
1) Welcome to a new #accredited #tweetorial in our series of educational programs on #hypertrophic #cardiomyopathy #HCM. Previous programs, still available for 🆓CE/#CME, are at cardiometabolic-ce.com/category/hcm/.
Now you can earn another 0.75hr credit by following this 🧵!
Now you can earn another 0.75hr credit by following this 🧵!
2) Our expert author is JA Linderbaum MS, ARNP, FACC, FPCNA @jlinderbaum, Associate Professor of Medicine, @MayoClinic, CV #NursePractitioner, Assoc. Medical Editor #AskMayoExpert.
#FOAMed #MedEd @MedTweetorials #CardioTwitter @transformingHC @TNPJ_Journal #cardiology
#FOAMed #MedEd @MedTweetorials #CardioTwitter @transformingHC @TNPJ_Journal #cardiology

3) This program is supported by an unrestricted educational grant from Bristol Myers-Squibb. Statement of accreditation and faculty disclosures at cardiometabolic-ce.com/disclosures/. Credit for #physicians #nursepractitioners #physicianassociates #nurses #pharmacists from @academiccme.
4a) This #tweetorial will follow a Q&A format and will address multiple foundational issues about the diagnosis, staging, and management of #HCM. @jlinderbaum will provide guideline supported comments #guidelines
4b) 2020 AHA/ACC Guideline for the Diagnosis & Treatment of Patients With Hypertrophic Cardiomyopathy: A Report of the @accintouch / @American_Heart Joint Committee on Clinical Practice Guidelines, from @SteveOmmen et al:
🔓pubmed.ncbi.nlm.nih.gov/33215938/ and pubmed.ncbi.nlm.nih.gov/33926766/
🔓pubmed.ncbi.nlm.nih.gov/33215938/ and pubmed.ncbi.nlm.nih.gov/33926766/
4c) 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients With Hypertrophic Cardiomyopathy: EXECUTIVE SUMMARY: A Report of the @ACCinTouch / @American_HeartJoint Committee on Clinical Practice Guidelines, from @SteveOmmen et al:
🔓pubmed.ncbi.nlm.nih.gov/33215938/
🔓pubmed.ncbi.nlm.nih.gov/33215938/
4d) Data summary from
Hypertrophic Cardiomyopathy: New Evidence Since the 2011 American Cardiology of Cardiology Foundation and American Heart Association Guideline, from #ArianeFraiche et al:
pubmed.ncbi.nlm.nih.gov/27294414/
Hypertrophic Cardiomyopathy: New Evidence Since the 2011 American Cardiology of Cardiology Foundation and American Heart Association Guideline, from #ArianeFraiche et al:
pubmed.ncbi.nlm.nih.gov/27294414/
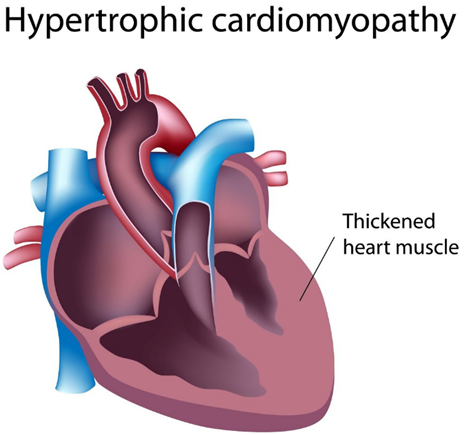
5b) Most individuals with #HCM are asymptomatic & have a normal life expectancy. Most can lead active, normal lifestyles. Individuals who present with symptoms or have a family history #FamHx of HCM may present w/ classic sx & findings which may include any of the following:
5c)
Symptoms: #presyncope, #syncope, exertional #dyspnea, activity intolerance, #palpitations, chest pain
Symptoms: #presyncope, #syncope, exertional #dyspnea, activity intolerance, #palpitations, chest pain
5d) Exam findings: individuals with HCM can have a normal physical exam, or may have a notable systolic ejection murmur () that changes intensity during maneuvers that affect contractility, preload and afterload, eg:
5e)
🫀 Squatting or passive leg raise ⬇️murmur intensity
🫀 Valsalva, squat-to-stand, or walking ⬆️murmur intensity
🫀 Murmur intensity that ⬆️after a long pause
🫀 Squatting or passive leg raise ⬇️murmur intensity
🫀 Valsalva, squat-to-stand, or walking ⬆️murmur intensity
🫀 Murmur intensity that ⬆️after a long pause
6a) ❓ What are the common ECG findings in individuals with HCM?
6b) Answer: Increased voltage with or without deep T-wave inversions in the lateral precordial leads. Some individuals with HCM, may have normal ECGs.

7a) ❓ What are important history-taking strategies for surveillance of my patients with known hypertrophic cardiomyopathy #HCM with or without known obstruction?
7b) Answer: Careful physical examination and interval assessment of symptoms remains paramount.
🫀 Symptoms may include #exertional #dyspnea, exertional #angina, exertional #syncope, or #presyncope and may vary based on loading conditions such as dehydration, heat, cold
🫀 Symptoms may include #exertional #dyspnea, exertional #angina, exertional #syncope, or #presyncope and may vary based on loading conditions such as dehydration, heat, cold
7c)
🫀 Symptoms may be variable based on loading conditions (eg, #hydration, #bloodpressure, temperature)
🫀 #Hypertrophic cardiomyopathy can be misdiagnosed as exercise-induced #asthma, especially for young pts or those in whom coronary artery disease #CAD has been excluded.
🫀 Symptoms may be variable based on loading conditions (eg, #hydration, #bloodpressure, temperature)
🫀 #Hypertrophic cardiomyopathy can be misdiagnosed as exercise-induced #asthma, especially for young pts or those in whom coronary artery disease #CAD has been excluded.
7d)
👉Importantly, #comorbid conditions can exist in addition to #HCM and may present over time (e.g. #CAD, activity intolerance with orthopedic problems)
👉Importantly, #comorbid conditions can exist in addition to #HCM and may present over time (e.g. #CAD, activity intolerance with orthopedic problems)
7e)
🫀 Functional capacity and frequency and severity of symptoms should be assessed at each visit. (e.g. ask patient to rate functional capacity 1-10 at each visit and document).
🫀 Functional capacity and frequency and severity of symptoms should be assessed at each visit. (e.g. ask patient to rate functional capacity 1-10 at each visit and document).
7f) Most individuals with #HCM are asymptomatic. Those who have symptoms may describe exertional dyspnea, angina, syncope or presyncope or palpitations.
Sx can vary from day to day based on the following conditions:
A. Hydration
B. Blood pressure
C. Humidity
D. All of the above
Sx can vary from day to day based on the following conditions:
A. Hydration
B. Blood pressure
C. Humidity
D. All of the above
7g) It's all the above loading conditions, and others, including environmental 🌡️, can impact the frequency and severity of symptoms for individuals with hypertrophic cardiomyopathy #HCM.
8a) ❓Can hypertrophic cardiomyopathy be mis-diagnosed?
8b) Answer: Hypertrophic cardiomyopathy can be mis-diagnosed as #exercise-induced #asthma, #aortic valve #stenosis, or #anginal_equivalent particularly in patients with known or suspected #coronary_artery_disease.
9a) ❓ Which of the following represents a red flag sign or symptom that should be urgently evaluated for individuals with hypertrophic cardiomyopathy:
A. Fatigue
B. Dizziness
C. Palpitations
D. Syncope
A. Fatigue
B. Dizziness
C. Palpitations
D. Syncope
9b) Answer: #Syncope in individuals with known hypertrophic cardiomyopathy #HCM may be a marker for malignant ventricular #arrhythmia and always requires urgent evaluation. See 🔓 pubmed.ncbi.nlm.nih.gov/33215931/
10a) ❓ What are the classic physical exam findings for an individual with hypertrophic cardiomyopathy with obstruction?
10b) Answer: A #systolic_murmur that changes intensity during maneuvers that effect #contractility, #preload and #afterload:
🫀 Squatting or passive leg raises ⬇️murmur intensity
🫀 #Valsalva, squat to stand or activity such as walking or bicycling 🚲, ⬆️murmur intensity
🫀 Squatting or passive leg raises ⬇️murmur intensity
🫀 #Valsalva, squat to stand or activity such as walking or bicycling 🚲, ⬆️murmur intensity
10c)
🫀 The strain phase of #Valsalva, a long pause, or the standing phase of a squat-to-stand maneuver ⬆️ murmur intensity
🫀 The strain phase of #Valsalva, a long pause, or the standing phase of a squat-to-stand maneuver ⬆️ murmur intensity
11a) ❓ What are other symptoms that may occur in individuals with #HCM requiring urgent or emergent evaluation and/or referral?
11b) Answer: Other Red flag 🚨signs or symptoms for individuals with #HCM necessitating urgent or emergent referral include:
🫀 Class 4⃣ #angina or #dyspnea, #syncope or #presyncope or the inability to perform activity without these symptoms.
🫀 Class 4⃣ #angina or #dyspnea, #syncope or #presyncope or the inability to perform activity without these symptoms.
11c)
🫀 A systolic blood pressure #SBP < 90 mmHg accompanied by any of the above symptoms
🫀 heart rate greater than 120 beats per minute accompanied by symptoms
🧠 Any acute neurologic or cognitive change
🫀 A systolic blood pressure #SBP < 90 mmHg accompanied by any of the above symptoms
🫀 heart rate greater than 120 beats per minute accompanied by symptoms
🧠 Any acute neurologic or cognitive change
12a) ❓ What are the initial tests for an individual with a history and physical exam findings consistent with suspected #HCM?
12b) Answer: Initial tests include an #electrocardiogram (assess for #LVH) and an #echocardiogram with strain (to assess for outflow obstruction)
12c) 👉Importantly, ECG findings can be normal in up to 5% of ppl with #HCM. If low voltage pattern is noted, other considerations should be investigated (infiltrative or dilated #cardiomyopathy).
👉Cardiac MRI may be indicated when diagnosis is uncertain.
👉Cardiac MRI may be indicated when diagnosis is uncertain.
12d)
🫀 Individuals and families with #HCM should be referred to a Center of Excellence for comprehensive care, genetic counseling, family screening and an individualized surveillance plan for the individual and family.
🫀 Individuals and families with #HCM should be referred to a Center of Excellence for comprehensive care, genetic counseling, family screening and an individualized surveillance plan for the individual and family.
13a) #HCM may sometimes be a diagnosis of exclusion, particularly in younger individuals with left ventricular hypertrophy. What are other conditions that may contribute to #LVH?
13b)
#LVH can be related to other conditions including physiologic adaptation in elite athletes, #hypertension, #aortic valve #stenosis, & all of the following except?
a. amyloidosis
b. chronic kidney disease #CKD
c. mitral valve prolapse
d. glycogen storage dz, (e.g. Fabry Dz)
#LVH can be related to other conditions including physiologic adaptation in elite athletes, #hypertension, #aortic valve #stenosis, & all of the following except?
a. amyloidosis
b. chronic kidney disease #CKD
c. mitral valve prolapse
d. glycogen storage dz, (e.g. Fabry Dz)
13c) Mark you response and RETURN TOMORROW for the correct answer, MORE Q&A on #HCM, and your link to 🆓CE/#CME.
👏 @SrihariNaiduMD @SABOURETCardio @pabeda1 @4hcm @EduQuintanaCVS @MagliariRafael @neallakdawala @tikuowens @DrImranSheikh
👏 @SrihariNaiduMD @SABOURETCardio @pabeda1 @4hcm @EduQuintanaCVS @MagliariRafael @neallakdawala @tikuowens @DrImranSheikh
14) WELCOME BACK! @jlinderbaum is taking us methodically through foundational clinical knowledge of #hypertrophic #cardiomyopathy #HCM and YOU are earning 🆓CE/#CME.
✔️yesterday's quiz? The answer is C; all of the other options are in the #ddx for #HCM.
🫀 Now let's move on!
✔️yesterday's quiz? The answer is C; all of the other options are in the #ddx for #HCM.
🫀 Now let's move on!
15b) Answer: #Holter monitor may evaluate the incidence & presence of cardiac #arrhythmias that may occur both w/ or without patient-reported sx. Asymptomatic nonsustained #ventricular #tachycardia in individuals with #HCM is associated w/ ⬆️ risk of sudden cardiac death #SCD.
15c) Holter monitoring is typically recommended every 1-2 years to assess for nonsustained ventricular tachycardia #Vtach or asymptomatic #arrhythmias.
16a) ❓ When should #treadmill #stress_testing be considered for individuals with #hypertrophic #cardiomyopathy?
16b) Answer: Treadmill stress testing is used to determine #risk_stratification for sudden death, to assess #exercise capacity, & to promote active lifestyle in individuals with #HCM.
16c) Exercise testing can also be used to assess for ventricular arrhythmias or hypotension w/ exercise that may indicate ⬆️risk of #SCD, & to identify the presence of a dynamic #LV #outflow obstruction (dynamic in nature, which may be absent at rest, and audible with exercise).
17b) Answer: #Cardiac MRI with and without #gadolinium is used for #risk_stratification and can be indicative of ⬆️risk for cardiac #arrhythmias. A cardiac MRI will assess the anatomy of the #LV & may sometimes be used in individuals with suboptimal echocardiographic images.
17c) The presence of late #gadolinium enhancements (evidence of myocardial disarray) on cardiac MRI is a risk marker for cardiac #arrhythmias and sudden cardiac events.

18a) ❓What the risk markers for sudden cardiac death #SCD 🪦 in individuals with hypertrophic cardiomyopathy #HCM?
Answers:
🫀 Massive hypertrophy with a wall thickness >/= 3 cm
🫀 Family history of unexplained sudden death or #SCD due to known hypertrophic cardiomyopathy
Answers:
🫀 Massive hypertrophy with a wall thickness >/= 3 cm
🫀 Family history of unexplained sudden death or #SCD due to known hypertrophic cardiomyopathy
18b) (cont)
🫀 Unexplained syncope, (esp within the past 6mos)
🫀 Nonsustained #VTach on exercise testing or #Holter
🫀 Extensive (>15%) #gadolinium enhancement on cardiac MRI
🫀 #LV systolic dysfunction (LVEF <50%)
🫀 Presence of an #apical #aneurysm on #echo or MRI
🫀 Unexplained syncope, (esp within the past 6mos)
🫀 Nonsustained #VTach on exercise testing or #Holter
🫀 Extensive (>15%) #gadolinium enhancement on cardiac MRI
🫀 #LV systolic dysfunction (LVEF <50%)
🫀 Presence of an #apical #aneurysm on #echo or MRI
19a) ❓ What are the most important symptoms to assess at office visits for individuals with hypertrophic cardiomyopathy?

19b) Answer:
🫀 #Syncope or #presyncope, especially during exercise
🫀 #Chestpain &/or or postprandial #angina equivalent
🫁 #dyspnea with activity or after being supine
🫀 #Palpitations
🫀 Fatigue or activity intolerance
🫀 #Syncope or #presyncope, especially during exercise
🫀 #Chestpain &/or or postprandial #angina equivalent
🫁 #dyspnea with activity or after being supine
🫀 #Palpitations
🫀 Fatigue or activity intolerance
20a) ❓ What is the significance of a dynamic left ventricular outflow tract obstruction #LVOTO >50 mmHg?
20b) Answer: #Dynamic (sometimes present, variable) #LVOTO occurs in ~ 70-75% of ppl w/ #HCM. #Gradient > 30 mmHg at rest may ➡️sx.
Gradients >/= 50 mmHg at rest or w/ provocation & associated w/ sx are considered the threshold for consideration of #septal #reduction therapies.
Gradients >/= 50 mmHg at rest or w/ provocation & associated w/ sx are considered the threshold for consideration of #septal #reduction therapies.
21a) ❓What should be included in the annual clinical follow-up for persons with #HCM?
Answer:
🩺Annual clinical exam w/ review of patient education including hydration, aerobic activity, symptom assessment and avoidance of highly strenuous exercise with loading conditions.
Answer:
🩺Annual clinical exam w/ review of patient education including hydration, aerobic activity, symptom assessment and avoidance of highly strenuous exercise with loading conditions.
21b) (cont)
🫀 #Holter monitor every 1-2 years or with change in symptoms
🫀 Echocardiogram every 1-3 years or change in clinical status
🫀 #Holter monitor every 1-2 years or with change in symptoms
🫀 Echocardiogram every 1-3 years or change in clinical status
22) ❓What meds should be avoided 🚫in pts with #HCM?
Answer: #Vasodilators & #diuretics should be avoided due to the potential for exacerbation in #LV outflow obstruction. These medications are generally avoided in individuals with HCM.
Answer: #Vasodilators & #diuretics should be avoided due to the potential for exacerbation in #LV outflow obstruction. These medications are generally avoided in individuals with HCM.
23a) ❓ What are the common 💊 used for the treatment of #HCM?
Answer: The most common drug classes for the treatment of symptomatic HCM include (established) #beta_blockers and #CCBs, plus (emerging) cardiac myosin inhibitor (not yet in guidelines, see cardiometabolic-ce.com/hcm2/):
Answer: The most common drug classes for the treatment of symptomatic HCM include (established) #beta_blockers and #CCBs, plus (emerging) cardiac myosin inhibitor (not yet in guidelines, see cardiometabolic-ce.com/hcm2/):
23b) #Beta_blockers are the preferred initial therapy for symptomatic, dynamic outflow obstruction. BBs ⬇️myocardial contractility & HR response to exercise, which lowers the degree dynamic obstruction. Start at low dose & titrated to a resting HR </= 60 bpm.
23c) #Beta_blockers are usually effective with some symptom improvement in about 70% of individuals with #HCM.
23d) #CCBs ⬇️contractility & HR response to exercise ➡️ degree of obstruction.
Verapamil requires caution in case of severe resting obstruction due to potential for acute hemodynamic deterioration. CCB are usually effective in ~ 60% of individuals with outflow tract obstruction.
Verapamil requires caution in case of severe resting obstruction due to potential for acute hemodynamic deterioration. CCB are usually effective in ~ 60% of individuals with outflow tract obstruction.
23e) 1⃣ cardiac myosin inhibitor has recently been approved by @US_FDA to date: #mavacamten. Mavacamten promotes an energy-sparing and super-relaxed state that translates as a reduction in #LVOTO & improvement of cardiac filling pressures.
24) ❓What are additional lifestyle rec's for individuals with #HCM & #LVOTO?
Answer:
🌡️Avoid environmental vasodilatation (high temperatures & humidity, hot tubs, saunas)
🫀 Avoid vasodilators, including alcohol, diuretics
🥤Consistent hydration: at least 2 L water per day
Answer:
🌡️Avoid environmental vasodilatation (high temperatures & humidity, hot tubs, saunas)
🫀 Avoid vasodilators, including alcohol, diuretics
🥤Consistent hydration: at least 2 L water per day
25a) ❓When should I refer to an #HCM expert?
Answer: Patients should be referred to a HCM specialist and/or an HCM Center of Excellence at initial diagnosis and when sx persist despite medical therapy, or they are unable to tolerate medical therapy.
Answer: Patients should be referred to a HCM specialist and/or an HCM Center of Excellence at initial diagnosis and when sx persist despite medical therapy, or they are unable to tolerate medical therapy.
25b) Individualized tx options may be indicated:
🫀 Review & titrate 💊
🫀 SCD risk assessment
🫀 advanced management such as a septal myectomy or septal ablation
💊advanced med tx such as #disopyramide or #mavacamten
🧬Advanced genetic screening & family planning
🫀 Review & titrate 💊
🫀 SCD risk assessment
🫀 advanced management such as a septal myectomy or septal ablation
💊advanced med tx such as #disopyramide or #mavacamten
🧬Advanced genetic screening & family planning
26a) ❓ What are screening options for first-degree family relatives of pts w/ known #HCM?
Answer:
🧬Genetic testing and/or echocardiographic surveillance should be considered for all first-degree relatives of individuals with hypertrophic cardiomyopathy.
Answer:
🧬Genetic testing and/or echocardiographic surveillance should be considered for all first-degree relatives of individuals with hypertrophic cardiomyopathy.
26b) Genetic testing requires referral to a genetic counselor for discussion & evaluation of coverage options. Currently, the yield of genetic testing is ~ 60%, so shared decision making & careful selection of individuals for genetic testing . . .
26c) ... based on clinical and echocardiographic findings can help to identify patients more likely to have a positive genetic test.
26d) Echocardiographic surveillance is necessary when genetic testing is inconclusive/incomplete. Echo screening is rec'd annually for 1st deg relatives & competitive athletes, & every 5 years for other adults as clinically indicated based on age & physical activity status.
27) So congratulations! You just earned 0.75h 🆓CE/#CME! We have reviewed the current #guidelines for #HCM all right here on Twitter. Claim your credit NOW at cardiometabolic-ce.com/hcm4/.
I am @jlinderbaum of @MayoClinic, #CV #NursePractitioner. Please FOLLOW US for more programs!
I am @jlinderbaum of @MayoClinic, #CV #NursePractitioner. Please FOLLOW US for more programs!
• • •
Missing some Tweet in this thread? You can try to
force a refresh












