Another important population is the non-insulin using population. I think if someone is maxed out on non-insulin agents but not reaching their A1C target, a #CGM is the perfect next step!
23b)👩: It may be enough to change their lifestyle and get #A1C to target, but if it is not then you will have the #AGP to help you initiate and adjust #insulin.
24) 👩: In the Immediate Study the authors shows that FreeStyle Libre (intermittently Scanned CGM) and education compared to education alone resulted in a 10% improvement in TIR and 0.5% lowering in A1C. 🔓 pubmed.ncbi.nlm.nih.gov/36546594/

25) So the guidelines are now evolving to recognize this newer evidence.

26a)👨: Ok, I think you have convinced me that #CGM has benefits for #PWDs & their #PCPs; #TIR does make a lot more sense than #A1C & the visual glucose profile can help us quickly identify areas of risk and areas for improvement.
26b)👨: How easy is it for me to prescribe these devices to my patients?
27a) 👩: Ah, the hardest question to answer given we are tweeting to an international audience. In Canada, most people w/ #T2D w/ private or public insurance can get access to #isCGM if they are on insulin. #rtCGM coverage is also improving in the T2D space in private insurance.
27b) 👩: For people not on insulin or w/out insurance a single Free Style Libre sensor that lasts 2wk will cost around CAD$90. In that population, periodic use may be very helpful. They can wear for 2wk before the appt with you & then you have useful data to review together.
27c) 👨: OK, I am going to try to use more of this technology in my practice. I will probably have more questions, but I know where to find you 😉
28a) So let’s close with a couple knowledge ✔️ questions!
First, monitoring #PWDs with #A1c alone misses:
a. Extent or timing of hypoglycemia
b. Extent or timing of hyperglycemia
c. Glycemic variability
d. All of the above
First, monitoring #PWDs with #A1c alone misses:
a. Extent or timing of hypoglycemia
b. Extent or timing of hyperglycemia
c. Glycemic variability
d. All of the above
28b) It’s d. #A1c may predict long-term complications but falls short on providing actionable information for #PWD and #HCPs. Now, for most adult #PWDs, what is target #TIR?
28c) It’s c, > 70%, but as per tweets 9a and 9b above, don’t neglect to check #TBR and #TAR as well to effectively monitor glucose management and limit excursions into hypo- and hyperglycemia.
29) And that’s it! Under the expert tutelage of @ilanajhalperin 👩 & @NoahIvers 👨, you just earned 0.75hr 🆓CE/#CME 🇨🇦🇺🇸🇬🇧🇪🇺. Go to cardiometabolic-ce.com/cardiorenal46/ NOW and claim your credit, and FOLLOW @cardiomet_CE for more expert-delivered #MedEd!
#FOAMed #cardiotwitter #nephtwitter
#FOAMed #cardiotwitter #nephtwitter
• • •
Missing some Tweet in this thread? You can try to
force a refresh












