,
24 tweets,
14 min read
Read on Twitter
Excited to have our work examining tradeoffs of alternative approaches to hematuria evaluation out in @JAMAInternalMed today. Sharing here origin story, highlights from the paper and related thoughts (THREAD)
1/n
jamanetwork.com/journals/jamai…
1/n
jamanetwork.com/journals/jamai…
Work with @pennstate2003 et al got us thinking about tradeoffs associated with differing recs in this context, in particular harms associated with radiation from CT & wide real-world dose variation (enter coauthor @UCRadSafety)
2/n
annals.org/aim/fullarticl…
2/n
annals.org/aim/fullarticl…
Concerns re low yield of CT & radiation harms ncbi.nlm.nih.gov/pmc/articles/P… motivated coauthor Ron Loo et al to study their outcomes ncbi.nlm.nih.gov/pubmed/23312369 & ultimately implement new risk-stratified KP guideline
3/n
3/n
Provocative, related (very nice) work @joshuahalpern1 jamanetwork.com/journals/jamai… & @yeciests @daviesbj ncbi.nlm.nih.gov/pubmed/29857078 sugg costs & harms>>benefit for CT in microhem. We add considerations re radiation risk + conservative assumption of subgroup w hx gross hematuria
4/n
4/n
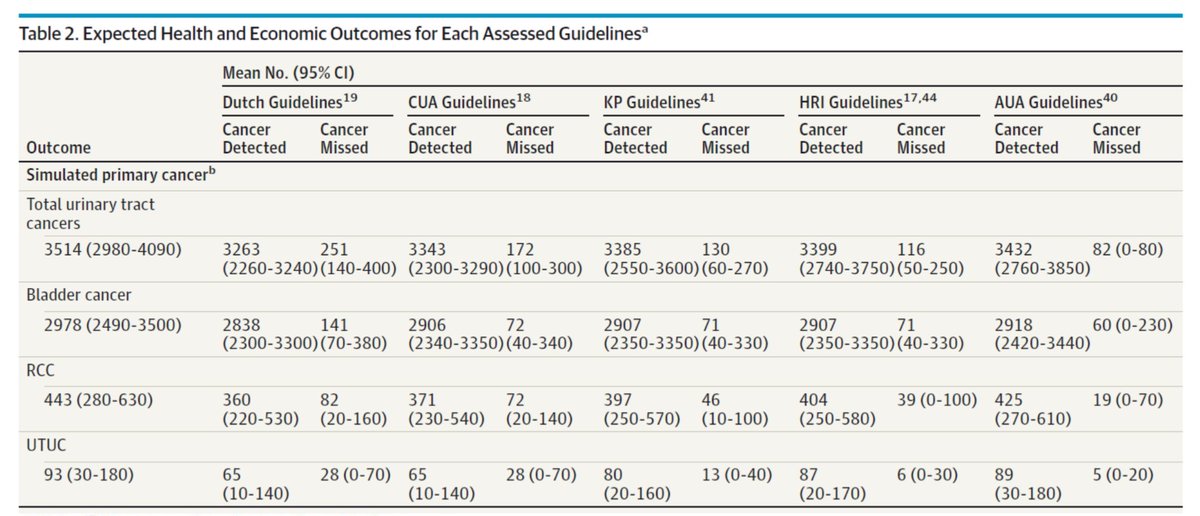
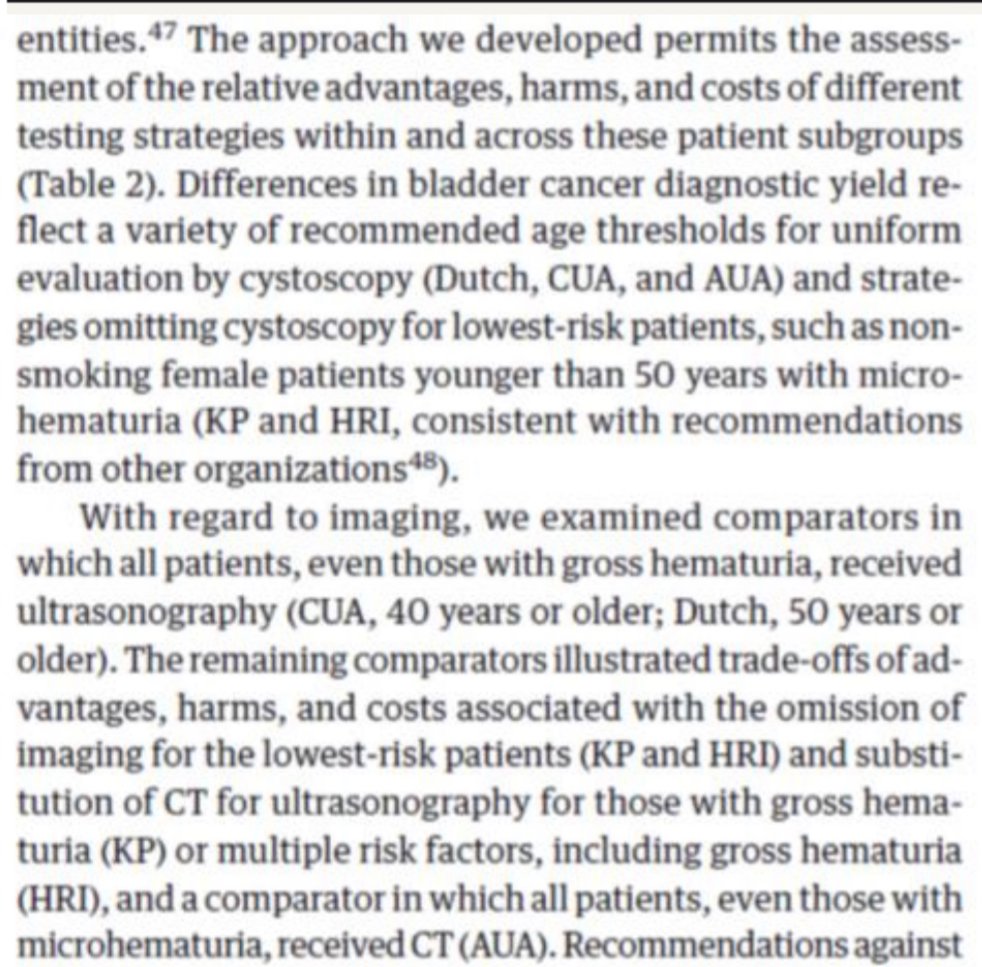
Here (Table 2) we detail incremental cancers detected by site per strategy (+ text walking through the comparators). Majority of additional cancers detected with more intensive approaches (esp those w CT) were renal cell carcinoma (RCC).
5/n
jamanetwork.com/journals/jamai…
5/n
jamanetwork.com/journals/jamai…
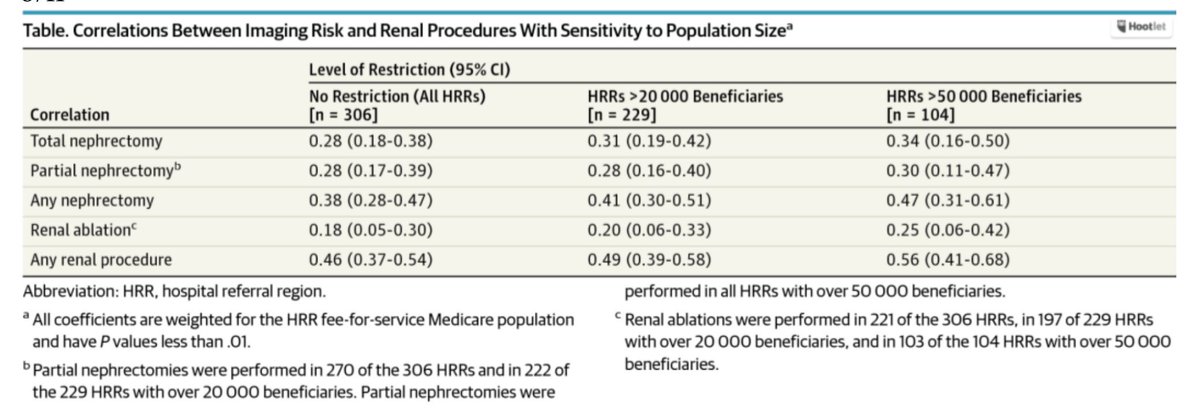
NB prevalence of RCC in our simulated popn (0.44%: drawn from the 2 largest published hematuria series), approximates rate of renal procedures/nephrectomy in recent series undergoing chest/abd CT for *all indications* [image here from: jamanetwork.com/journals/jamai…]
6/n
6/n
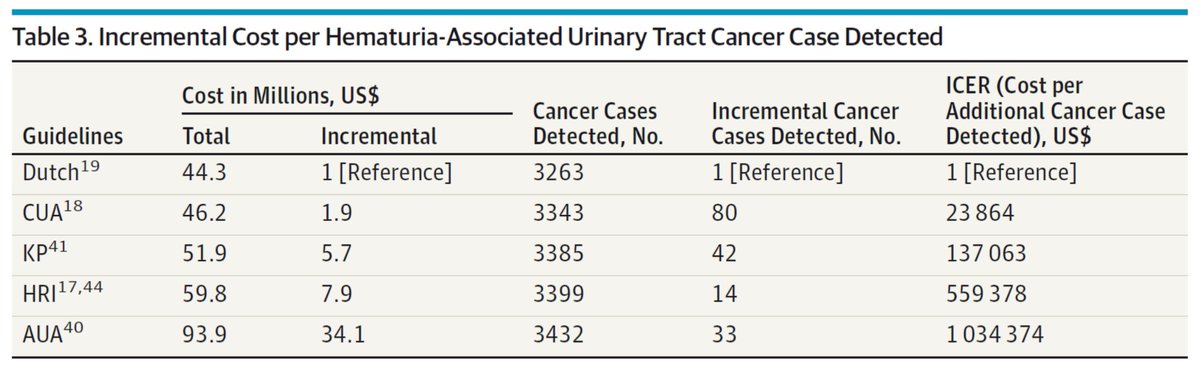
Our Table 3: incremental cost per cancer detected
& Fig 2: Cost-effectiveness acceptability curves (NB: considering GU cancers in aggregate)
7/n
jamanetwork.com/journals/jamai…
& Fig 2: Cost-effectiveness acceptability curves (NB: considering GU cancers in aggregate)
7/n
jamanetwork.com/journals/jamai…
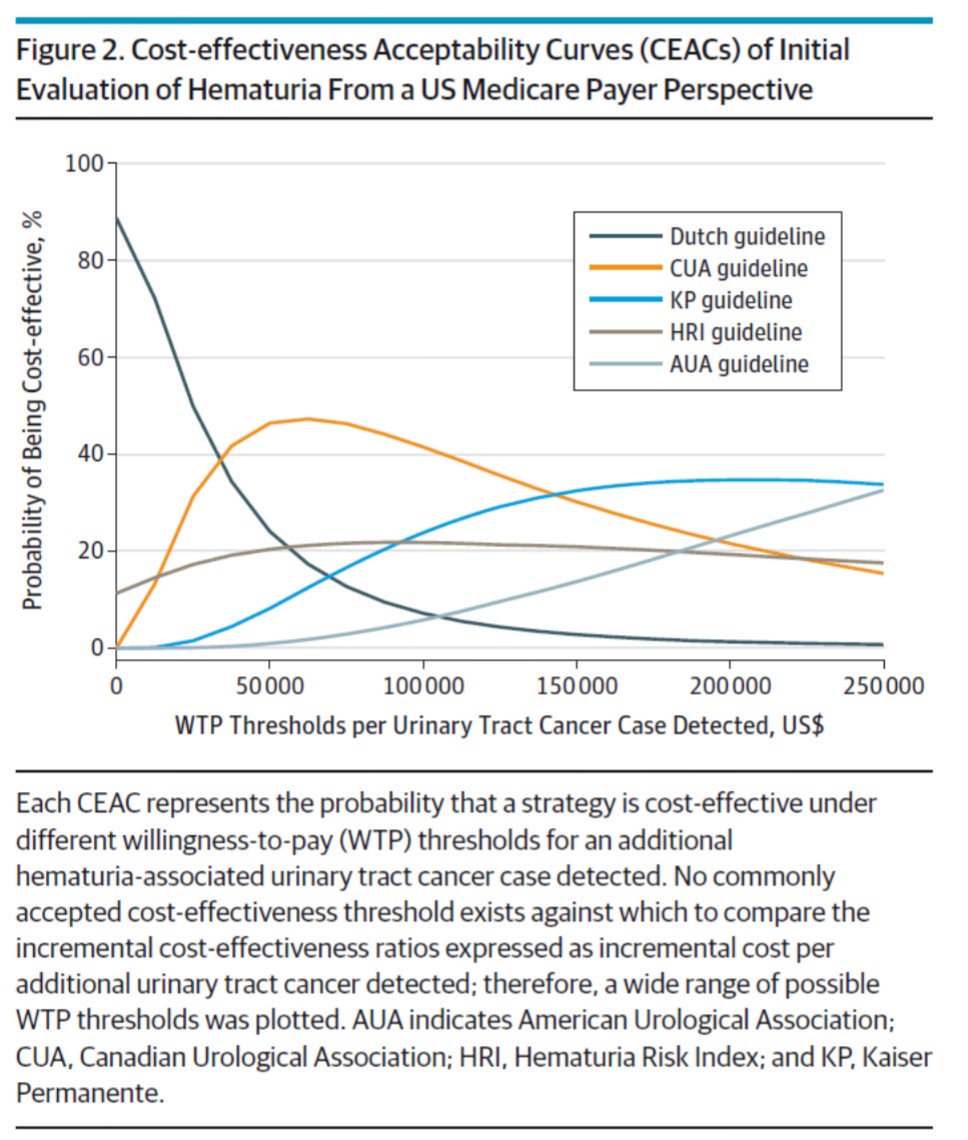
Recognizing majority incremental cases detected=RCC*, ultrasound-first approach {Canada} looks more favorable
*incidental findings?
8/n
*incidental findings?
8/n
NB We did not include incidental extraurinary findings--recent series of CT for hematuria est. additional ~$700 *per patient*, distributed from fraction w follow-up eval/invasive testing
[reflecting additional costs/harms not in our estimates]
9/n
ncbi.nlm.nih.gov/pubmed/27318261
[reflecting additional costs/harms not in our estimates]
9/n
ncbi.nlm.nih.gov/pubmed/27318261
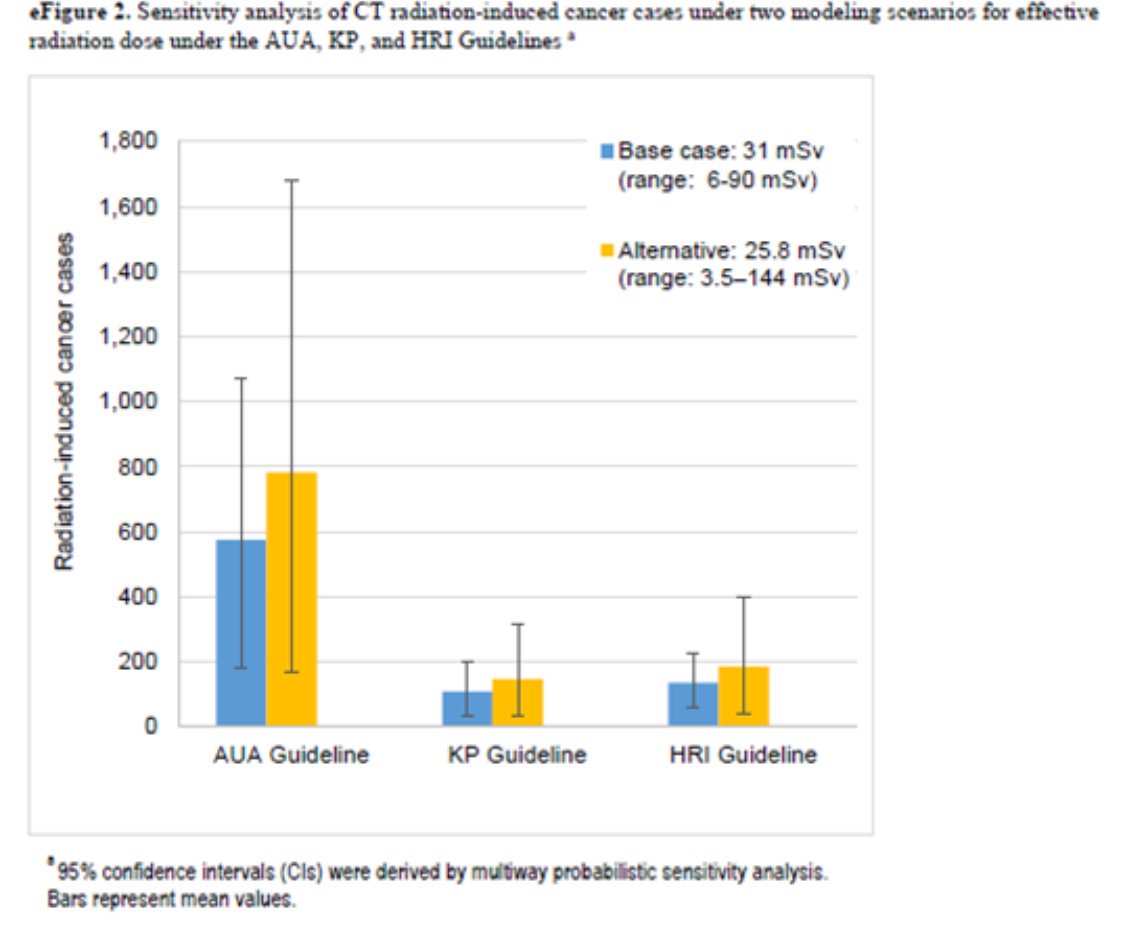
We explicitly modeled variation in CT dose from observed/real world data, which has substantial impact on the harm estimates (Fig in supplement)—underscores @UCRadSafety work to reduce dose variation: jamanetwork.com/journals/jamai…
10/n
10/n
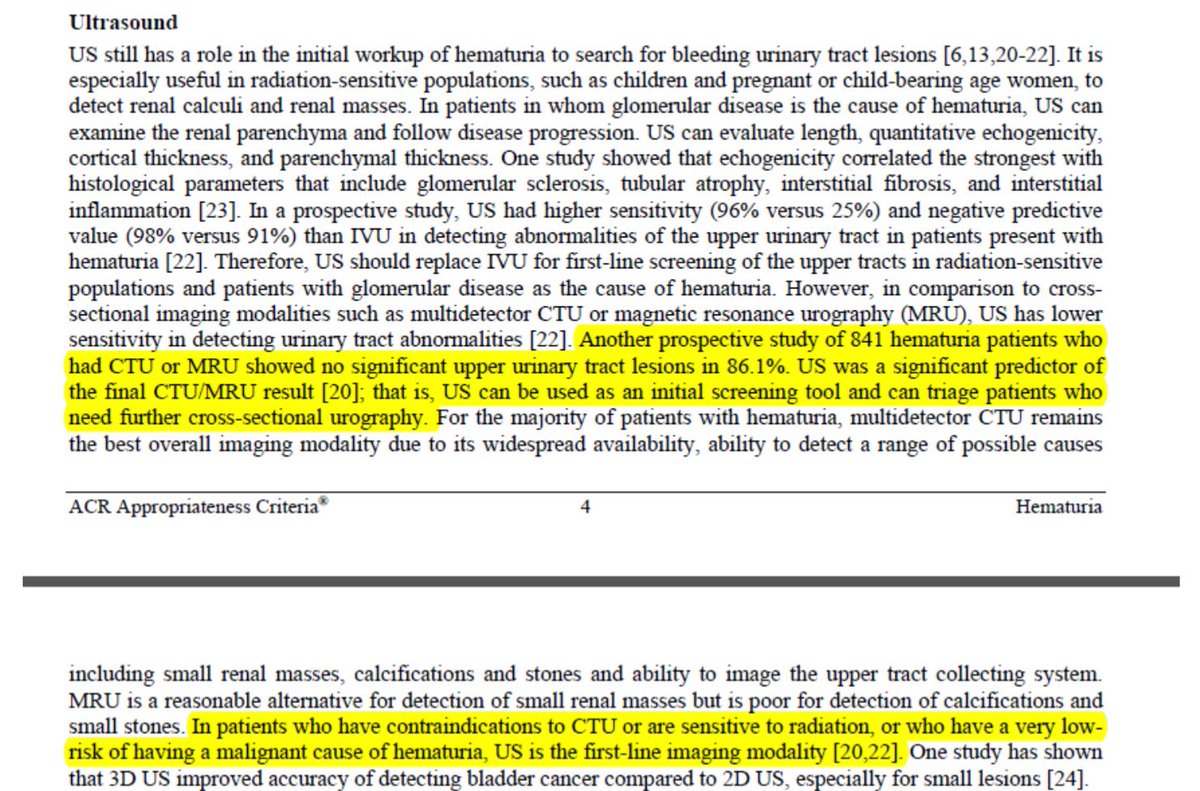
ACR Appropriateness Criteria recommends CT w contrast as top pick for hematuria eval, though discussion suggests room to consider ultrasound-first / triage approach (esp given extremely low pretest prob for overwhelming majority)
acsearch.acr.org/docs/69490/Nar…
11/n
acsearch.acr.org/docs/69490/Nar…
11/n
Several limitations noted in the paper—big picture: this should be considered a stylized comparison of different representative approaches
12/n
12/n
Quote below, attributed (h/t @DrSidMukherjee) to a pioneer of animal models of cancer, applies to the use of models as simplified representations of reality in many research contexts
en.wikipedia.org/wiki/Howard_E.…
13/n
en.wikipedia.org/wiki/Howard_E.…
13/n
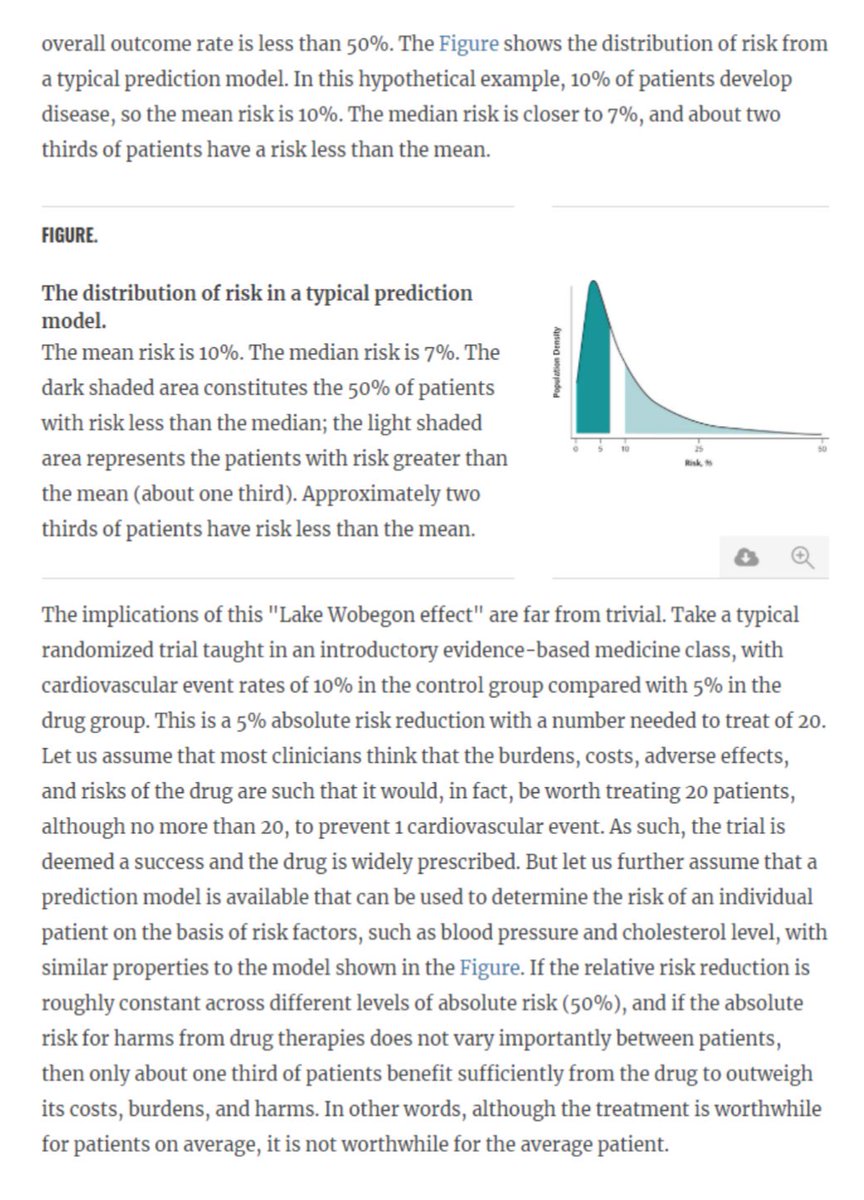
Our findings support Vickers et al assertion: most patients are at below average (mean) risk ncbi.nlm.nih.gov/pmc/articles/P…
14/n
14/n
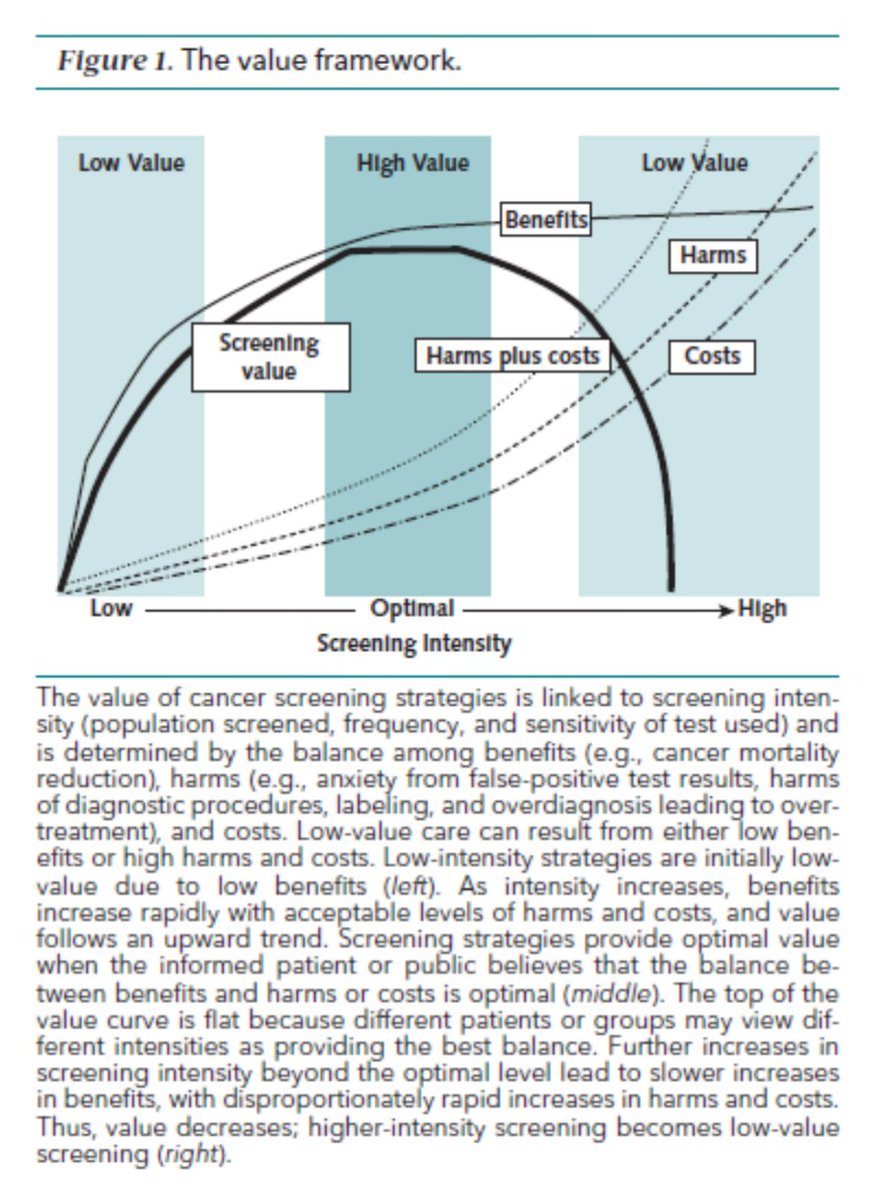
& @ACPinternists value framework for cancer screening: as intensity increases over optimal, slower increase in benefits w disproportionate increase in harms/costs
annals.org/aim/fullarticl…
15/n
annals.org/aim/fullarticl…
15/n
Good intentions (focus on sensitivity/specificity, maximizing diagnostic certainty) can lead us astray in diagnostic test evaluation
16/n
16/n
As brilliant @f2harrell blogs (channeling Bayes):
“We are interested in the probability of the unknown given the known and the probability of a future event given past and present conditions and events...”
17/n
fharrell.com/post/backwards…
“We are interested in the probability of the unknown given the known and the probability of a future event given past and present conditions and events...”
17/n
fharrell.com/post/backwards…
Risk stratification seems attractive in this context, to the extent balance of benefits/harms for a given approach varies in a predictable way across groups of similar individuals
18/n
annals.org/aim/article-ab…
18/n
annals.org/aim/article-ab…
More nice work from @yeciests @daviesbj et al (too recent to be ref’d in our paper) highlights opportunities to further stratify even the relatively higher risk subgroup with gross hematuria
19/n
ncbi.nlm.nih.gov/pubmed/31255539
19/n
ncbi.nlm.nih.gov/pubmed/31255539
Elephant in the room: improving value of care for hematuria needs to address misallocation of testing resources. (See also brilliant @LisaRosenbaum17):
20/n
nejm.org/doi/full/10.10…
20/n
nejm.org/doi/full/10.10…
Future: eval impact of KP guideline implementation—needed real-world effectiveness research in this context, also opportunity to study a specific example of unlearning and substitution, described by @helfrich_c &co #ImpSci
21/n
ncbi.nlm.nih.gov/pmc/articles/P…
21/n
ncbi.nlm.nih.gov/pmc/articles/P…
Huge thanks to terrific coauthors’ TNTC contributions to this work. @mivlage, @StephWheelerUNC, @DanErimMDPhD, @UCRadSafety, Ron Loo, @caseyng1, @Tullika_Garg, @Matt_Raynor_uro
22/n
22/n
Thanks also to the reviewers and journal editorial staff for extensive constructive feedback that improved this & to @scottryanbauer @pcarroll_ & D.Grady for thoughtful commentary
23/23
jamanetwork.com/journals/jamai…
23/23
jamanetwork.com/journals/jamai…
Sorry! @DanErim_MDPhD