1) Welcome to a new #accredited #tweetorial, Prevention and Management of Heart Failure in T2 Diabetes: The Diabetologist’s Perspective! Our expert author is Melanie J Davies CBE FMedSci @profmjdavies, Prof of Diabetes Medicine, U Leicester, Leicester Diabetes Unit @LDC_Tweets 

2) This program is intended for #healthcare professionals and is accredited by @academiccme for 0.75h CE/#CME credit for #physicians #physicianassistants #nurses #nursepractitioners #pharmacists 🇺🇸🇨🇦🇬🇧🇪🇺. FOLLOW US for #cardiometabolic education from expert authors!
3) @cardiomet_CE is supported by educational grants from AstraZeneca, Bayer, Boehringer Ingelheim Pharmaceuticals Inc. and Eli Lilly Company, and Chiesi. See archived programs still available for credit at cardiometabolic-ce.com. Disclosures at cardiometabolic-ce.com/disclosures/
3) In this programme we will consider evidence-based approaches to #manageHF & #preventHF in people living with #T2DM.
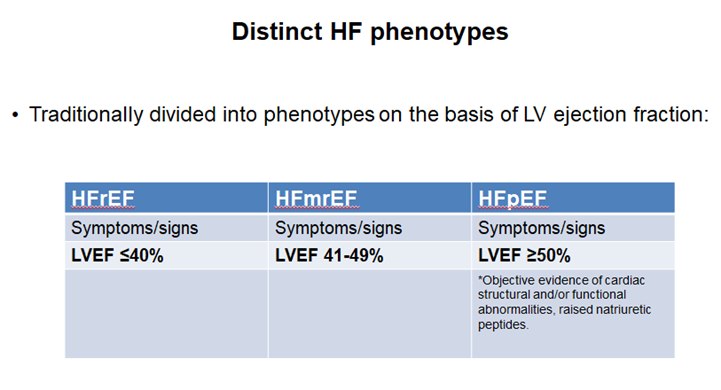
4) But let's begin with some basics, many of us are not #Hfexperts, but may be diabetes or primary care teams, so it's worth reminding ourselves of the typical #HFsigns and #HFsymptoms
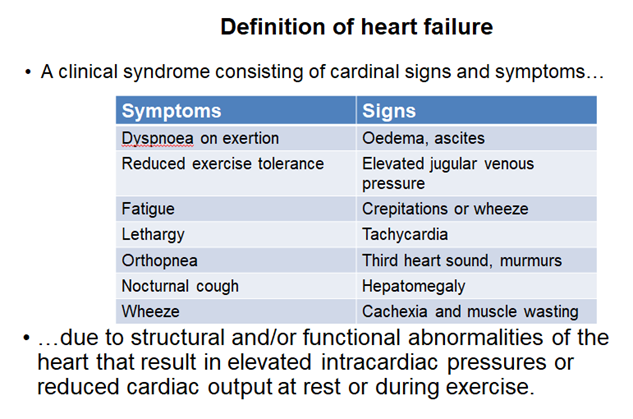
5) Also we increasingly recognise distinct #HFphenotypes based on #LVEF, for example Reduced Ejection Heart Failure #HFrEF & Preserved Ejection Heart Failure #HFpEF
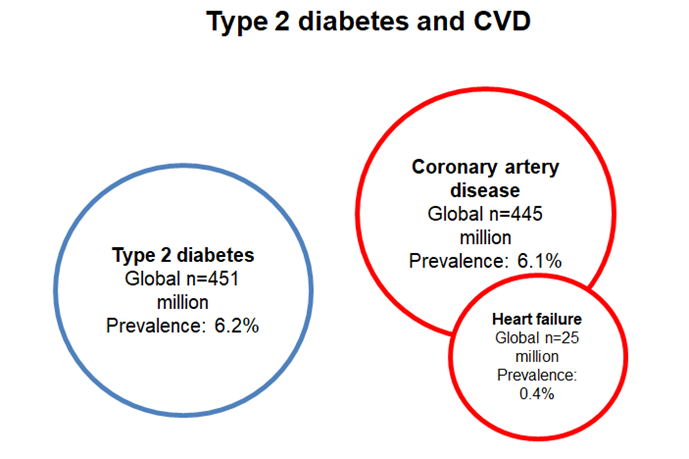
6) People with #diabetes comprise only about 5% of the entire adult population in the Western world, yet they account for 25-30% of admissions for #cardiovascular complications.
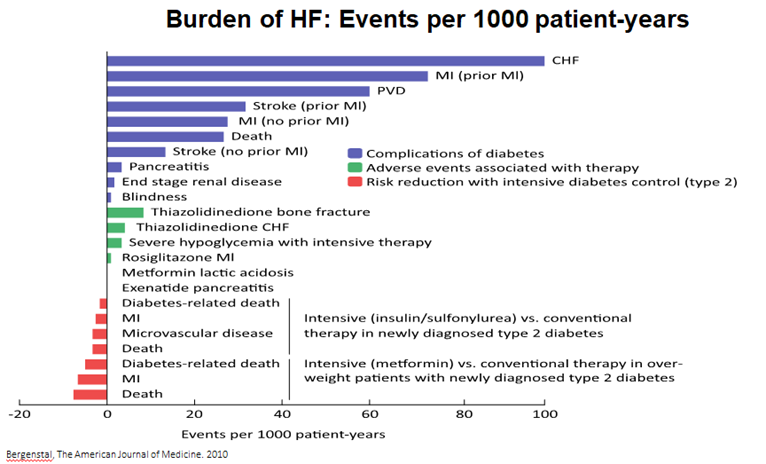
7) The high burden of #HF in #T2DM is starting to be more appreciated by #HCPs. For example, in pubmed.ncbi.nlm.nih.gov/20362759/, #HF had the highest number of events per 1000 patient years of any complication.
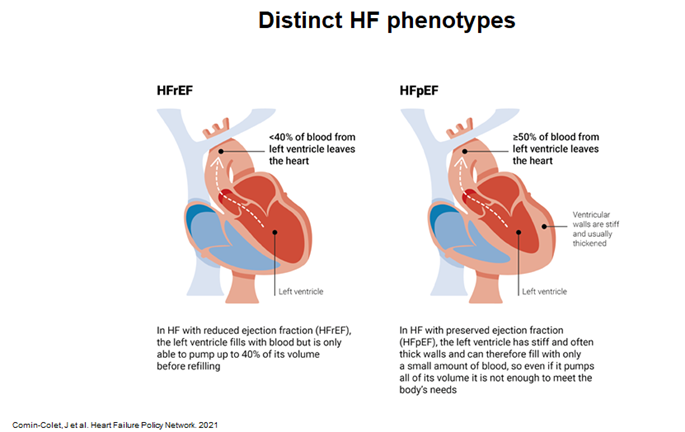
8) Although the signs and symptoms are the same, the mechanisms driving these are very different in #HFrEF and #HFpEF. See 🔓hfpolicynetwork.org/project/heart-… from @HFPolicyNetwork.
9) Furthermore, clinical outcomes for #HFrEF and #HFpEF are generally similar and are generally poor! See 🔓jacc.org/doi/abs/10.101….
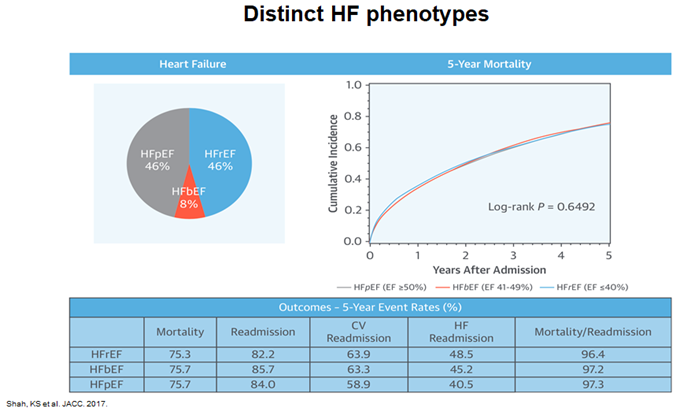
10a) In data from the “Get with The Guidelines – Heart Failure” (GWTG-HF) registry 🇺🇸 of patients presenting to hospital with acute decompensated heart failure, median survival overall was 2.1 years.
10b) In a risk-adjusted survival analysis, all subgroups had similar 5-year mortality and rehospitalization was similar for all subgroups.
11a) Mechanisms driving underlying #cardiac dysfunction are different in #HFrEF and #HFpEF. In the general population, patients with #HFpEF are more likely to be ♀️, with a higher prevalence of #hypertension and #diabetes. #Obesity is a major feature of HFpEF.
11b) By contrast, #HFrEF more commonly affects ♂️who have a history of ischaemic heart disease.
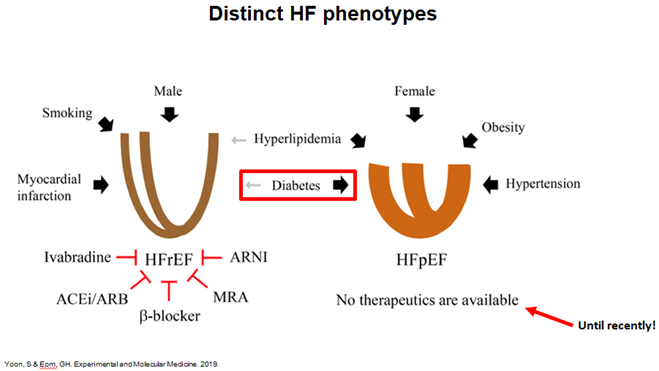
12) Moreover, remodelling patterns are different in the 2 forms of HF. The 🫀 in HFrEF is dilated, but in HFpEF is thickened & restricted. Most importantly, whilst there are many evidence-based tx's for HFrEF, until recently there have been no clear tx options for HFpEF.
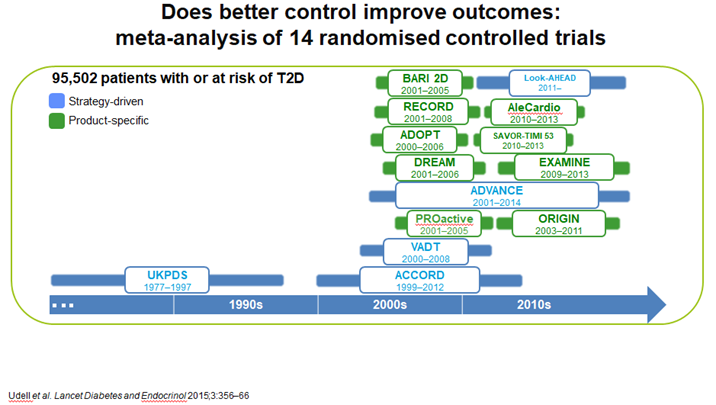
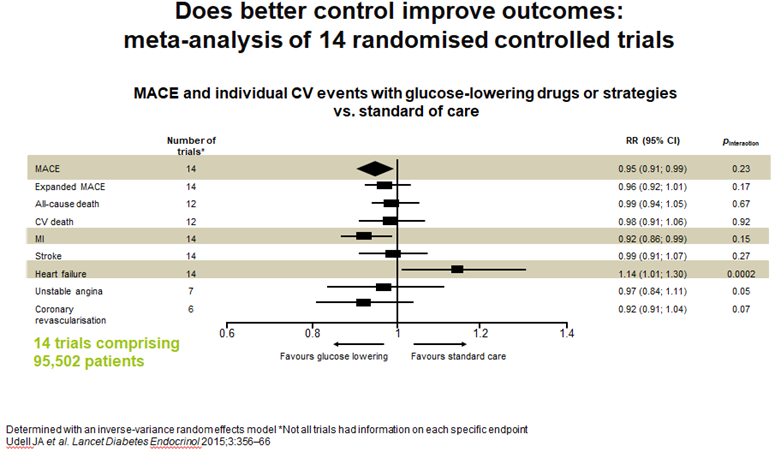
13a) See 🔓pubmed.ncbi.nlm.nih.gov/25791290/ for a meta-analysis of glucose lowering trials & impact on long-term outcomes that assessed the extent to which glucose ⬇️by various drugs/strategies affects risk of HF in pts w/ or at risk for T2D, ...
13b) ... & to establish whether #HF risk is associated with glycaemic control
14) These data showed an ⬆️in #HF, probably explained by the inclusion of studies with #TZDs and the early trials with #DPP4i, including #saxagliptin
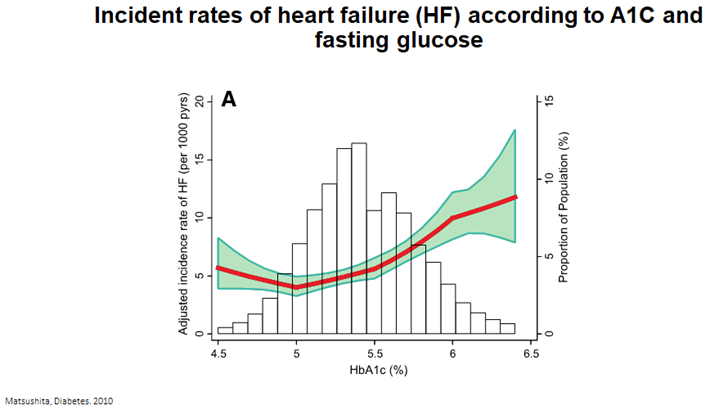
15) Furthermore, studies in those w/o #diabetes & risk of #HF, #HbA1c levels >5.5% are associated with incident heart failure, suggesting chronic hyperglycaemia prior to the development of #DM contributes to the development of #HF, highlighting the potential role of #prevention
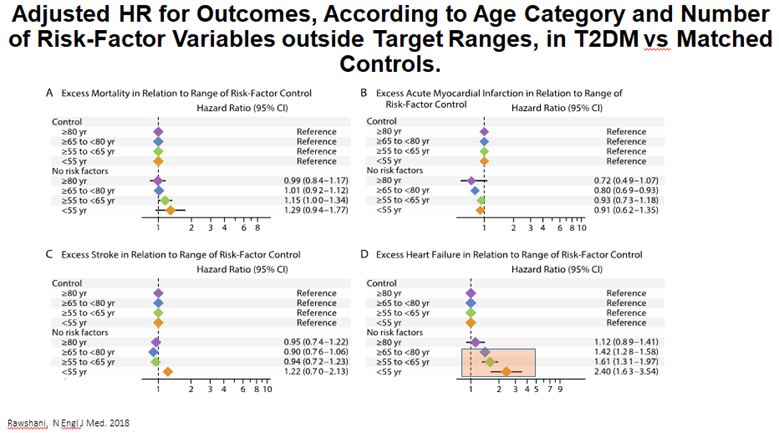
16a) The challenge of how to reduce the risk of #HF in people with #T2DM is highlighted in data from over 270,000 people with T2DM from the #Swedish National Diabetes Register 🇸🇪. Targeting 5 traditional #CV risk factors . . .
16b) . . . almost⬇️excess risk to control levels for #stroke & #MI but not #HF, partic in younger age groups. This emphasizes need for different approaches to care beyond traditional risk factor control to⬇️HF in #T2DM, esp in younger pts
17b) Mark your best answer & return TOMORROW for more education on the #prevention & #management of #HF in #T2D. EARN 🆓CE/#CME! 👍to @PNewlandJones @VickiaDSN @ClareHambling @WilmotEmma @EDEN_Leicester @drpratikc @sotonDSN @DrAndrewBaldwin @TaheriShahrad #FOAMed @kamleshkhunti
18) Welcome back! I am @profmjdavies and you are earning CE/#CME while you learn about #prevention & #management of #heartfailure in #T2D! Let's keep it going! 👏to @westernuFamMed @ProfBatterhamMD @AliRacaniere @JuleenRZierath @iDEALdiabetes @GoggleDocs @MedTweetorials #FOAMed
19) Yesterday's quiz? Scroll ⤴️to #17a if you didn't yet answer. NO PEEKING!
OK, the answer is d. patients with #HFpEF are more likely to be ♀️, with a higher prevalence of #hypertension and #diabetes. #Obesity is a major feature of HFpEF.
OK, the answer is d. patients with #HFpEF are more likely to be ♀️, with a higher prevalence of #hypertension and #diabetes. #Obesity is a major feature of HFpEF.
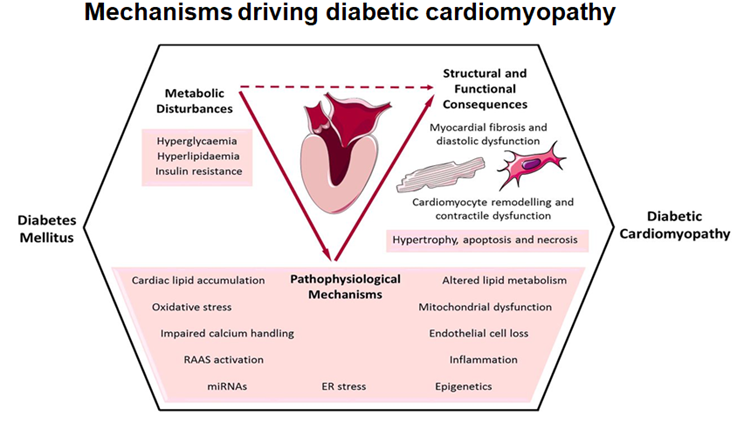
20) The mechanisms driving #HF in #T2DM are complex, multifactorial and incompletely understood, but ➡️ a particular predisposition towards #HFpEF.
21) Data from our own group (see 🔓pubmed.ncbi.nlm.nih.gov/24606573/ & 🔓pubmed.ncbi.nlm.nih.gov/24970723/) highlights a real concern of the risk in early signs of heart failure in younger people with T2DM, beyond the risk with obesity alone
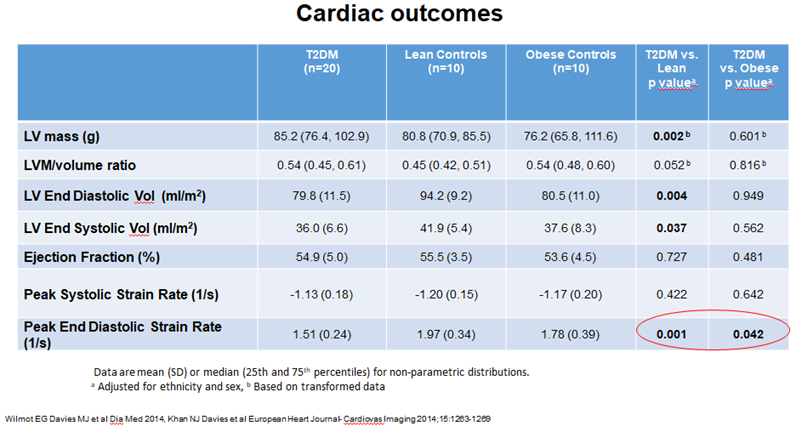
22) We showed Subclinical LV diastolic dysfunction was present in young adults with T2DM despite short disease duration & #Independent of #obesity. Indeed, #diastolic #dysfunction is the earliest manifestation of Diabetic #Cardiomyopathy (🔓pubmed.ncbi.nlm.nih.gov/24970723/)
23a) Diastolic dysfunction results in impaired #QoL, reduced #exercise tolerance, #heartfailure (37% risk over 5 years). May get benefit from weight loss (diet or bariatric surgery), better glycaemic control, CV risk factor management including ACE inhibitors and statin therapy.
23b) That's the message from 🔓ncbi.nlm.nih.gov/pmc/articles/P…, 🔓pubmed.ncbi.nlm.nih.gov/17925474/, & 🔓pubmed.ncbi.nlm.nih.gov/18158708/). Diastolic dysfunction is an indication for early and aggressive management including potential for weight management in this younger and high risk group
24a) Moving to what we know regarding #HF outcomes for the trials of various #GLT (glucose lowering therapies) in #T2DM, we can categorise agents that increase risk of #HF – the #TZD & some of the #DPP4i’s (saxliptin).
24b) Other #DPP4i, #basal #insulin, and α-GI are neutral but and @GLP1 RAs have modest benefit from meta-analysis. #SGLT2i show consistent and robust benefits. Consider 🔓nejm.org/doi/full/10.10…, 🔓pubmed.ncbi.nlm.nih.gov/30418475/, 🔓pubmed.ncbi.nlm.nih.gov/28605608/, 🔓pubmed.ncbi.nlm.nih.gov/30415602/. . .
24c) 🔓pubmed.ncbi.nlm.nih.gov/28910237/, 🔓pubmed.ncbi.nlm.nih.gov/26630143/, 🔓pubmed.ncbi.nlm.nih.gov/27633186/, pubmed.ncbi.nlm.nih.gov/30291013/, 🔓nejm.org/doi/full/10.10…, pubmed.ncbi.nlm.nih.gov/28917545/, 🔓pubmed.ncbi.nlm.nih.gov/26052984/, pubmed.ncbi.nlm.nih.gov/25765696/, 🔓pubmed.ncbi.nlm.nih.gov/23992601/ . . .
24d) 🔓pubmed.ncbi.nlm.nih.gov/17666462/, & pubmed.ncbi.nlm.nih.gov/19501900/, 🔓pubmed.ncbi.nlm.nih.gov/27295427/. So, you're welcome--there's your #HF--#T2D clinical trial library!


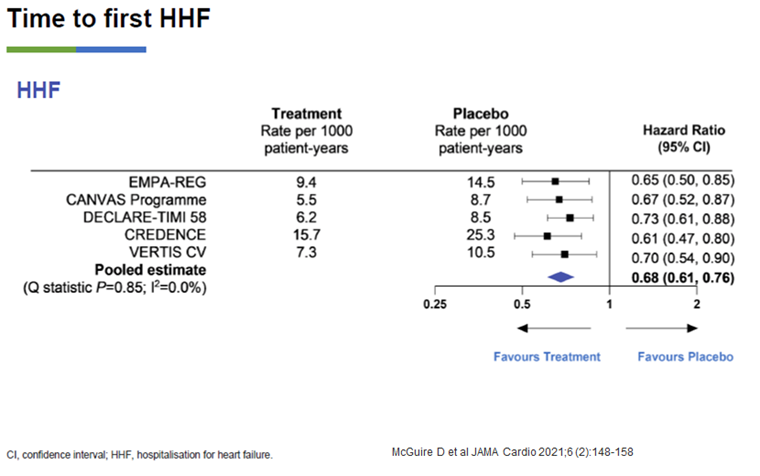
25) Data from the large #CVOTs in #T2DM with the #SGLT2i class has shown robust & remarkably consistent benefit in reducing hospitalisation for Heart Failure #HHF, a pre-specified secondary outcome in many of these trials
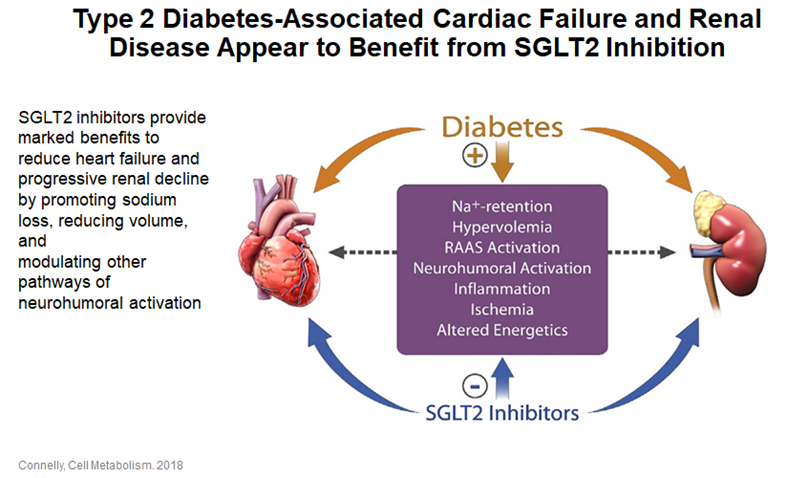
26) There are a number of postulated mechanisms which explain the beneficial effects of #SGLT2i on #heartfailure outcomes & also explain their benefit in #CKD
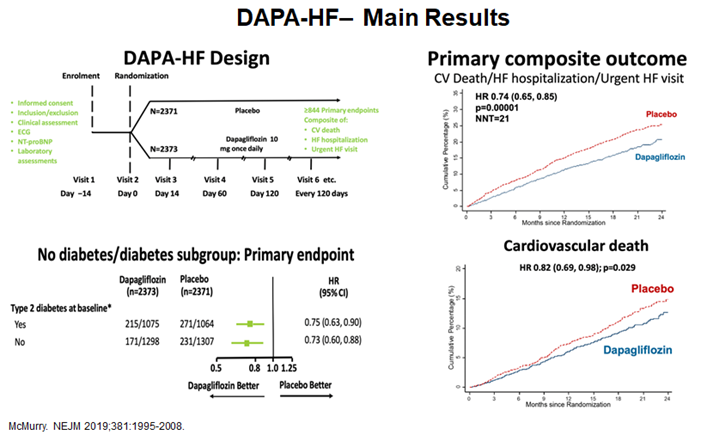
27a) The first trial to examine #HF as a primary outcome in people w/ & w/o #T2D was the #DAPA_HF study with #Dapagliflozin (🔓pubmed.ncbi.nlm.nih.gov/31535829/). The trial met its primary endpoint of CVDeath/hHF/UrgentHF visit as well as showing ⬇️#cardiovascular death with dapagliflozin.
27b) DAPA-HF was the 1st HF outcomes trial investigating tx of adults with #HFrEF, w/ & w/o #T2D, w/ an #SGLT2i on top of standard of care (#ACE-I, #ARB, β-blockers, #MRA, #ARNI). Dapa➡️stat significant & clinically meaningful⬇️in risk of worsening heart failure events ...
27c) ... and #CV death vs placebo, ➕improvement in #HFsymptoms, when added to standard tx. The safety findings of DAPA-HF were consistent with the well-established safety profile of dapagliflozin and the rate of discontinuation was low.
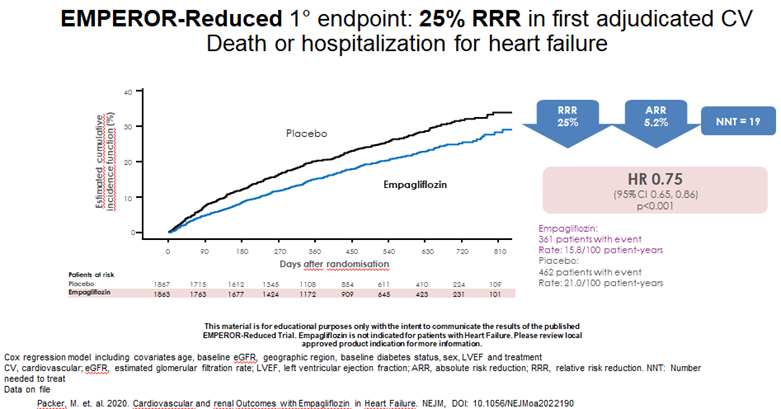
28) A subsequent #HF trial with the #SGLT2i #Empagliflozin also met its primary endpoint: 🔓nejm.org/doi/full/10.10…
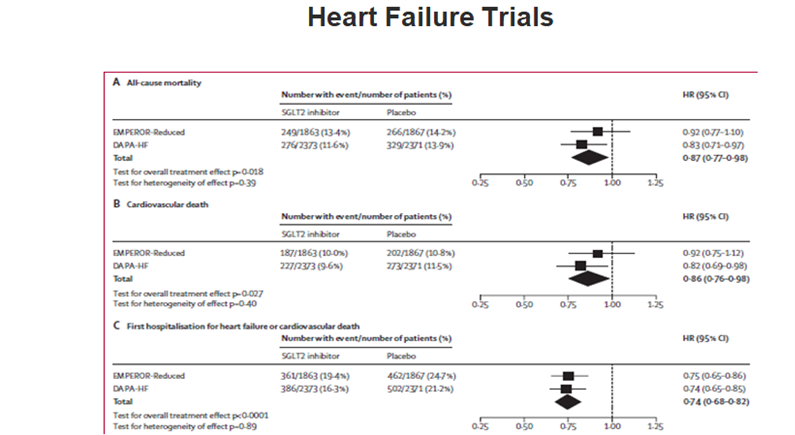
29) A meta-analysis pubmed.ncbi.nlm.nih.gov/32877652/ demonstrated the benefits of #SGLT2i on #HFrEF outcomes in these two trials, AND showed the benefits in these patients on #renal outcomes with a reduction in first kidney outcome composite HR 0.62 (CI 0.43-0.9).

30) So how about a quick knowledge ✔️? Which of the following helps explain the benefit of #SGLT2i therapy on #HF & #CKD outcomes?
31) Mark your best answer and return tomorrow for a wrap-up of this program and a link to your 🆓CE/#CME! It's that easy! Tip o' the hat to @EsePresident @brendonneuen @RpratleyMD @AliceYYCheng @cpcannon @DLBHATTMD @SantosGallegoMD @mvaduganathan @EylemLevelt @ShivaniM_KC
• • •
Missing some Tweet in this thread? You can try to
force a refresh