How likely are you to have a heart attack over next 5y?
Risk prediction model developed in 400K in contemporary New Zealand
Cool study
Thread
thelancet.com/journals/lance…
Risk prediction model developed in 400K in contemporary New Zealand
Cool study
Thread
thelancet.com/journals/lance…
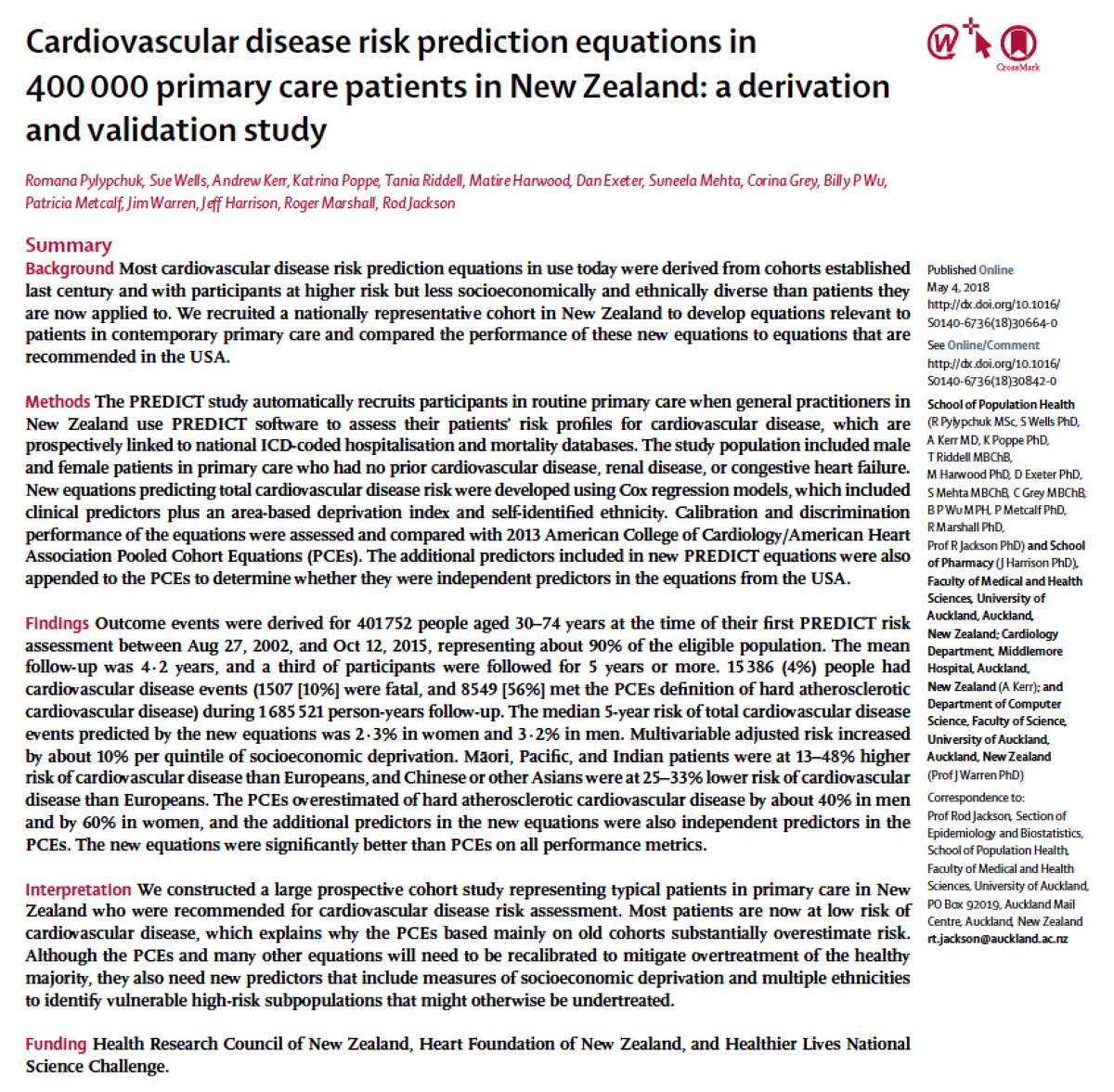
Risk prediction for first CV event is a hard problem.
Without any testing, if you just told everyone that they will *not* have a heart attack over the next 5y, you would be correct >95% of time!
At present, first CV event rates low over 5y period – median 2.3% women, 3.2% men
Without any testing, if you just told everyone that they will *not* have a heart attack over the next 5y, you would be correct >95% of time!
At present, first CV event rates low over 5y period – median 2.3% women, 3.2% men
In US, ACC/AHA Pooled Cohorts Equations (PCE) is recommended
PCE predicted risk used to guide BP and chol Rx
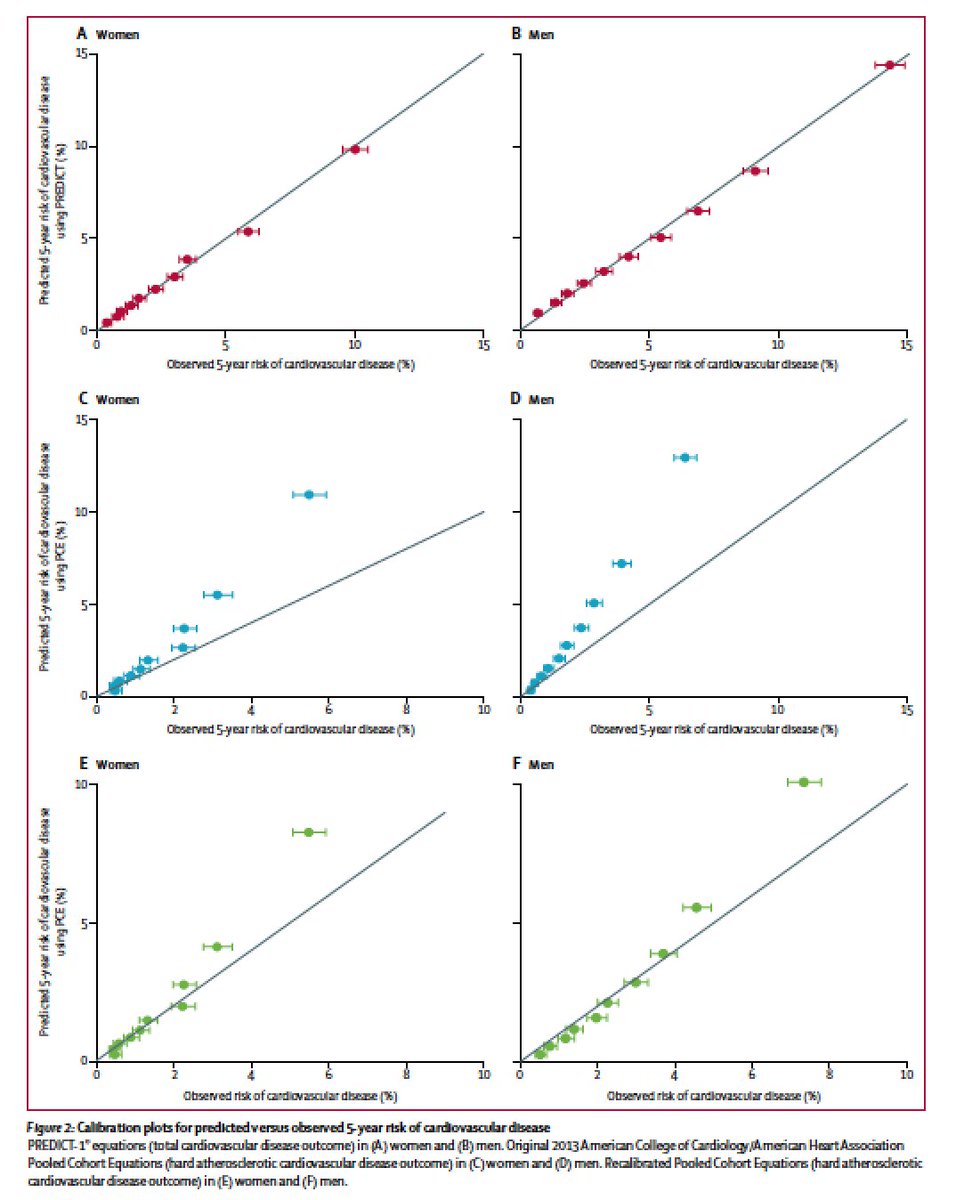
But, in many studies now, PCE predicted risk consistently shown to over-estimate actual observed risk
Same over-estimation by PCE seen in this NZ study (middle panel)
PCE predicted risk used to guide BP and chol Rx
But, in many studies now, PCE predicted risk consistently shown to over-estimate actual observed risk
Same over-estimation by PCE seen in this NZ study (middle panel)
Initial maelstrom re PCE over-estimation set off by Paul Ridker and Nancy Cook (see below) in 2013 when PCE was introduced
Looks like Paul was correct
@ACCinTouch @American_Heart need to seriously consider revising the equations
nytimes.com/2013/11/18/hea…
Looks like Paul was correct
@ACCinTouch @American_Heart need to seriously consider revising the equations
nytimes.com/2013/11/18/hea…
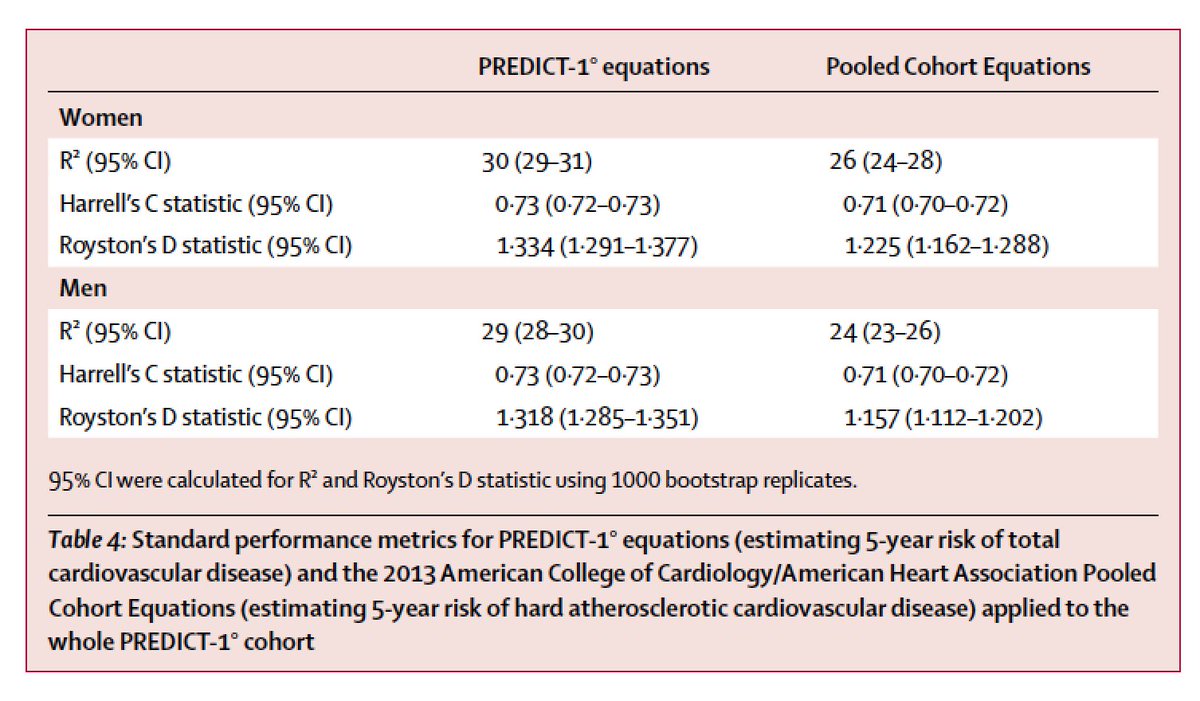
Developing a model in 400K (current study) is likely to be much better than in ~20K (ACC/AHA Pooled Cohorts Equations)
But, AUC of this model is only 0.73!
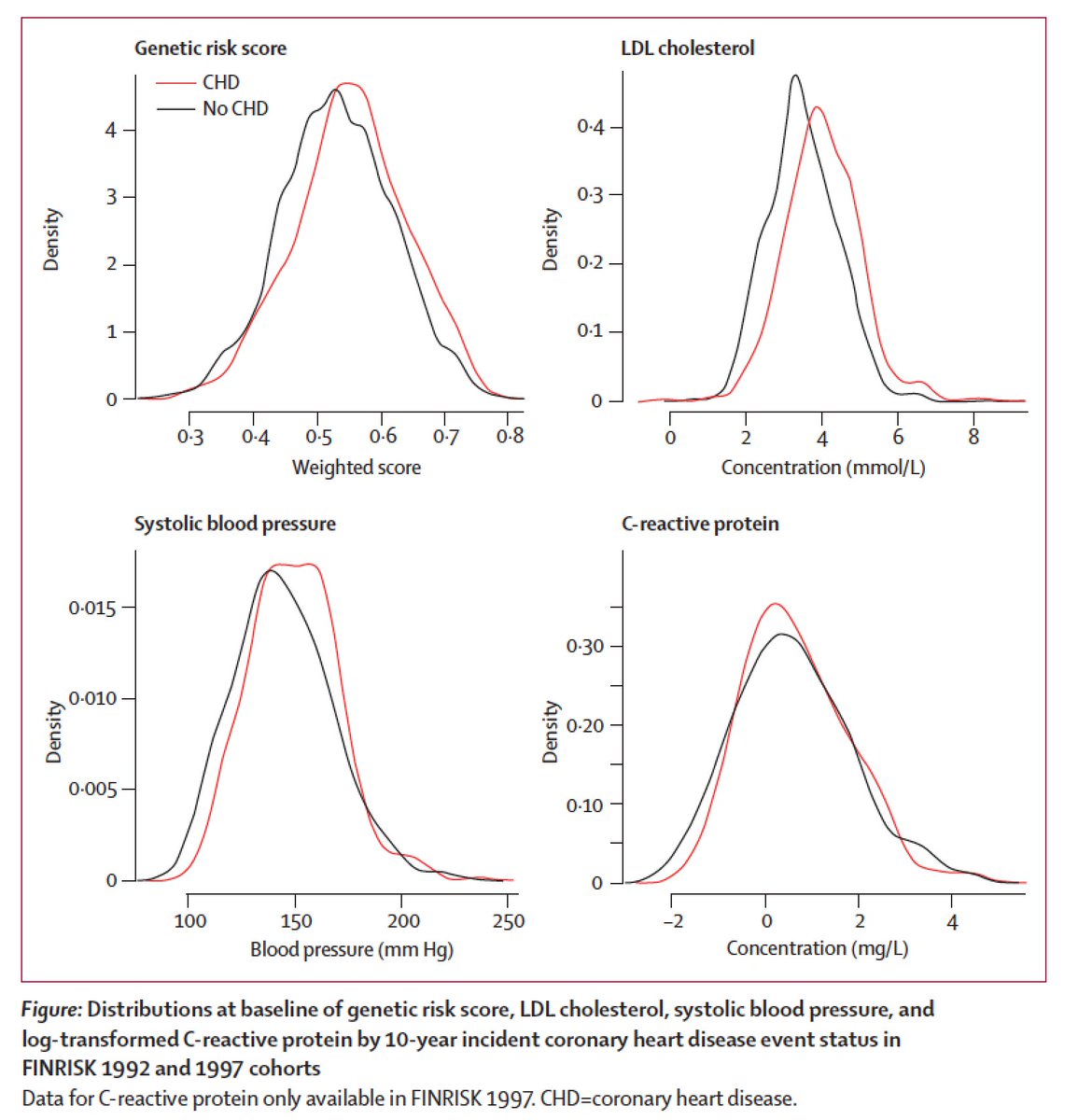
What does AUC 0.71 look like? See below (R) for distributions of factors with AUC ~0.7 in event/non-events
But, this is the way it is for any complex disease which is the result of many inputs with no single input being deterministic
What does AUC 0.71 look like? See below (R) for distributions of factors with AUC ~0.7 in event/non-events
But, this is the way it is for any complex disease which is the result of many inputs with no single input being deterministic
Age remains biggest predictor (ie. in pop’n, older you are, more likely to have a heart attack).
And thus, these models limited utility for men 30-50, women 40-60 as all will be predicted to be low-risk
Germline genetic risk assessment may help here
And thus, these models limited utility for men 30-50, women 40-60 as all will be predicted to be low-risk
Germline genetic risk assessment may help here
Finally, new approaches such as AI applied to prediction may improve situation
(can’t close a thread in 2018 without mention of AI/deep learning) 😀
Finis
(can’t close a thread in 2018 without mention of AI/deep learning) 😀
Finis