
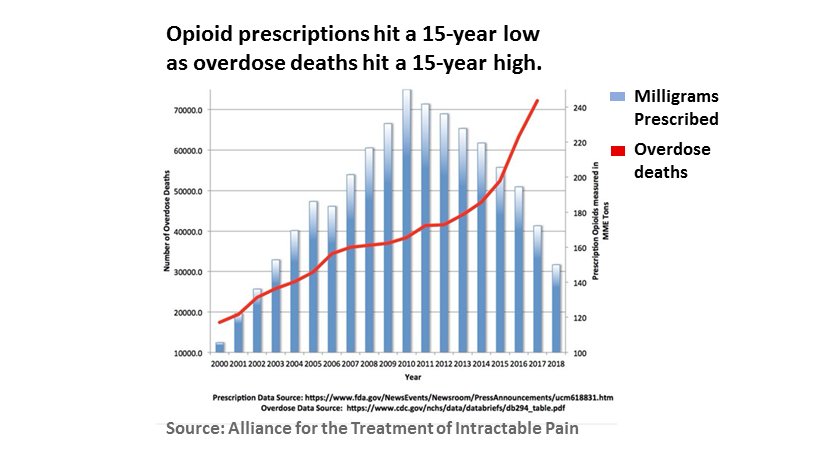
🟠 How can guidelines be "expert" recommendations if researchers haven't carefully investigated how patients will react when their rx #opiod med is stopped or reduced?
Are we going to feel better or worse? Are we going to live or die?
Are we going to feel better or worse? Are we going to live or die?


#Gratitude: @josephwfrank My colleague Dr @NitaGhei & I direct @headsUPmigraine. Thanks to you & your 2017 team for your review. It's fuel for our advocacy.
VA-funded researchers tracked what happened to the #vets whose rx #opioid was stopped in FY 2013. They found 2,887 #veterans dead from overdose or suicide.
1 year of discontinuation at the VA produced just 90 fewer bodies than terrorists did on 9/11. bmj.com/content/368/bm…
1 year of discontinuation at the VA produced just 90 fewer bodies than terrorists did on 9/11. bmj.com/content/368/bm…
Discontinuing & reducing #opioids increases the risk of #suicide by as much as 6.8 times (see Oliva above). But failing to prescribe effective #opioid pain med can put people in pain at high risk, too. researchgate.net/profile/Richar…
#Pain, #suicide, #opioid discontinuation
#PrimaryCare #PCP #neurology #MedicalTwitter
suicideinfo.ca/wp-content/upl…
#PrimaryCare #PCP #neurology #MedicalTwitter
suicideinfo.ca/wp-content/upl…
24.85% w/ acute pain (AP) & 34.9% w/ #ChronicPain (CP) reported a history of wanting to die.
5.83% of people w/ AP & 9.38% w/ CP reported frequent active #suicidal ideation, nearly 2x - 3x the risk of people w/o pain.
academic.oup.com/painmedicine/a…
5.83% of people w/ AP & 9.38% w/ CP reported frequent active #suicidal ideation, nearly 2x - 3x the risk of people w/o pain.
academic.oup.com/painmedicine/a…
7.06% w/ acute #pain & 7.92% w/ #chronicpain reported having a #suicide plan (4.3 to 4.8 x risk in people w/o pain).
14.11% w/ AP & 20.53% (CP)--1/5th--had attempted suicide (2.2 to 3.25 x risk of people w/o pain).
Depression & insomnia increase this risk dramatically.
14.11% w/ AP & 20.53% (CP)--1/5th--had attempted suicide (2.2 to 3.25 x risk of people w/o pain).
Depression & insomnia increase this risk dramatically.
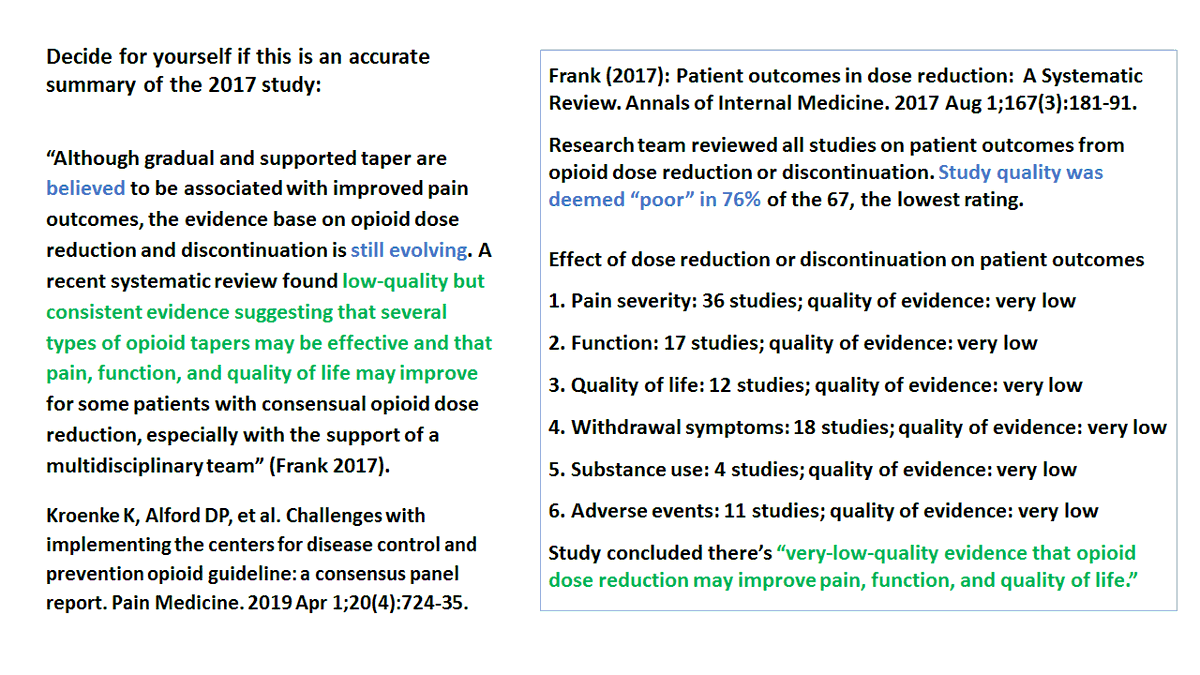
🚩 UPDATE. A 2019 paper discusses the findings of a panel that met to discuss the challenges of implementing the CDC Rx #Opioid Guideline. Here's how the 2017 Review ("very-low quality" evidence on all 6 patient outcomes) is summarized in the 2019 paper. (Hold onto your hats.)
"A recent systematic review found low-quality
but consistent evidence suggesting that several types of
#opioid tapers may be effective & that pain, function,
& QOL may improve for some patients w/
consensual opioid dose reduction, esp w/ the
support of a multidisciplinary team."
but consistent evidence suggesting that several types of
#opioid tapers may be effective & that pain, function,
& QOL may improve for some patients w/
consensual opioid dose reduction, esp w/ the
support of a multidisciplinary team."
'17: There's "very-low-quality evidence that opioid dose reduction may improve pain, function, & QOL."
'19: Altho gradual/supported "taper are believed to be associated with improved pain outcomes, the evidence base on #opioid dose reduction & discontinuation is still
evolving."
'19: Altho gradual/supported "taper are believed to be associated with improved pain outcomes, the evidence base on #opioid dose reduction & discontinuation is still
evolving."
People who BELIEVE tapers improve pain can know they're looking at "very-low-quality evidence" & see it as "evolving."
This BELIEF is the single biggest impediment to letting doctors prescribe #opioids the way they prescribe all other meds: to individuals, based on evidence.
This BELIEF is the single biggest impediment to letting doctors prescribe #opioids the way they prescribe all other meds: to individuals, based on evidence.
Kroenke K, Alford DP, et al. Challenges with implementing the centers for disease control and prevention opioid guideline: a consensus panel report. Pain Medicine. 2019 Apr 1;20(4):724-35.academic.oup.com/painmedicine/a…
@NitaGhei @headsUPmigraine If I weren't a disabled footnote junkie, I wouldn't have noticed this. How many primary-care physicians have the time to sit around matching a summary in 1 paper to the original text?
@threadreaderapp unroll
@threadreaderapp unroll

