To cap a weekend of #colchicine-induced GI upset from the press release of #ColCorona trial relative %s approaching statistical significance for #COVID19... started getting messages regarding #Maduro's announcement this evening of #Carvativir, Jose Gregorio's miraculous drops 

He plans to distribute the new wonder anti-#COVID19 treatment widely throughout #Venezuela this week. He mentioned the drug is given as drops sublingually every 4 hours...
efectococuyo.com/salud/carvativ…
efectococuyo.com/salud/carvativ…
The news on #Carvativir is likely to generate multiple creative responses from many, likely to compete with the #BernieMeme from the last few days.
If you look closely at the bottle, #Carvativir's active ingredient is #isotimol (#isothymol), at a concentration of 5mg/mL.
If you look closely at the bottle, #Carvativir's active ingredient is #isotimol (#isothymol), at a concentration of 5mg/mL.

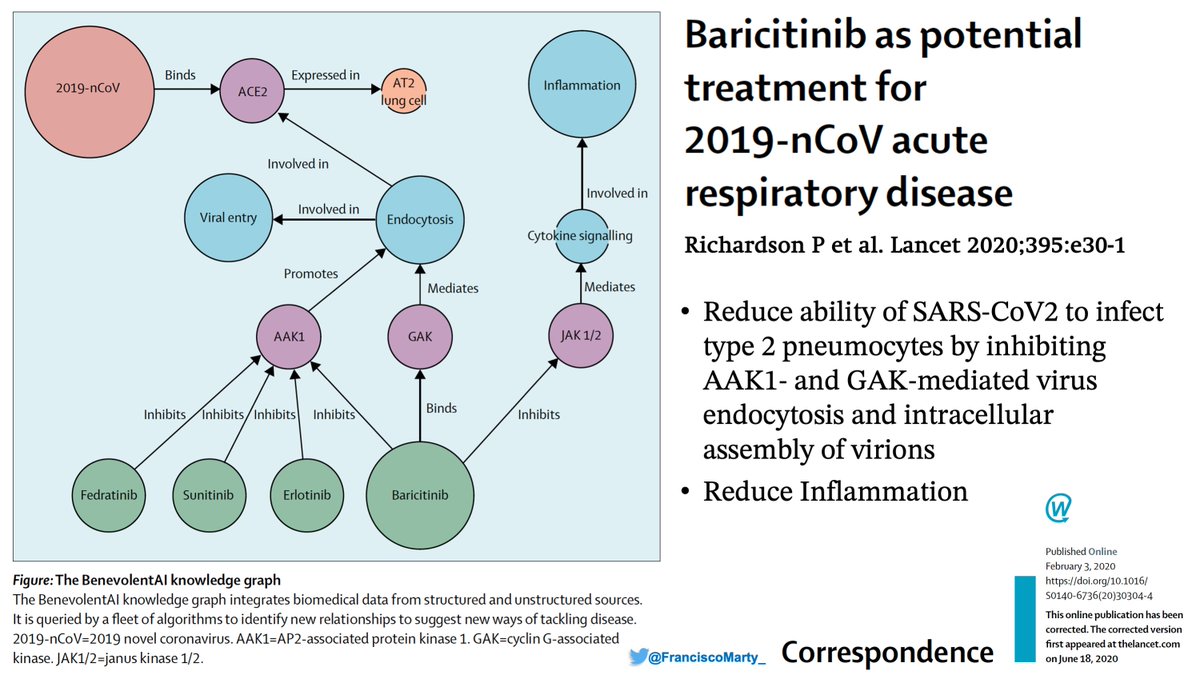
When you search for #isothymol in Pubmed, you find this link of an in-silico study postulating #isothymol may be active against #SARSCoV2 by blocking ACE2
pubmed.ncbi.nlm.nih.gov/32362217/
pubmed.ncbi.nlm.nih.gov/32362217/
Then it gets more interesting when you Google #isotimol.
You find this direct connection between #Carvativir, the proposed brand name of #isothymol for treatment of #COVID19, posted online by Laboratorio Farmacológico de Venezuela.
Link:scribd.com/document/47544…
You find this direct connection between #Carvativir, the proposed brand name of #isothymol for treatment of #COVID19, posted online by Laboratorio Farmacológico de Venezuela.
Link:scribd.com/document/47544…


The main author is Raul Ojeda from Droguería J&R, with other authors form this local Pharma company, a doctor from one of the Caracas Public Hospitals and someone from a government agency.
The 69 slides have a colleague of #SARSCoV2 biology & experiments?
scribd.com/document/47544…
The 69 slides have a colleague of #SARSCoV2 biology & experiments?
scribd.com/document/47544…
It’sclear that some people have been thinking about #isothymol.
The treatment claim for #Carvativir’s brand for #COVID19 is unsubstantiated by any clinical data, but as a #Maduro pres-release, it may hit the social media waves for another high of sublingual bread & circus.
The treatment claim for #Carvativir’s brand for #COVID19 is unsubstantiated by any clinical data, but as a #Maduro pres-release, it may hit the social media waves for another high of sublingual bread & circus.
• • •
Missing some Tweet in this thread? You can try to
force a refresh