
,
20 tweets,
8 min read
Read on Twitter
#MedThread Day 10 (sorta). I'm sure most know this, which is why I consider this #BreadNButterMedicine. But, if you follow along, you might learn a little history as well! Today, we are going to talk about Central Venous Catheters.
2/ If you had your choice of central line sites (no contraindications), what would you choose?
3/ 1st, why would you want to place a CVC?
🔹CVP monitoring
🔹Resuscitation
🔹Emergency venous access
🔹Inability to obtain peripheral venous access
🔹Repetitive labs
🔹Need for hyperalimentation, caustic agents, or other concentrated fluids
🔹HD
🔹and MORE!
🔹CVP monitoring
🔹Resuscitation
🔹Emergency venous access
🔹Inability to obtain peripheral venous access
🔹Repetitive labs
🔹Need for hyperalimentation, caustic agents, or other concentrated fluids
🔹HD
🔹and MORE!
4/ These are problems doctors have fought for a century to remedy. How did we end up here? Well, researching this, I fell into this rabbit hole and realized that this is something that would better be addressed by @AdamRodmanMD probably as an #AdamAnswers...
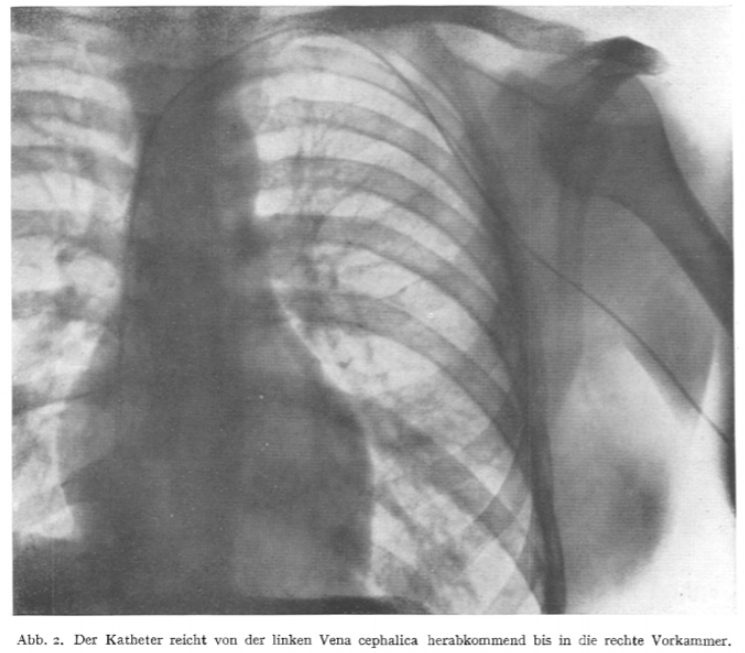
5/ Suffice to say, the history is crazy and it includes lots of horses, some dogs and crazy doctors like German surgical resident Werner Forssmann who cannulated himself with a 4-Fr ureteric catheter in 1929. 

6/ Afterwards he climbed “several” flights of stairs to then get an X-ray to confirm the catheter tip into the right atrium. This was the first documented instance of intracardiac positioning of a percutaneously placed catheter. link.springer.com/article/10.100…
7/ If you want to learn more, check out "A Short History of Central Venous Catheterization". onlinelibrary.wiley.com/doi/pdf/10.111…

8/ Forssmann’s site was the cubital fossa. This and the femoral sites were apparently the most commonly used in the early days. In the 1950s, the subclavian approach became more accepted. Of course with CVC placement, also came documented complications.
9/ The problems they saw then, are no different now…
🔹Pneumothorax (more w/ subclavian)
🔹Art puncture (more w/ femoral)
🔹Malposition
🔹Hematoma
🔹Hemothorax
🔹Infection (historically more w/ femoral)
🔹Thrombosis
🔹Arrhythmia (from guidewire)
🔹Venous air embolism
🔹Bleeding
🔹Pneumothorax (more w/ subclavian)
🔹Art puncture (more w/ femoral)
🔹Malposition
🔹Hematoma
🔹Hemothorax
🔹Infection (historically more w/ femoral)
🔹Thrombosis
🔹Arrhythmia (from guidewire)
🔹Venous air embolism
🔹Bleeding
10/ What data do we have now make our decisions on the best site? Is there one site, whether subclavian or femoral or internal jugular that clearly has less complications?
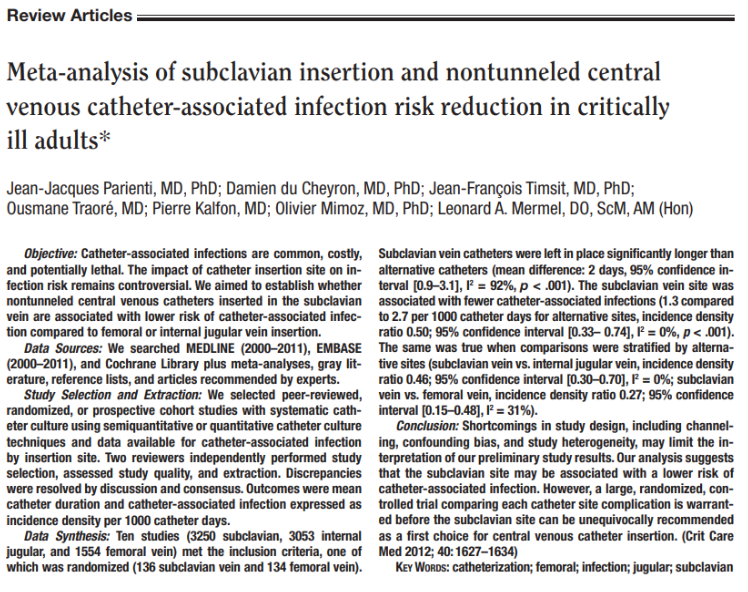
11/ Despite issues of confounding bias & study heterogeneity, a 2012 meta-analysis suggested that subclavian (SC) placement was associated w/ lower risks of catheter-associated infections. They concluded that a large RCT was needed for further evaluation. ncbi.nlm.nih.gov/pubmed/22511140
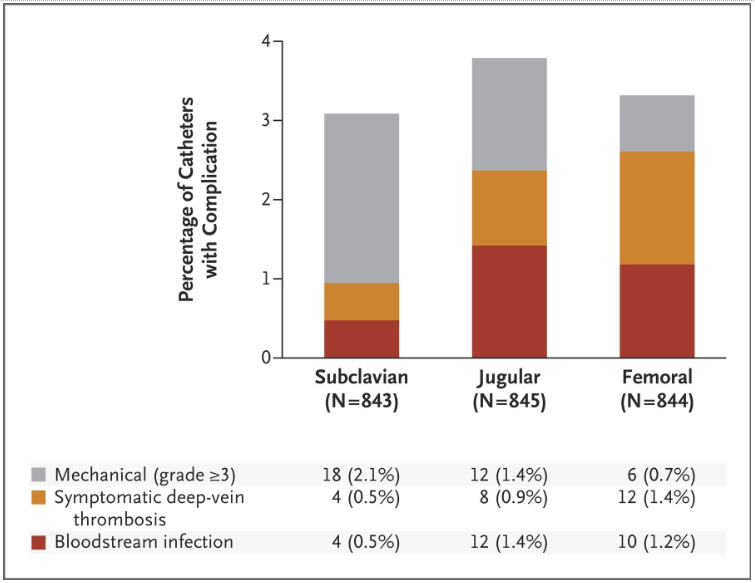
12/ The 3SITES Trial (2015) was this multicenter RCT
What did it find?
🔹SC was associated with fewer bloodstream infections
🔹SC associated with fewer DVTs
🔹SC had the highest rate for mechanical complications
ncbi.nlm.nih.gov/pubmed/26398070
What did it find?
🔹SC was associated with fewer bloodstream infections
🔹SC associated with fewer DVTs
🔹SC had the highest rate for mechanical complications
ncbi.nlm.nih.gov/pubmed/26398070

14/ Interesting result of the 3SITES trial aside from the comparisons was the fairly low percentage of complications OVERALL & the fairly low infection rates of the femoral lines.
Historically, it had been taught that fem lines should be avoided b/c high risk for infection.
Historically, it had been taught that fem lines should be avoided b/c high risk for infection.
15/ What are some criticisms of the study?
🔹Mechanical complications were only a secondary outcome
🔹Ultrasound guidance was not randomized
🔹High rate of failure and crossover in the SC arm (14.7%)
🔹Selection Bias (not 1:1:1 randomization)-> High risk excluded from SC sites?
🔹Mechanical complications were only a secondary outcome
🔹Ultrasound guidance was not randomized
🔹High rate of failure and crossover in the SC arm (14.7%)
🔹Selection Bias (not 1:1:1 randomization)-> High risk excluded from SC sites?
16/ @srrezaie's take-away from this study:
"A skilled or ultrasound guided subclavian is an ideal option but should be avoided if the operator is uncomfortable w/ the procedure.
"A skilled or ultrasound guided subclavian is an ideal option but should be avoided if the operator is uncomfortable w/ the procedure.
17/ Based on the low rates of complications (including infectious complications) a femoral line is an excellent option when clinically indicated."
Check out his discussion on the REBEL Cast: rebelem.com/november-2015-…
Check out his discussion on the REBEL Cast: rebelem.com/november-2015-…
18/ Summary:
💡SC may have lowest infection rates
💡Hard to tell if⬇️infection rates are offset by the⬆️complication rates
💡Fairly⬇️rates of complications in all sites
💡Infections for femoral⬇️than expected
💡CVCs should be placed based on operator comfort (best with US)
💡SC may have lowest infection rates
💡Hard to tell if⬇️infection rates are offset by the⬆️complication rates
💡Fairly⬇️rates of complications in all sites
💡Infections for femoral⬇️than expected
💡CVCs should be placed based on operator comfort (best with US)
FIN/ If you are only now catching my "14 days" of #Tweetorials, you can start from the beginning here:
Damn... Misspelled that tag. @WikEM_org









