Been following @jenniferdoleac @anita_mukherjee naloxone paper w trepidation since learning about it last summer. Frustrating to watch how few constructive conversation emerged from the paper's recent broad exposure. My attempt to remedy w long #thread papers.ssrn.com/sol3/papers.cf… 
First, let me just say criticizing the paper or its authors for doing what is standard in their field (e.g. publishing online before formal peer review) is patently unfair. Whether or not those academic conventions make sense is a different, longer conversation
But please learn the facts and don't critique people for things they aren't responsible for. Goes without saying, there's definitely no room for personal attacks, including those baselessly questioning the authors' intelligence, competence and professionalism
These attacks are especially pernicious in view of the well-documented gender bias in Economics and other quantitative academic disciplines (as well as many other corners of academia and elsewhere)
Whether you support the "paper" or "oppose" it, I wish we could have a measured debate that doesn't devolve into a shouting match. Quixotic, but we need to do better
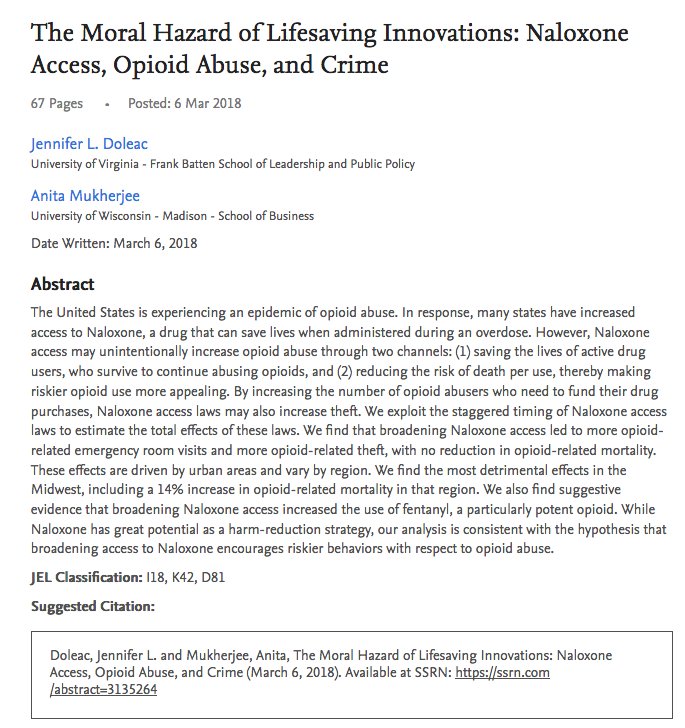
Now for thoughts about "The Moral Hazard of Lifesaving Innovations: Naloxone Access, Opioid Abuse, and Crime." Not necessarily "hot takes," as some of the below reflect points already made by others
This paper's framing and language position it to lose many readers at "hello." This "hard start" (as they say in relationship counseling) is partly why, as the authors note, their paper has received such vociferous opposiiton from "public health" community theglobeandmail.com/opinion/articl…
To be specific, the paper's analytical question, as laid out in the abstract, could be read as follows: Given that people who OD are "abusers" and criminals, is the society better or worse off when we prevent their death? (A much more abrasive paraphrase of the original, granted)
This framing is parallel to something like: "Given that Blacks w life-threatening gunshot wounds are criminal superpreditors, we better off letting them bleed out?" (NB: hyperbolic hypothetical intended to illustrate a point). See @jeremyfaust in @Slate slate.com/technology/201…
As a society, we value life very highly and spend a lot of resources saving people who have very low survival prospects. So, doubtful this line of inquiry would appear normatively appropriate w other health issues. But substance use is highly stigmatized, as this framing confirms
The choice of modeling parameters in this paper map directly onto problematic stereotypes abt who overdoses and why. This is one of the key reasons why this analysis is NOT like assessing the moral hazard of seatbelts, as some have suggested washingtonpost.com/opinions/the-m…. More below
Relatedly, moniker "abuser," though still used by some, is widely considered derogatory, about as acceptable as the term "superpreditor." The imperative to use person-first language has been covered extensively elsewhere. Here, it only reinforces the problematic analytical frame
So both question that is being asked and how it is being asked can be read as highly stigmatizing. Fighting stigma has been a difficult slog, and will continue to be 1 of the key problems impeding progress to advance policies and programs that address ODs vox.com/science-and-he…
The language and framing of the analysis is thus upsetting to a lot of ppl, especially those w lived experience and those fighting to save lives. This explains some of the visceral and sometimes vitriolic reactions the paper has received (again, NOT condoning personal attacks)
Of course, researchers are free to pursue whatever questions they desire, but framing and language matter. And there are ways of asking key questions about naloxone rescue, including the moral hazard/disinhibition question, without using stigma-laden vocabulary and assumptions.
To be clear, this analysis didn't upset so many ppl b/c it looks at and finds "evidence" of beh disinhibition. There is an entire field of public health research on this, as the authors note. It is the way this analysis frames and executes the inquiry that some find objectionable
One could stop there, as reframing and shifting its language would go a long way in addressing much of the consternation. But this analysis also suffers from major methodological problems that render its principal findings likely inaccurate, and most definitely overstated
Here, a caveat: I am an epidemiologist and not an econometrician. In my limited understanding, much of the actual quantitative strategy and analysis in this paper is solid. On the advanced math, I defer to those who are qualified to critique it (not me)
But even the most sophisticated and well-executed econometric models are subject to the "Garbage In, Garbage Out" critique. This means that quantitative analyses can be rendered highly suspect if they are built on faulty assumptions and employ biased or otherwise problematic data
First, let's examine the exposure variable for this analysis. The most fundamental, as others have noted "fatal" methodological flaw of the paper is the authors' misleading claim to measure the effect of "naloxone ACCESS." This is puzzling, b/c the analysis does NO SUCH THING
In epi research, if you set out to assess the relationship between constructs X and Y, but use a distinct proxy variable Z for variable X, you really couldn't then claim Z causes Y unless there's solid proof that construct X and proxy Z are interchangeable (among other things)
Here, analysis measures relationship between presence of naloxone access laws, crime, OD rates, and other phenomena. But in their title and write-up, they substitute "naloxone access LAW" with "naloxone ACCESS," then proceed to make causal claims about the latter
Though seemingly pedantic, using data for one construct but then calling it a another construct is highly misleading. Leaving everything else as is, this is a major, major defect that is easy enough to address simply by calling a law, a law instead of something else
Aside from the linguistic distinction, naloxone access laws are, in reality, FAR from being interchangeable w levels of naloxone access. This analysis uses 12mo window after passage of a naloxone access law to measure "treatment effect"
This makes the measurement of naloxone "exposure" vulnerable to BOTH Type I and Type II error. In other words, presence of the law may signal broadened naloxone access where there is none, or the absence of law can mask reality that there is substantial naloxone access
Having worked on legal aspects of naloxone access for over a decade including several versions of the laws in question, I can say with a high degree of confidence that the passage of these laws represent some combination of the following:
First: laws were a proxy for existing naloxone access, typically designed to clarify legal basis for ONGOING distribution. As @scottburrisphlr and I argued a decade ago, OEND is not predicated a specific law, can be supported though interim legal measures papers.ssrn.com/sol3/papers.cf…
But liability concerns, other legal barriers spurred advocates to work codify existing practice in state-level leg. (Ironically, ideological resistance to naloxone spurred advocates to work on laws, bc decisionmakers used artificial legal concerns to rationalize their opposition)
Second: in many, if not most instances, naloxone access laws were rejected for several years before passage. Oftentimes, this was based on claims about "moral hazard," despite total lack of empirical basis to support those claims
But concerns abt spiraling ODs, combined with solid data on the positive impact of naloxone put increasing pressure on legislatures/governors to endorse it. So law passage is likely CO-LINEAR w accelerating OD rates, whether in state, neighboring jurisdictions, or nationally
Third: No state naloxone access law I'm aware of designated substantial resources for naloxone distribution. As many others have pointed out, access did not typically shift as a result of the law, and certainly not within 12 mo. e.g. RI just saw nlx boost
Bottom line: critical "exposure" variable in this analysis is w/o doubt in my mind a much better proxy for ongoing (but limited) naloxone distribution efforts and legislative concern/public pressure re OD crisis than it is predictor of street-level naloxone access or deployment
Authors claim to have controlled for the possibility that the laws would have limited effect on access by engaging in "intention to treat" analysis
As an epidemiologist not an econometrician, don't see evidence that this analysis adequately addressed fundamental concerns abt Type I and Type II error, or co-linearity between exposure and outcome variables. It could be that I just don't get it, so leave it to the experts
But to reiterate, what is totally clear is that this analysis must redact all claims to be analyzing "naloxone access," when in fact they are analyzing state exposure to "naloxone access laws." I hope this fundamental distinction is beyond debate
Last thing about the exposure variable: actual laws are heterogeneous, incl both access and liability protections. So if the analysis is going to proceed w measuring law impact, a much more nuanced classification of parameters in these interventions should be considered
If the analysis instead focuses on actual naloxone access, there are, in fact sources for data on naloxone distribution. None of the sources are perfect, and certainly none as clean as the binary presence/absence of access the analysis is currently using
But complexity should not deter efforts to arrive at a better estimation of the construct the analysis currently purports to test
My take is that the above is enough to warrant a substantial re-examination, but a few more words about modeling assumptions made in this analysis. (The word "assumption" has its colloquial meaning, and it is also a term of art in econometrics)
IMHO, a number of untested assumptions about substance use, including those rooted in stigma about people who OD became translated in this analysis into quantitative "leaps of faith" that raised serious concerns about its subsequent causal inference
Sophisticated quantitative methods are employed in epidemiology, but conventions dictate that analytical assumptions be grounded in empirical evidence, either quantitative or qualitative. As far as I am aware, this is also true of econometrics
Yet here is an illustrative, not exhaustive list of assumptions used in this model that are, as far as I know, divorced from real-world evidence:
Assumption: rise in fentanyl can be driven by demand of users for stronger drugs. Reality: rise in fentanyl is not user-driven to any substantial degree. It resulted from many factors, but users exercise far too little information and choice in this market to shape it in this way
This is building on the reality that users, by and large, do not express preference for fentanyl, whether after OD or otherwise. There are perhaps occasional exceptions to this, but the modal user response is one of fentanyl avoidance, as @DanCiccarone and others have shown
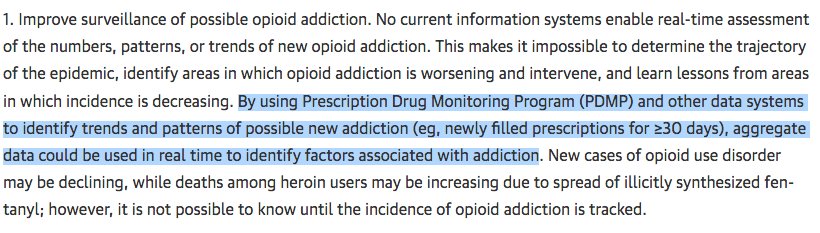
Assumption: People looking for drug treatment do so by searching internet for term "rehab." Reality: never been documented or validated as a reliable measure of help-seeking. Highly problematic for that purpose (eg questionable whether "rehab," "treatment" are interchangeable)
Assumption: levels of crime are reflected in police activity. Reality: this is a notoriously inaccurate metric of crime dynamics, see @JohnFPfaff and others
Perhaps most critical assumption: opioid users engage in behaviors reflecting moral hazard. Reality: no evidence, and certainly not on a pop scale. In fact half a dozen studies sought and did not find any empirical evidence to support risk compensation/disinhibition from naloxone
Now, this doesn't mean that we shouldn't study the issue of moral hazard further, incl re naloxone. After all, other areas of risk compensation/disinhibition/moral hazard research, including those focused on Gardasil, PreP for HIV, and male circumcision boast reams of evidence
Much of that lit refutes the risk compensation hypothesis, as humans are complex, rarely respond in ways that are predicted by classical economic theory. To be clear, some evidence in the PreP-sexual behavior realm suggests that disinhibition does occur in limited circumstances
But in epidemiology, modeling of this or any other behavior change requires an empirically-grounded estimate of effect. In other words, you have to study and quantify behavior change so that you can then extrapolate those observations using complex modeling techniques
In this case, empirical researchers did not find evidence of risk compensation. This is presumably why, to support its assumptions of naloxone-related risk compensation, this analysis relies on an urban myth amplified by policymakers presumably opposed to naloxone distribution
In the public health/epi world, a sophisticated model that anchors its core assumption on 0 empirical evidence and then uses its findings to make causal claims contravening the empirical evidence base would have dubious viability
In the public health/epi world, such an analysis would at the very least come with a lengthy limitation section to examine flaws in its inputs, outputs, and implications. This analysis does no such thing (although some limitations are outlined in the footnotes, as by convention)
Also for all of the statements directed at public health folks, it is unclear if the authors ever consulted with any public health researchers or practitioners in getting feedback to the analysis. Perhaps I missed some in the acknowledgements
And this is despite the fact that the paper has already gone through several rounds of informal peer review among visible econometric experts. So it is not clear how journal reviewers will respond to this article when it is finally submitted for formal publication
Finally, implications. This is just 1 analysis showing results that contravene all others. But in policymaking world, studies (however flawed) supporting certain ideological viewpoints get lifted up, while those that contravene that viewpoint are never robust, or numerous enough
The impact of this analysis is not predicated on publication in a peer reviewed journal. For all of its flaws, the analysis has already likely dealt a substantial setback to advocates for harm reduction
Policies restricting and rolling back naloxone access are already emerging, including in some of the hardest-hit areas of US, at the same time as calls to double down on failed punitive approaches are gathering steam usatoday.com/story/news/nat…
In its current form, this analysis will likely further fuel those restrictions. Whether intended or not, its impact will be measured in lost lives that could have been saved by naloxone
But there is room for common ground. The driving point of the paper is pretty uncontroversial. At its core, the key underlying motivating question for this analysis appears to not be: should we provide naloxone rescue, but Is naloxone rescue enough? Their conclusion is: No
My guess this is totally in line w how most ppl who study and/or work on the OD crisis (the "Opioid Mafia," as some have quipped) think. I've been working on naloxone access since 2005, primarily to provide more legal support to community-based organizations doing distribution
Models developed in those early days and employed today never contemplated naloxone being used for anything other than emergency. It is not a silver bullet, but it is an important, vital tool that "enables" life
As the @jenniferdoleac @anita_mukherjee analysis highlights, we are doing a terrible job of getting ppl rescued w naloxone connected to evidence-based Tx. Check dismal rates of access to OAT among ppl after non-fatal OD in Mass--one of "progressive" states mass.gov/eohhs/docs/dph…
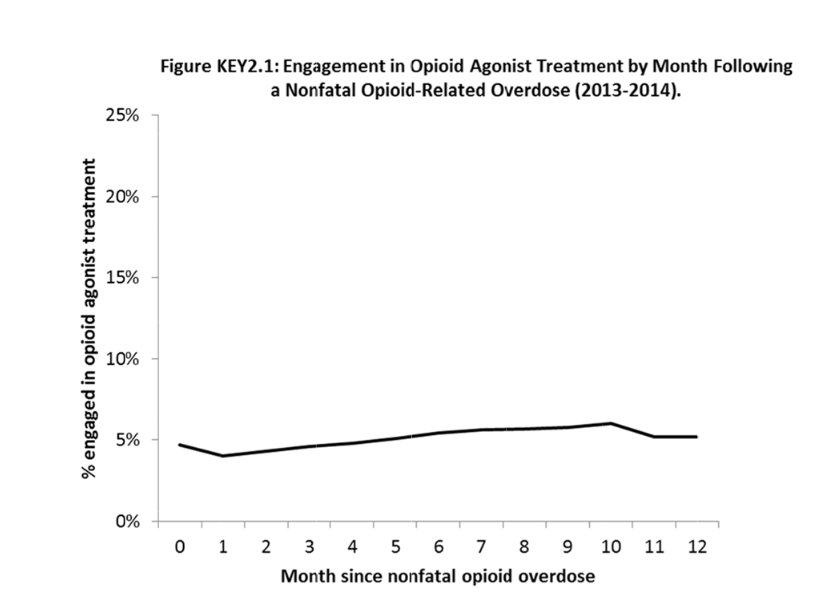
Want to think that the sliver lining here is that, amidst all of the attn to this paper we can shine a light on this shocking and easily remediable element of the OD crisis. Yes we need naloxone, but we also need treatment on demand and other services to help ppl stay alive
/end
/end