,
21 tweets,
8 min read
Read on Twitter
I will share my #SCAI2019 talk. 
This was the suggested workflow from our group in 2014. #whyCMR was considered a downstream test due to a lack of understanding on what it has to offer. Now it has become the to-go test in our center to assess for cardiac Amyloidosis.
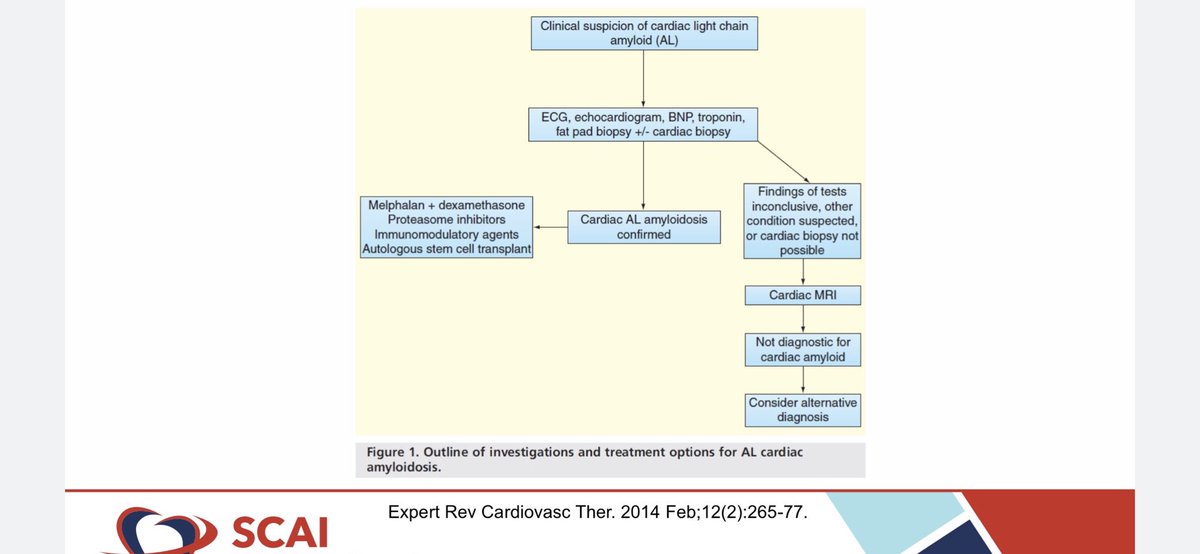
Congo red from biopsy, no longer needed for cardiac Amyloidosis, I’ll show you why

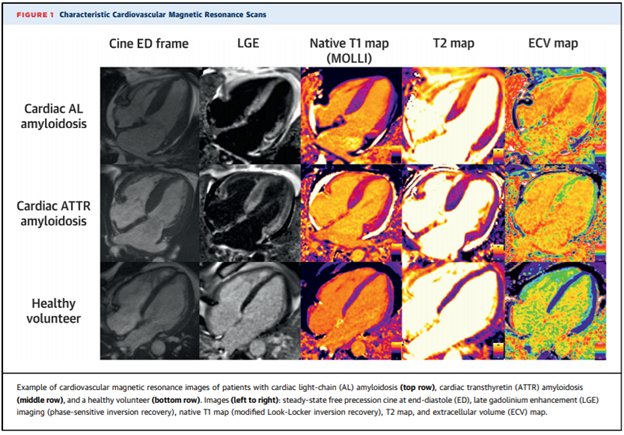
It’s all about the gad! delayed enhancement with gadolinium allows us to assess myocardial integrity. Increase in extra cellular (EC) space due to amyloid protein deposition allows the gad to accumulate & cause enhancement.

Enhancement patterns in Amyloidosis are: global endocardium, transmural, patchy. We use these known patterns in CMR to diagnose etiology of cardiomyopathy.

An example of an LGE pattern suggestive of cardiac amyloidosis. SSFP only to compare LGE findings. “Patchy mid mural” pattern.

Several studies showing the strength of sens/spec & prognosis of presence of LGE.




-ve LGE in a patient with a diagnosis of cardiac Amyloidosis confers good prognosis.

There are some differences between LGE enhancement pattern in CMR. Not enough for it to be making clinical decisions for definitive tx.

ECV=extracellular volume fraction=space between myocytes. Amyloid proteins that are produced by liver (ATTR) or abnormal plasma cells (AL) infiltrate myocardium and this causes an increase in ECV where gadolinium accumulates. Normal ECV~0.28

Middle case shows T1 imaging. Non contrast technique that is used to calculate ECV. Tends to be higher in pts with cardiac amyloidosis.

T1 & ECV values in cardiac amyloidosis & prognostic capabilities.




Data from our center showing ECV & T2/ECV capabilities in establishing prognosis.

PYP SPECT is a very important technique, as it can be used to diagnose TTR cardiac amyloidosis. Measuring counts and calculating a ratio of heart counts / contralateral count and getting a ratio of >1.5 strongly suggest ATTR cardiac Amyloidosis.

H/CL ≥1.6 confers bad prognosis. Another technique with diagnostic & prognostic capabilities.

Without biopsy you can currently assess not only the presence of cardiac amyloidosis, but differentiate between AL & ATTR by using CMR & PYP.

A patient with suspected CA undergo testing with free serum light chains and fat pad bx , & others like kidney, more accessible for mass spectrometry testing. If there is a +ve CMR in a patient with amyloidosis at other organ, is easier to establish a dx and no need for EMBx.👇🏼

Thanks for your attention. Any questions, please either DM me or post. But bottom line is that CMR & PYP are important techniques that should be part of the evaluation of patients with suspected cardiac amyloidosis. EMBx not needed most cases.

*go-to test. 😂Not to go.
@threadreaderapp unroll thread
PDF download of the slides documentcloud.adobe.com/link/track?uri…