@matthewherper @sciencescanner A short thread on triglycerides (TG), triglyceride-rich lipoproteins (TRL), coronary artery disease, and medicines development 
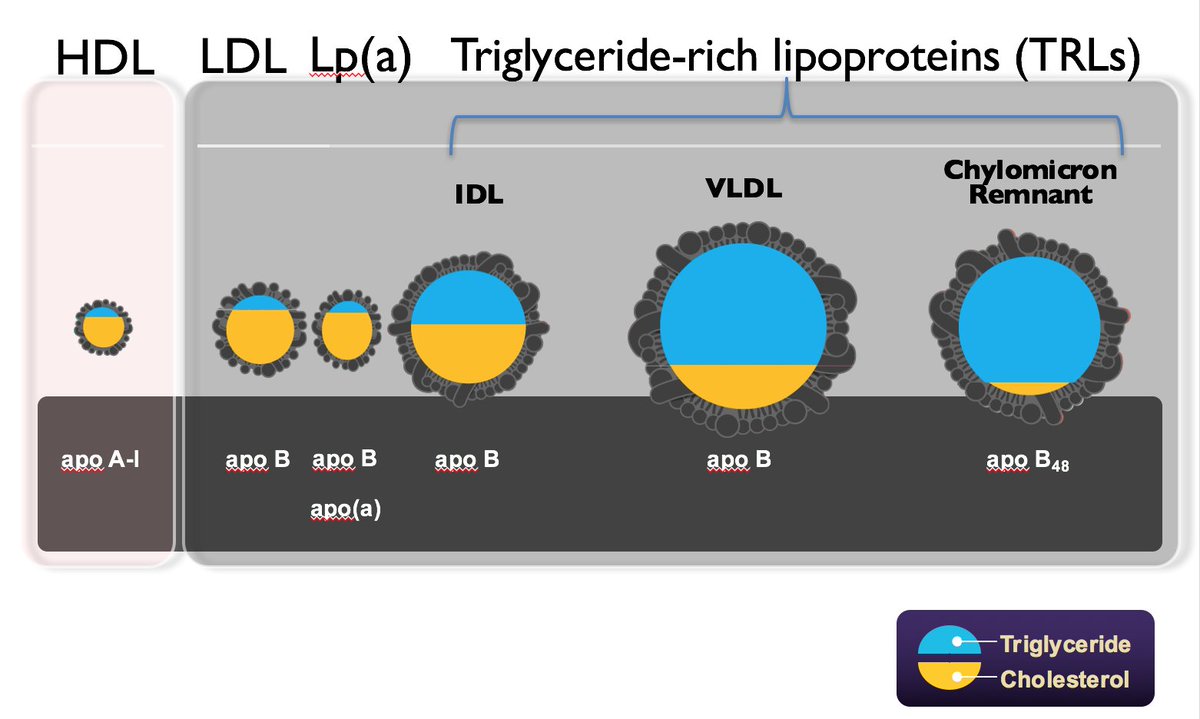
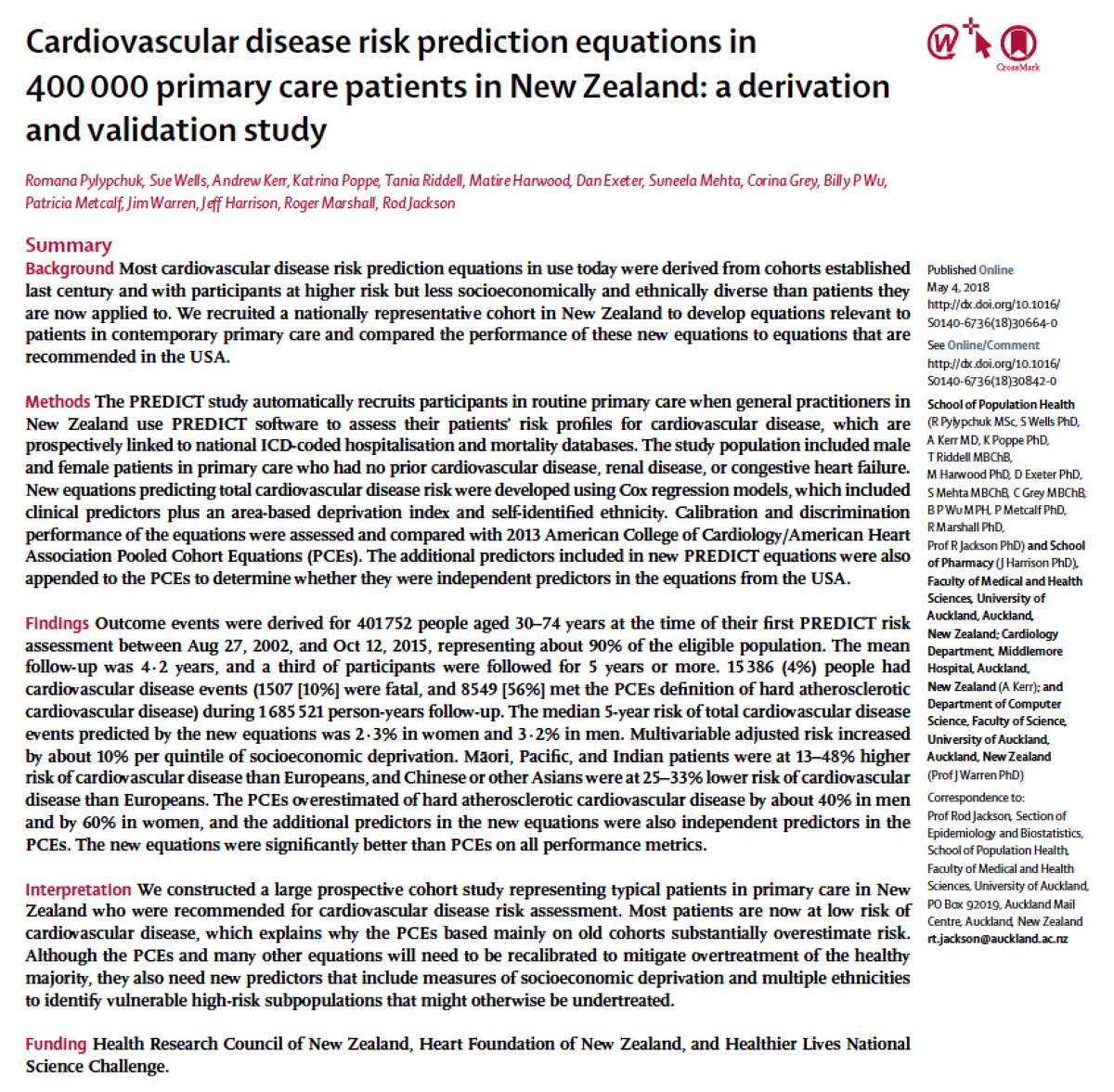
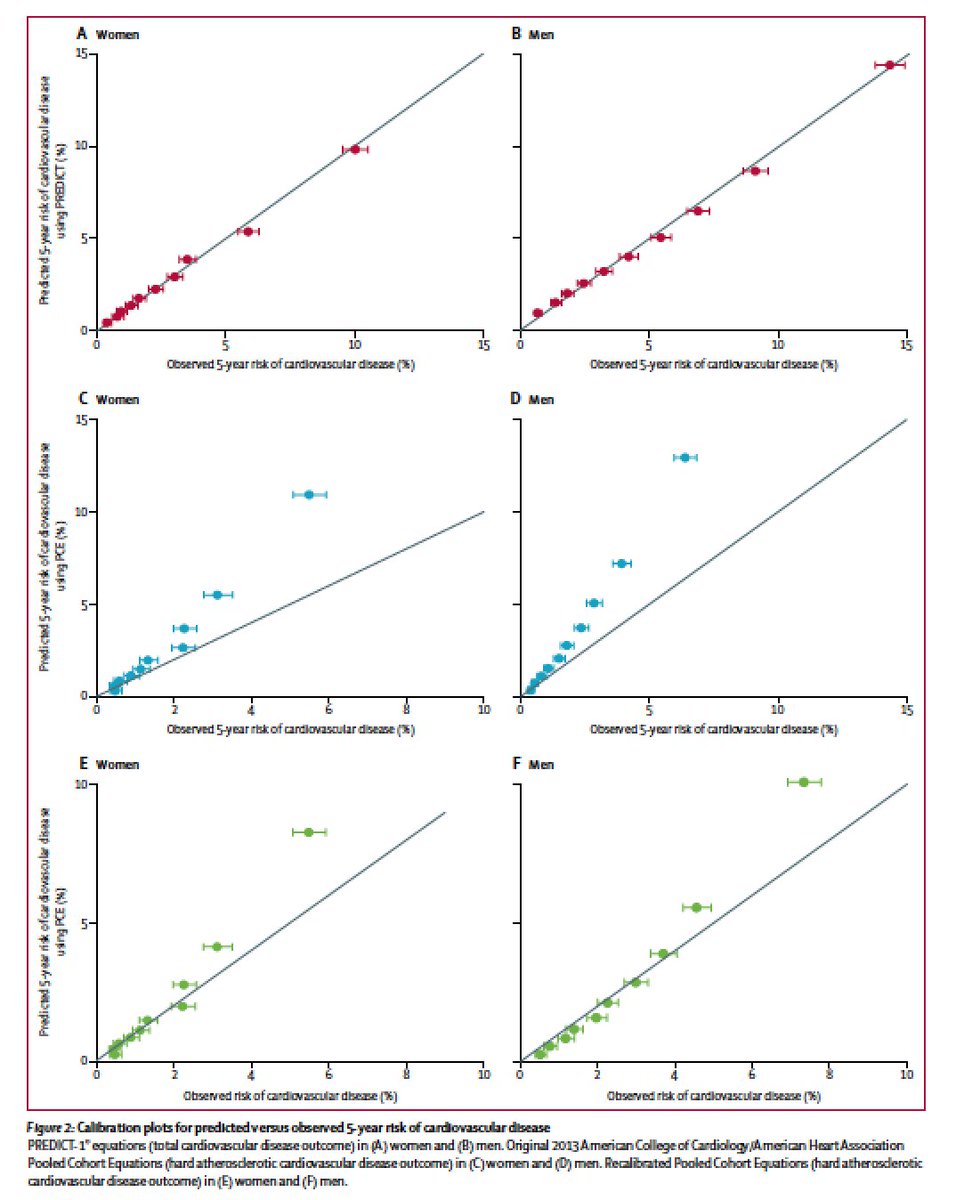
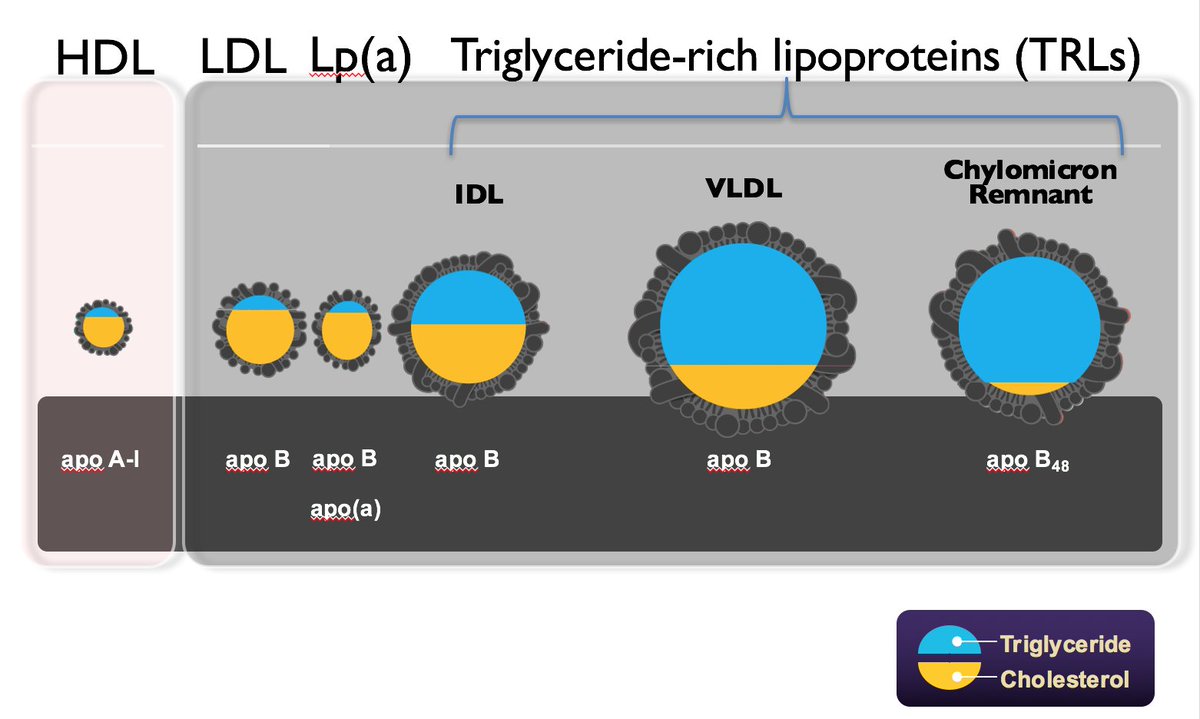
@matthewherper @sciencescanner Lipoproteins: macromolecules that carry lipids in center
We approximate [lipoproteins] by measuring lipids they carry
TG levels approximate [TRLs] (a collection of several particles)
But, TRLs also carry cholesterol
For every 5 mg/dl triglycerides in TRL, ~1 mg/dl cholesterol
We approximate [lipoproteins] by measuring lipids they carry
TG levels approximate [TRLs] (a collection of several particles)
But, TRLs also carry cholesterol
For every 5 mg/dl triglycerides in TRL, ~1 mg/dl cholesterol
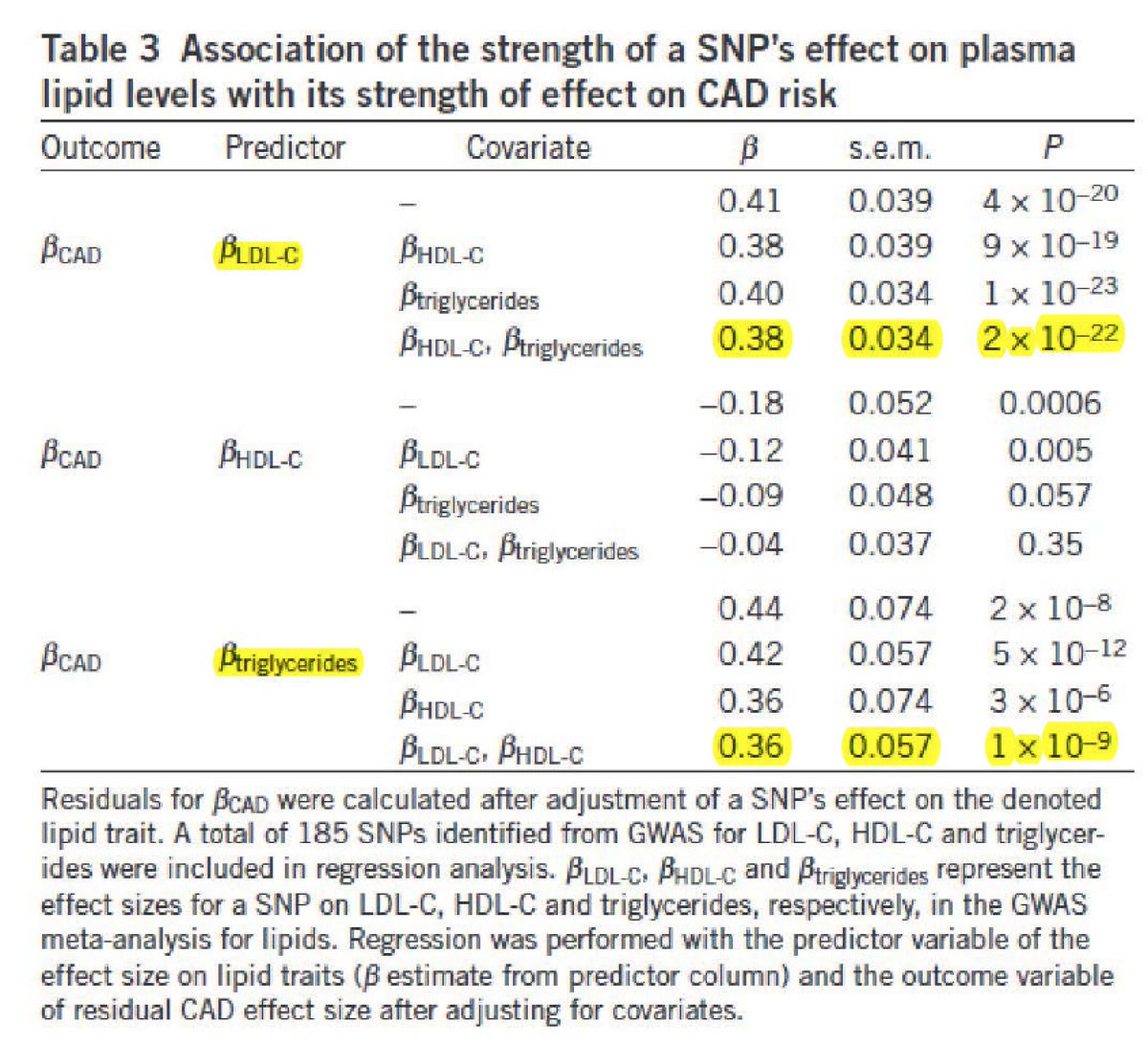
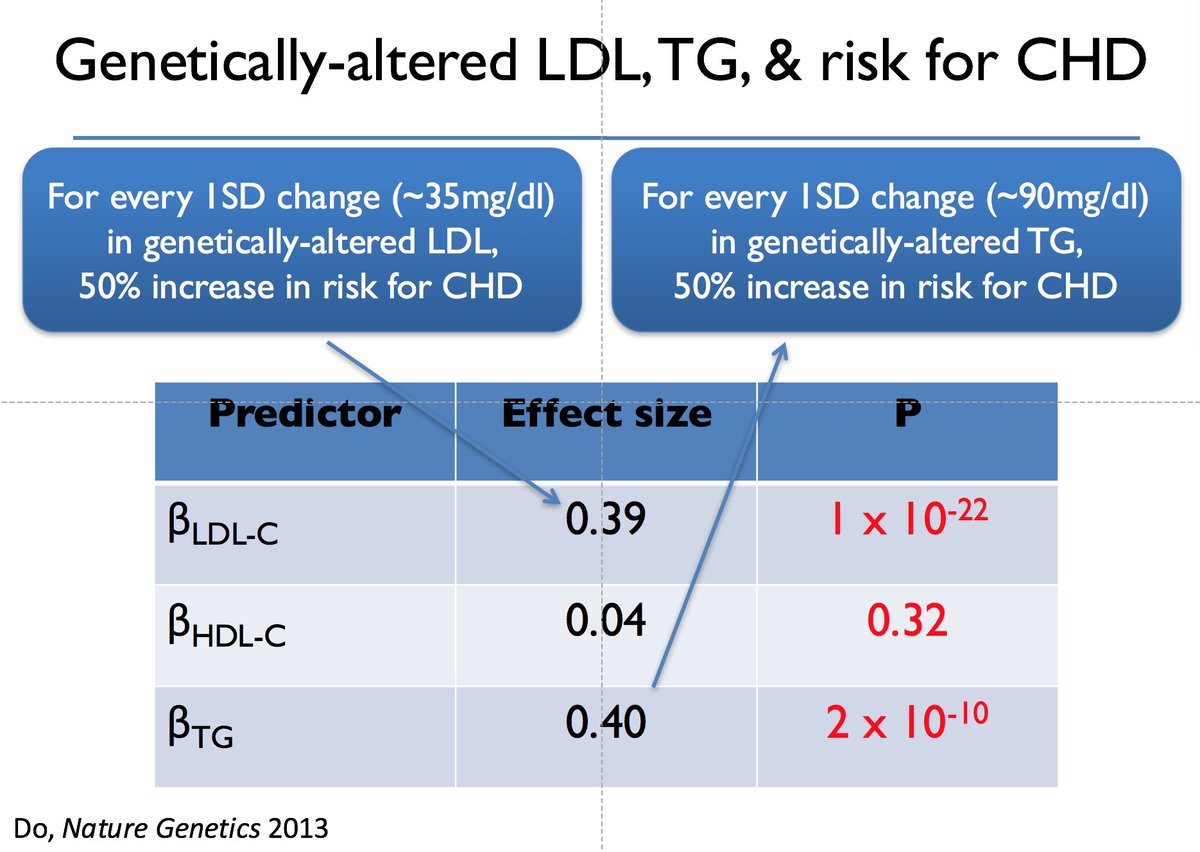
@matthewherper @sciencescanner Genetic studies suggest that after LDL, concentration of TRL ‘causally’ relates to coronary artery disease
See here from 2013
kathiresanlab.org/our-publicatio…
See here from 2013
kathiresanlab.org/our-publicatio…
@matthewherper @sciencescanner But, 3 key unanswered questions:
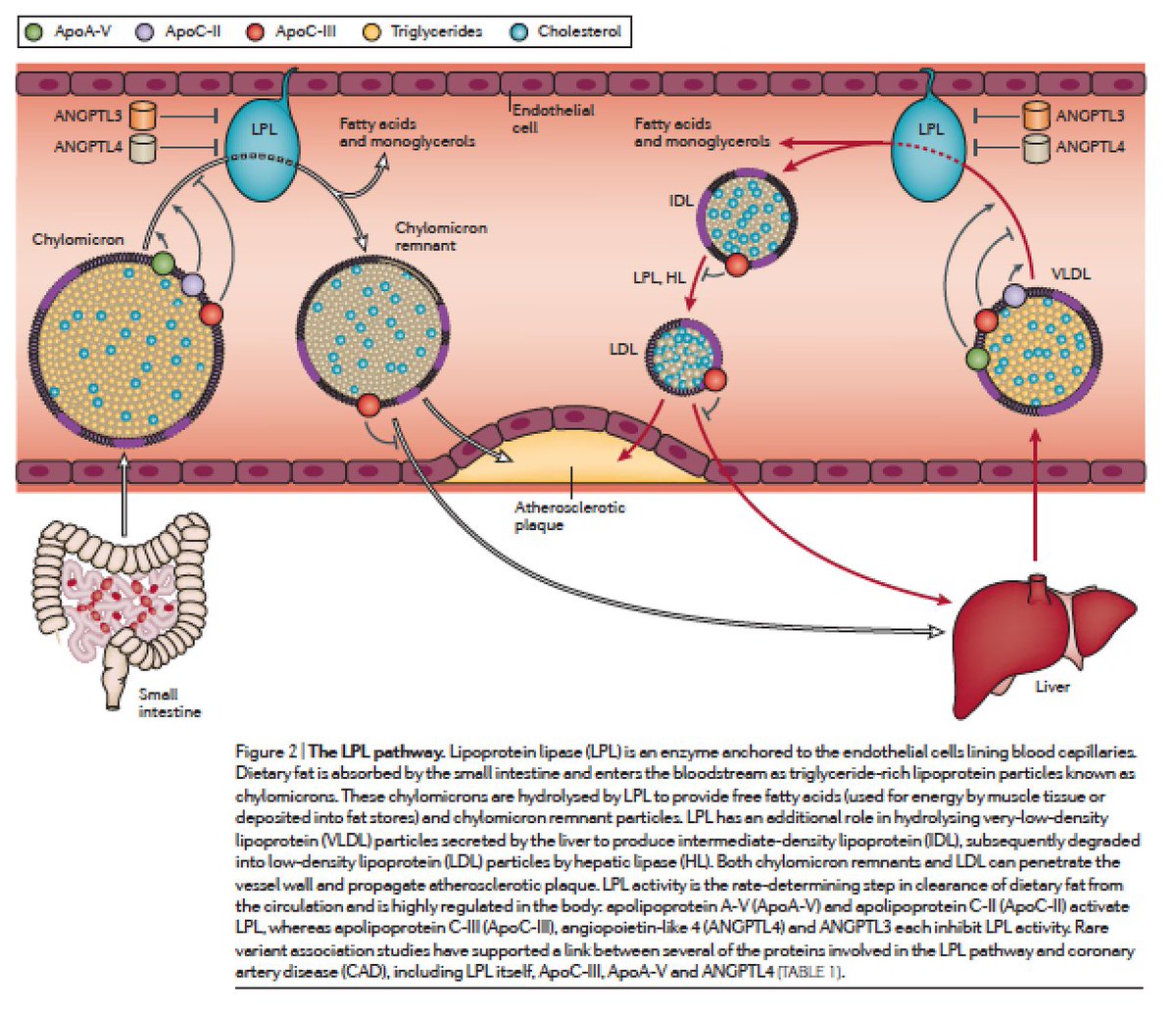
1. will every way of lowering plasma TRL reduce CAD risk?
Best genetic evidence is for one pathway (lipolysis by LPL)
5 genes:
lipoprotein lipase (LPL) and 4 endogenous regulators (ANGPTL3, ANGPTL4, APOC3, APOA5)
kathiresanlab.org/our-publicatio…
1. will every way of lowering plasma TRL reduce CAD risk?
Best genetic evidence is for one pathway (lipolysis by LPL)
5 genes:
lipoprotein lipase (LPL) and 4 endogenous regulators (ANGPTL3, ANGPTL4, APOC3, APOA5)
kathiresanlab.org/our-publicatio…
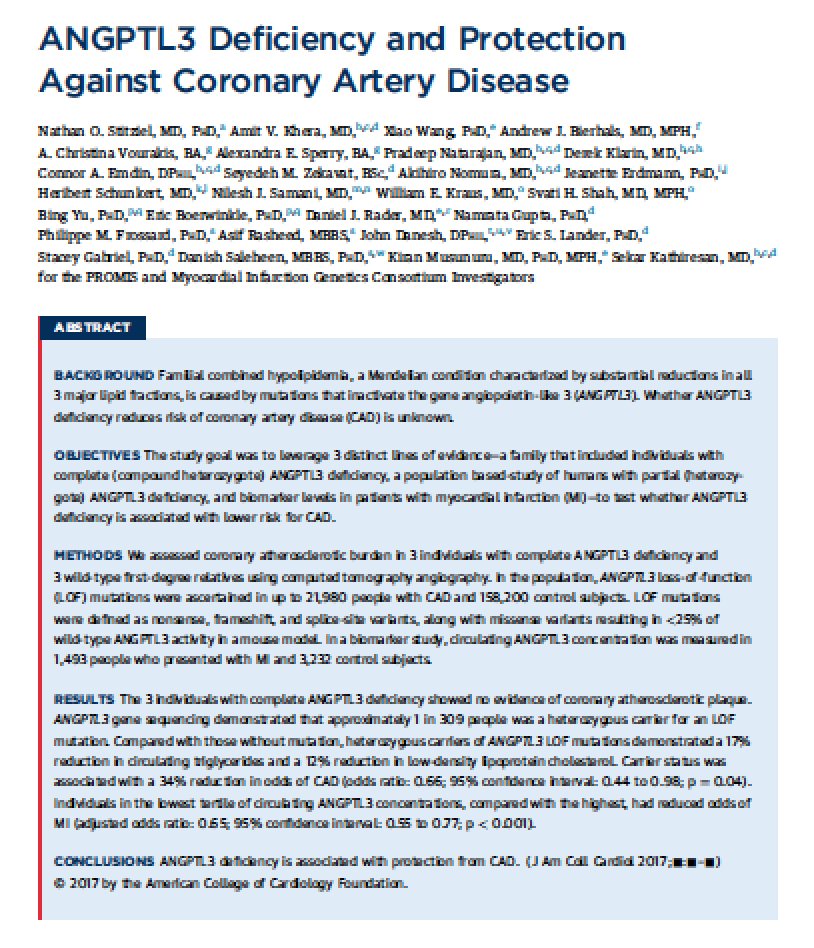
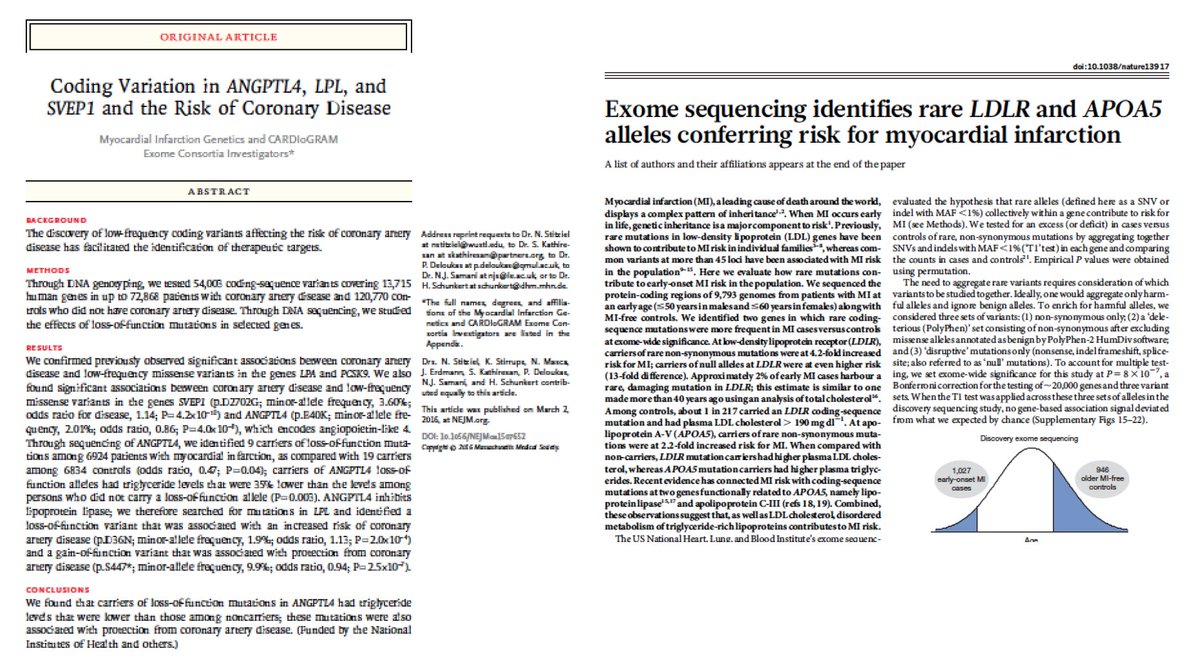
@matthewherper @sciencescanner here are some of the papers re:
rare coding mutations in 5 LPL pathway genes affect CAD risk
rare coding mutations in 5 LPL pathway genes affect CAD risk


@matthewherper @sciencescanner 2. which measure TRL concentration best biomarker for medicines development?
At least 3 options:
blood TG
blood apoB
blood non-HDL-C cholesterol (this is the cholesterol in the LDL and TRL particles)
Report today suggesting that apoB might be best
At least 3 options:
blood TG
blood apoB
blood non-HDL-C cholesterol (this is the cholesterol in the LDL and TRL particles)
Report today suggesting that apoB might be best
@matthewherper @sciencescanner 3. what is dose response relationship of TRL lowering with Rx and CAD?
Our genetic data suggested that for a standard deviation increase in plasma TG (genetic, lifelong, SD ~90mg/dl), 50% higher CAD risk
Flipping for lowering,
90mg/dl lower TG = 33% lower CAD risk
Our genetic data suggested that for a standard deviation increase in plasma TG (genetic, lifelong, SD ~90mg/dl), 50% higher CAD risk
Flipping for lowering,
90mg/dl lower TG = 33% lower CAD risk
@matthewherper @sciencescanner But, above was for genetic/lifelong change
So, need to at-least halve estimate for Rx which is typically < 5y
Now, you get: for every 90mg/dl lower TG with Rx = ~15% lower CAD risk !!!
Are STRENGTH and REDUCE-IT powered for this dose-response?
So, need to at-least halve estimate for Rx which is typically < 5y
Now, you get: for every 90mg/dl lower TG with Rx = ~15% lower CAD risk !!!
Are STRENGTH and REDUCE-IT powered for this dose-response?
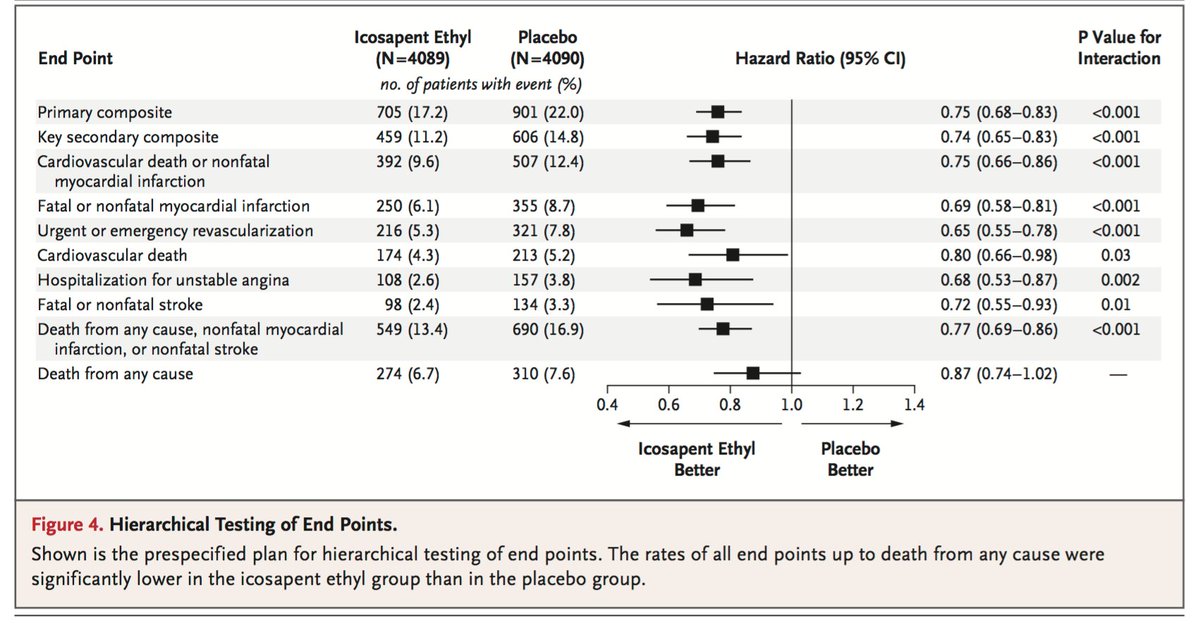
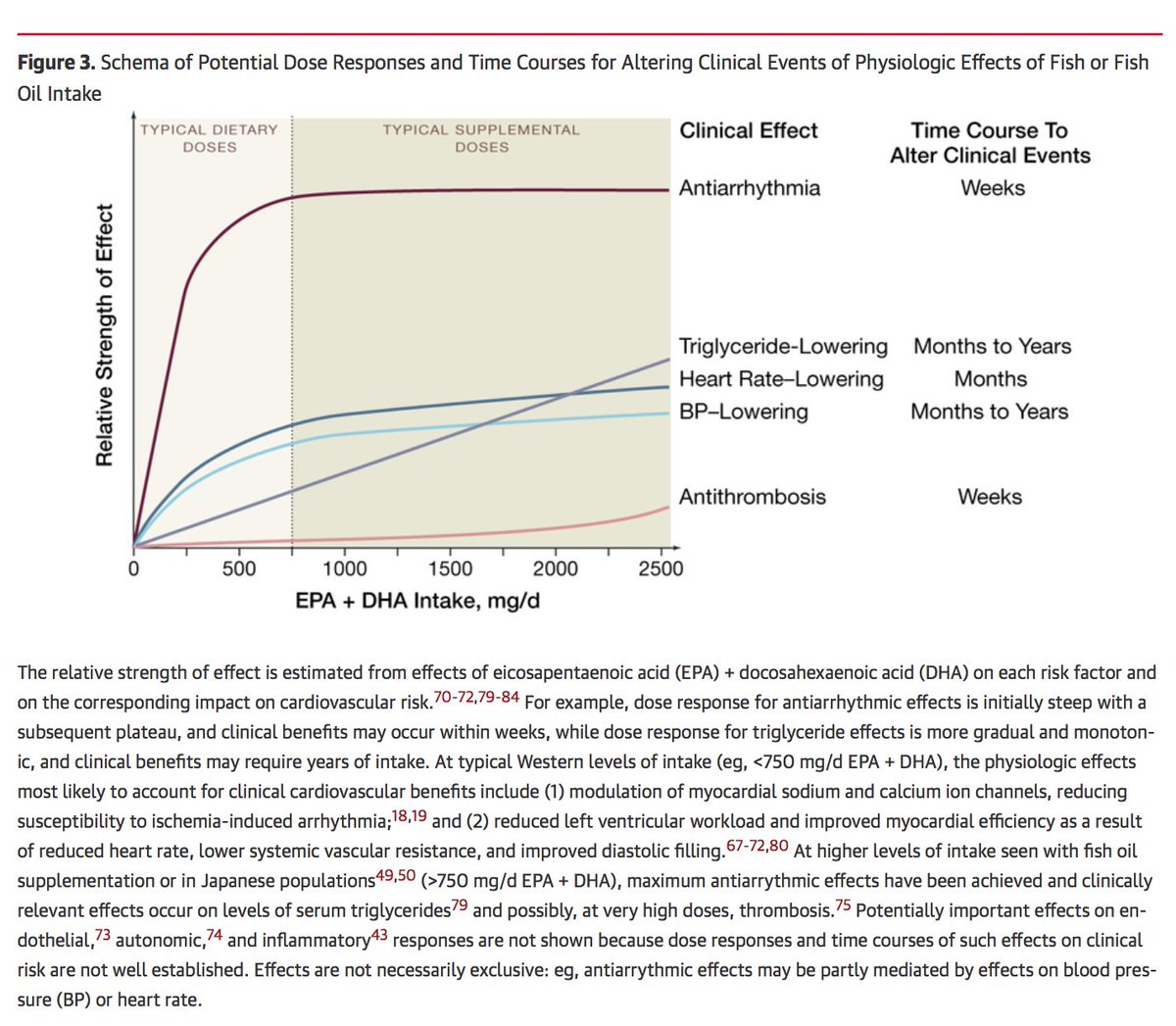
@matthewherper @sciencescanner So, will STRENGTH & REDUCE-IT fish oil RCT of higher dose (3-4 g) and in high TRL populations show efficacy?
Maybe but concerns:
a. don’t know exact target(s) fish oil
b. even if getting at lipolysis pathway, degree TRL lowering may not be enough (studies on margin of power)
Maybe but concerns:
a. don’t know exact target(s) fish oil
b. even if getting at lipolysis pathway, degree TRL lowering may not be enough (studies on margin of power)
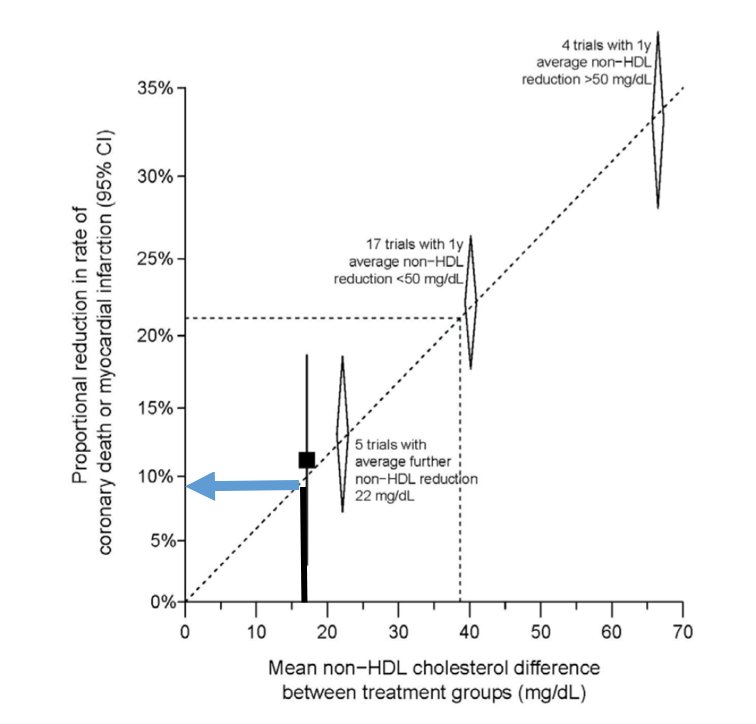
@matthewherper @sciencescanner P.S. Brian Ference has done nice work trying to estimate dose-response relationship.
Simple approach:
Take TG change & divide by 5 to get the cholesterol change.
Then, ask how much that degree of cholesterol would be expected to change CAD risk (based on CTT)
Simple approach:
Take TG change & divide by 5 to get the cholesterol change.
Then, ask how much that degree of cholesterol would be expected to change CAD risk (based on CTT)
@matthewherper @sciencescanner With this approach:
90 mg/dl TG lowering = 18 mg/dl cholesterol lowering
CTT: for every 39 mg/dl cholesterol lowering, about 22% reduction CAD
So, 18 mg/dl chol lowering = 10% reduction in CAD
So, if a fish oil lowers TG by 90 mg/dl, might only get 10% reduction CAD!
90 mg/dl TG lowering = 18 mg/dl cholesterol lowering
CTT: for every 39 mg/dl cholesterol lowering, about 22% reduction CAD
So, 18 mg/dl chol lowering = 10% reduction in CAD
So, if a fish oil lowers TG by 90 mg/dl, might only get 10% reduction CAD!