
,
113 tweets,
22 min read
Read on Twitter
POISE - the trial that found increased mortality when starting peri-operative beta blockade.
The result was unpleasant, and so we did what we usually do when trials don't show what we hoped.
We say there was something wrong with the trial.
The result was unpleasant, and so we did what we usually do when trials don't show what we hoped.
We say there was something wrong with the trial.
Neither Ashish @ash71us nor I have anything to do with POISE but we are going to discuss it for educational reasons.
Thanks Ashish for offering to take the anti-POISE position.
Thanks Ashish for offering to take the anti-POISE position.
The complaints Ashish raises are common ones, so they are important to study.
1. TOO BIG A DOSE OF BETA BLOCKADE

Name a trial that used an appropriate dose, Ashish?
Well, no answer from Ashish but surely no dose can be more appropriate than that which produced this effect on events?
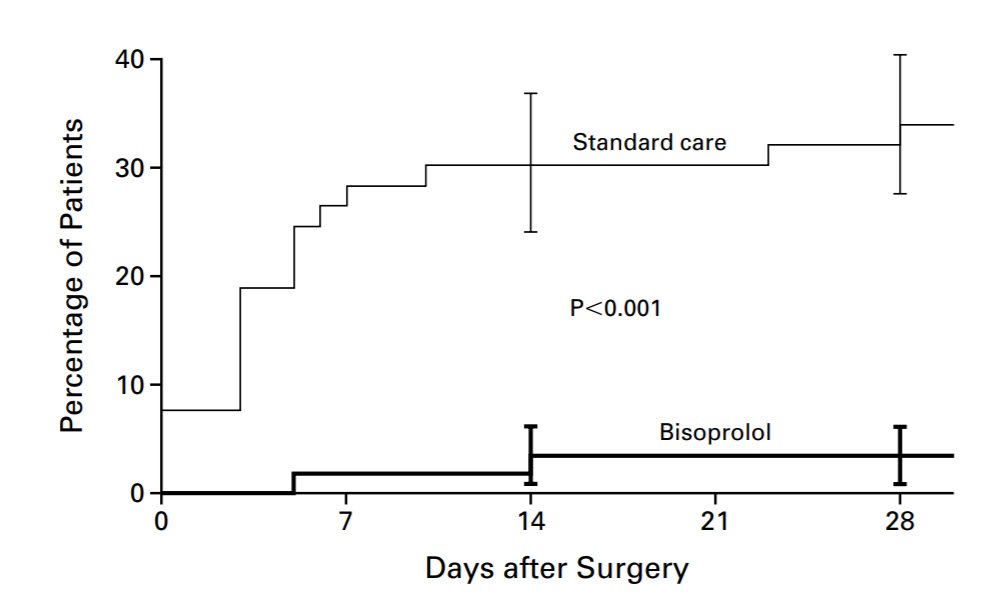
That trial used Bisoprolol.
POISE used Metoprolol CR/XL.
How should we compare the doses to see if the POISE dose was too large?
Remember these were DIFFERENT chemical compounds. Both beta blockers, but different ones.
POISE used Metoprolol CR/XL.
How should we compare the doses to see if the POISE dose was too large?
Remember these were DIFFERENT chemical compounds. Both beta blockers, but different ones.
Compare the heart rates in the left column (beta blocker) with those in the right column (control).
How much lower are the heart rates in the beta blocker arm, on average?
How much lower are the heart rates in the beta blocker arm, on average?

What is the difference between the columns?
Now let's look at POISE.

What was the heart rate reduction in the beta blocker arm of POISE?
So the beta blockade dose in POISE, that lowered heart rate by 7 bpm and BP by 2 mmHg, was:
Complaint 2.
POISE's Perioperative beta blockade, lowering heart rate by 7 bpm and BP by 2mmHg, was too rapid, because it was started within 24 hour pre operatively.
Too hurried!
POISE's Perioperative beta blockade, lowering heart rate by 7 bpm and BP by 2mmHg, was too rapid, because it was started within 24 hour pre operatively.
Too hurried!
Let's take a look at a careful analysis of this.


They'd been stung by letting the fake trials of D Poldermans be waved through to dominate the 2009 guidelines, due to D Poldermans being the chairman of the guideline committee.
So this was now a panel of 115 people who were definitely not D Poldermans.
No messing!
De-Poldered!
So this was now a panel of 115 people who were definitely not D Poldermans.
No messing!
De-Poldered!
Here is their work.
They start with a lie. This was a falsehood first introduced by Poldermans in a debate, and contradicted by the actual trialist who was present.
However, Poldermans friends on the panel, knowing it was false, still reintroduced this statements.
They start with a lie. This was a falsehood first introduced by Poldermans in a debate, and contradicted by the actual trialist who was present.
However, Poldermans friends on the panel, knowing it was false, still reintroduced this statements.
Tell a lie big enough, for long enough, and people will believe you.

This nonsense had long been debunked in a debate between colossal crook Don Poldermans and actual scientist PJ Devereaux.

Here is Poldermans trying to introduce the 400mg concept...
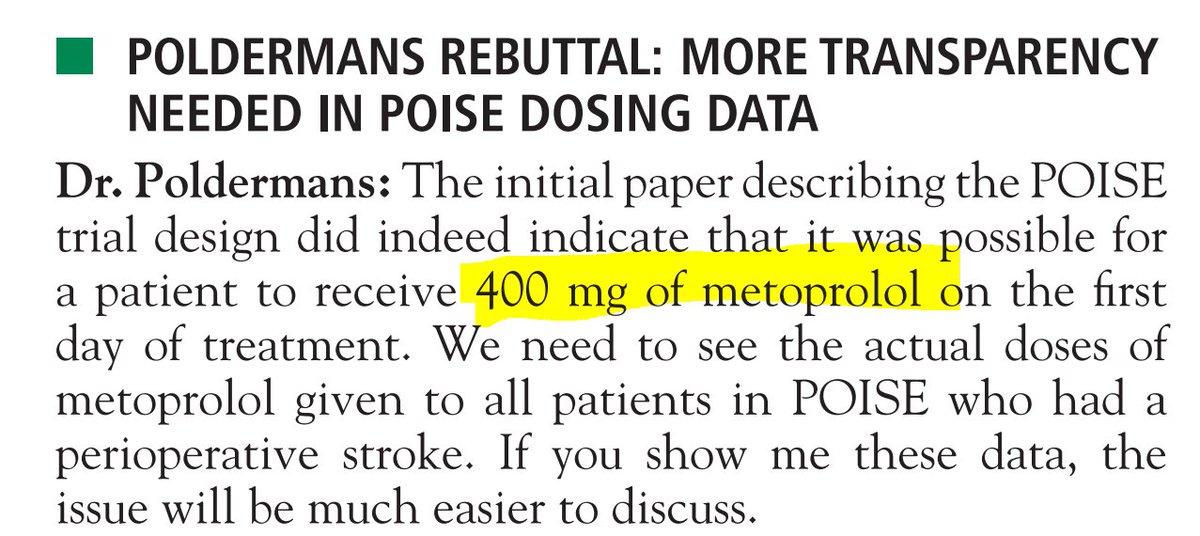
And here is PJ Devereaux, the PI, telling him to not be silly.

Poor Devereaux kept having to ram this point home, because Poldermans kept whining about it, despite being told clearly that it didn't happen.

That ended that. No sensible person would re-raise this Phantom Menace, you would think?
Until the 2014 guideline when the Poldermans Insurgency slipped it back in.
😧
Lies are a powerful tool. Even Ashish was taken in (and he is no Poldermans apologist).
Until the 2014 guideline when the Poldermans Insurgency slipped it back in.
😧
Lies are a powerful tool. Even Ashish was taken in (and he is no Poldermans apologist).
This is the second-most shameful part of the entire guideline.

The dose was *lower* than that of the DECREASE trials for which the Guidelinists retained a secret hankering.
The most shameful part of the guideline?


Reassuring, eh?
In how many HIGH RISK surgery studies, EXCLUDING the 1 DECREASE study, was perioperative beta blockade beenficial?
In how many HIGH RISK surgery studies, EXCLUDING the 1 DECREASE study, was perioperative beta blockade beenficial?
Once you've voted, we can take a look.
Please note that this is not a criticism of these poor people who were writing in and before 2010, long before Poldermans was outed as a charlatan.
Please note that this is not a criticism of these poor people who were writing in and before 2010, long before Poldermans was outed as a charlatan.

Poor guys...

Here indeed is the meta-analytical result.
Look at the section which stratifies the trials by risk level.
High risk.
Good, eh?
"Let's cite this boys! It'll prove we were right all along!"
Look at the section which stratifies the trials by risk level.
High risk.
Good, eh?
"Let's cite this boys! It'll prove we were right all along!"

"Our guidelines will look great! Nobody will check what these high risk trials are, will they? NOBODY EVER CHECKS!"

MAVS

Was it a positive trial?
Here is the second trial. Miller et a, ref 33.

Was it a positive trial for all-cause mortality?
Third trial is Neary et al.
Here is the result.
Here is the result.
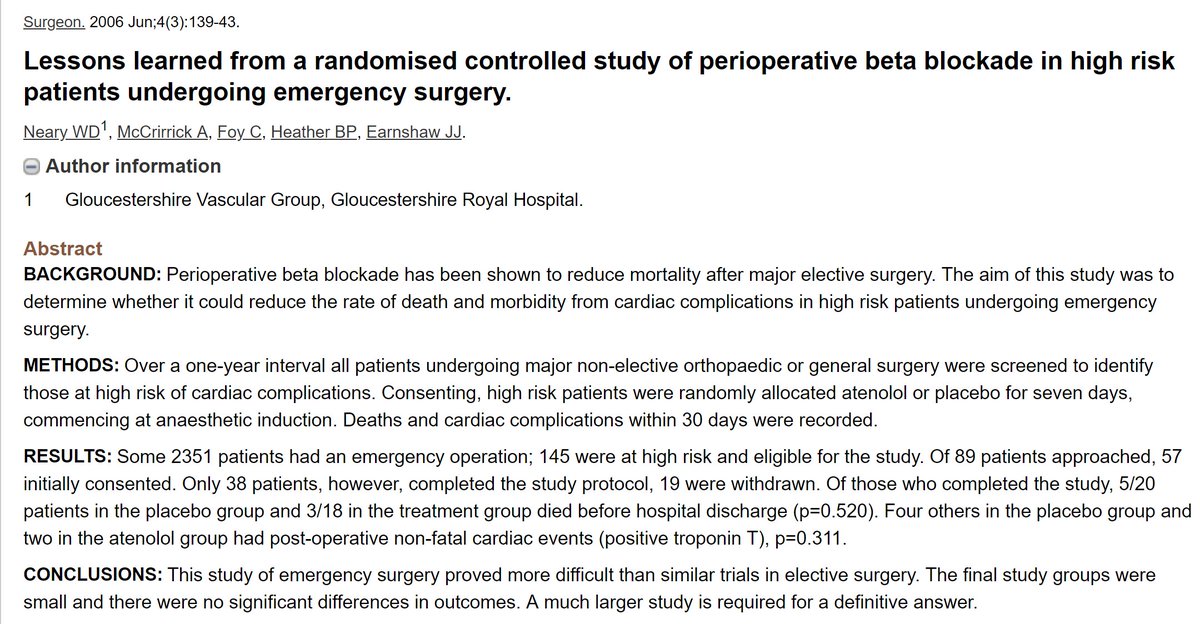
Positive trial?
4th trial. POBBLE.

Positive trial? Less deaths in beta blocker arm?
5th Trial in this High Risk group of trials.
Result:
Result:

How about this one, was it positive?
Yup, it is this trial that swung it, and gave the stunning hazard ratio!
Thank god for this trial.
Where shall we send the prize to, to the author of the trial, because he has saved us?
Thank god for this trial.
Where shall we send the prize to, to the author of the trial, because he has saved us?

Oh dear.
We are gonna have to send the prize award over the barbed wire, using a drone or something.
For the paper is by none other than the Teflon Don.
We are gonna have to send the prize award over the barbed wire, using a drone or something.
For the paper is by none other than the Teflon Don.

To be fair, what the guideline says is technically correct.

It is indeed 5 trials.
4 of which are neutral.
And DECREASE I, the made-up trial, which is stunningly positive for beta blockade, and causes beta blockers to "win".
4 of which are neutral.
And DECREASE I, the made-up trial, which is stunningly positive for beta blockade, and causes beta blockers to "win".
Is that obvious from the wording though?
Should it be so hard to work out when you are being conned by a guideline?
Should the 115 experts put so much effort into concealing things that you would probably want to know, i.e. the advice is actually coming from D Poldermans, despite the guideline being de-Poldered.
Should the 115 experts put so much effort into concealing things that you would probably want to know, i.e. the advice is actually coming from D Poldermans, despite the guideline being de-Poldered.
What about carefully titrating against heart rate?
Sounds good eh?
Carefully doing anything sounds good. Better than being careless.
Sounds good eh?
Carefully doing anything sounds good. Better than being careless.


Clearly vital to titrate to a target heart rate!
Let's have a look at the trials then.

First one is ref 9.
Oh dear.
Oh dear.

Second is ref 24.
Oh, deary, deary me. It's the Teflon Don's other masterpiece, DECREASE-IV.
Oh, deary, deary me. It's the Teflon Don's other masterpiece, DECREASE-IV.

Third is ref 25.
Now this looks more promising from the "not being fictional" point of view.
Now this looks more promising from the "not being fictional" point of view.

Ah. Zero events.

Fourth:

Oh, again nobody died.

Fifth, ref 38.
(Surely it shouldn't be this difficult to work out whether a guideline is true or not)
(Surely it shouldn't be this difficult to work out whether a guideline is true or not)


Oh dear. No deaths. Good for them, bad for us.

So, let's review.

In these dose-titrating trials ("Yes" row)
There were 2 deaths out of about 700 in the beta blocker arms
And 14 out of about 700 in the control arms.
Is that
There were 2 deaths out of about 700 in the beta blocker arms
And 14 out of about 700 in the control arms.
Is that
In those 6 trials, 4 of the trials had zero deaths.
So where were the deaths from?
So where were the deaths from?
Yes, they must be from the two.
And what were these trials, pray tell?
The saviours of beta blockade?
Oh ...
And what were these trials, pray tell?
The saviours of beta blockade?
Oh ...

... my ....

... god!
The supposedly de-Poldered guideline is telling people how wonderful beta blockade is when you dose-titrate, using a meta analysis whose events are
Did you know that already?
i.e. do you always trace references in a guideline, and then trace the references of those references, and then count the number of events and work out where everything comes from?
i.e. do you always trace references in a guideline, and then trace the references of those references, and then count the number of events and work out where everything comes from?
Most people don't check most things.
Luckily, otherwise the world would grind to a halt.
But sometimes people use our trusting natures to muddle things up, fluff the issue and cover up embarrassment.
Luckily, otherwise the world would grind to a halt.
But sometimes people use our trusting natures to muddle things up, fluff the issue and cover up embarrassment.
In this case the ESC was focussed on convincing everyone it had done nothing wrong. That was its overwhelming priority.
Hence the self-congratulatory editorial, with photos etc.
Hence the self-congratulatory editorial, with photos etc.
It succeeded, but as an unfortunate consequence it had to trash POISE and support Polderman's fake research.
A solution to this would be to develop guidelines in the open, instead of in secret.
That way, ordinary people like you and me can spot when we are being tricked, before the guideline comes into force.
That way, ordinary people like you and me can spot when we are being tricked, before the guideline comes into force.
It might take a lot of work to spot all the jiggery-pokery, but there are a lot of us out here in Twitterland.
I find young fellows are the sharpest, and hardest to trick.
I find young fellows are the sharpest, and hardest to trick.
Any young fellows (or other energetic persons) willing to volunteer to actually read and fact-check guidelines before they are put out?
Better than getting 115 fuddy-duddies that will basically sign anything as long as they get a nice blanket and a cup of cocoa in the evening.
Better than getting 115 fuddy-duddies that will basically sign anything as long as they get a nice blanket and a cup of cocoa in the evening.
Apply here: guideline writers are welcome to recruit from amongst the respondents!

Heh heh you are a vicious piece of work Larry.
I was planning not to mention it but since you force me, let's see how the other cheeky chappies got on?
I was planning not to mention it but since you force me, let's see how the other cheeky chappies got on?
DECREASE I
The original and best.
NEJM insist on keeping it as Top Stuff even though it is mathematically impossible.
The original and best.
NEJM insist on keeping it as Top Stuff even though it is mathematically impossible.

Who could forget DECREASE II.
Somebody told the poor fraud investigation panel that they could just ignore it because nobody did stress echo any more so it doesn't matter if the paper was entirely made up.
Somebody told the poor fraud investigation panel that they could just ignore it because nobody did stress echo any more so it doesn't matter if the paper was entirely made up.

Who stood shoulder to shoulder in this masterpiece of fiction ?

DECREASE III
Who again was a heartbeat away from the Teflon Don?
Who again was a heartbeat away from the Teflon Don?
DECREASE IV
(Yawn if you are finding this a bit repetitious)
(Yawn if you are finding this a bit repetitious)

Fortunately EHJ got proper independent review of all this mischief, to uncover the fraud.

Well surely the guidelines would have had honest people at the tiller ?

Poldermans was the chairman of the perioperative guidelines.
I guess he could order people around within the guideline committee.
Only one person had the authority to reprimand him in that role.
The boss of All the Guideline Chairpeople.
I guess he could order people around within the guideline committee.
Only one person had the authority to reprimand him in that role.
The boss of All the Guideline Chairpeople.
And who was this one hope for the perioperative patients ?
The capo di tutti capi, the caped crusader?
The capo di tutti capi, the caped crusader?
That's the problem.
115 experts or whatever , but almost none of them actually had a duty to do anything to fix the situation.
Everyone can defer to some later date or some committee or some other flim flam.
Everyone can blame someone else.
115 experts or whatever , but almost none of them actually had a duty to do anything to fix the situation.
Everyone can defer to some later date or some committee or some other flim flam.
Everyone can blame someone else.
While the actual strings are pulled by a small group of Top People.
I've asked Jeroen twice in person, once before he was elected president of ESC, and once a couple of months ago in Brussels.
As president of ESC you have the authority and power to simply say, these trials are insecure and should be retracted.
As president of ESC you have the authority and power to simply say, these trials are insecure and should be retracted.
Even just removing your name would be enough. Everyone else would pull their names too, and it would be left with Poldermans alone, and that would be enough for the journals to retract.
But no.
He feels no responsibility for this.
Sad.
But no.
He feels no responsibility for this.
Sad.
Click here to continue

Actually the more I think about it the more i think he isn't actually standing by it. He is just ignoring it because he thinks it will be embarrassing to retract the papers.
He might be right.
In which case it is our fault.
For NOT making him retract it.
For NOT asking him as the first question after each of his hundreds of Presidential lectures:
In which case it is our fault.
For NOT making him retract it.
For NOT asking him as the first question after each of his hundreds of Presidential lectures:
"Did you participate in the fraud or were you just an innocent victim. If innocent why do you not remove yourself from the papers ?"
Can people please ask him every time he lectures or come round to glad hand you?
If we all do it he will eventually agree he is better off in the camp of truth than the camp of crookedness.
If we all do it he will eventually agree he is better off in the camp of truth than the camp of crookedness.
Here is the fundamental problem, pointed out by Michael @Mielewczik.
People don't want to speak plainly and try to stop others too.
So everything gets fluffed and bungled.
And people don't actually understand that we are talking about fake trials.
f1000research.com/articles/6-1995
People don't want to speak plainly and try to stop others too.
So everything gets fluffed and bungled.
And people don't actually understand that we are talking about fake trials.
f1000research.com/articles/6-1995
These guys put the boot into the DECREASE trials.
They show that they were made up.
They show that they were made up.

And here is what the reviewers say.
You can see who the reviewers are and what they say. This is an excellent form of peer review.
Almost as good as Twitter.
You can see who the reviewers are and what they say. This is an excellent form of peer review.
Almost as good as Twitter.

And what do these kind hearted peer reviewers say about the conclusion that the DECREASE trials had manipulation ?

That's the problem.
We bend over backwards to be generous to fraudsters.
These trials never existed.
They were fictional.
Details:
google.com/url?sa=t&sourc…
We bend over backwards to be generous to fraudsters.
These trials never existed.
They were fictional.
Details:
google.com/url?sa=t&sourc…

Read at your peril...

Some people have messaged me to say that I am wrong to suggest that ESC contained a Poldermans-supporting rearguard team.
Well, judge for yourself.
Well, judge for yourself.
For many years, Don Poldermans had been riding high on perioperative euphoria. Genius.
The only person who could do perioperative beta blockade trials properly!
Other people did it, it killed people.
When he did it, it was amazing.
The only person who could do perioperative beta blockade trials properly!
Other people did it, it killed people.
When he did it, it was amazing.
Then suddenly he got caught.
A new and unhappy situation for him.
The situation of being discovered to be a colossal con man.
An awkward situation of being fired by his institution.
Some may have been happy the fraud was discovered.
And would have fired him.
Others not so.
A new and unhappy situation for him.
The situation of being discovered to be a colossal con man.
An awkward situation of being fired by his institution.
Some may have been happy the fraud was discovered.
And would have fired him.
Others not so.

Source: ESC Press Release
escardio.org/The-ESC/Press-…
escardio.org/The-ESC/Press-…
The power of maligning POISE so comprehensively is that all kinds of people start imagining amazing things happening in it.
It's like hypnotism.
It's like hypnotism.

Even @NicholasChrimes - who is no Poldermans puppet - is thinking of 80 mmHg BP drops _induced_ by beta blockade.
Let's look at the reality.
Let's look at the reality.
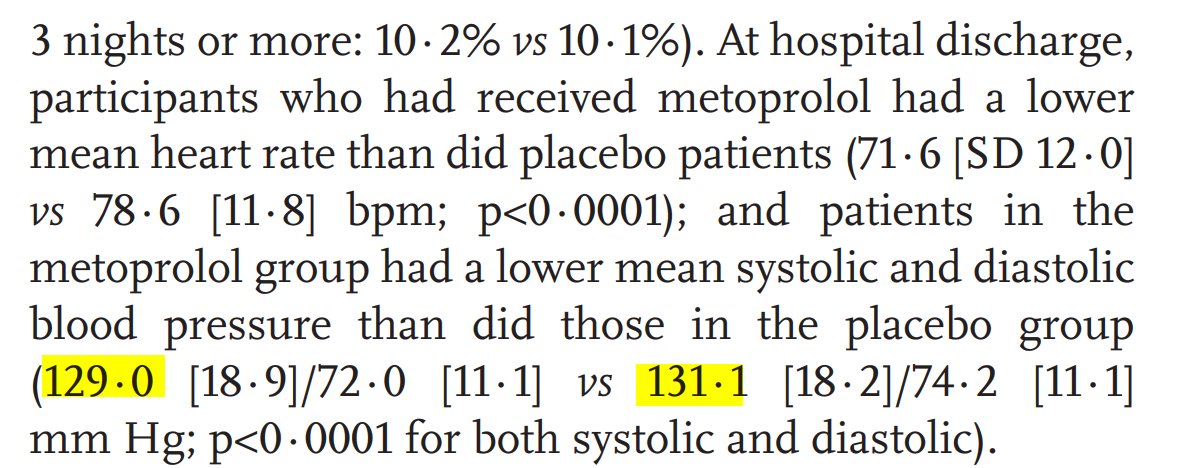
How much lower was the BP in the beta blocker than the placebo arm?
Incidentally, it turns out Nicholas Chrimes developed the superb Vortex Approach to airway management.
It's brilliant because it is aimed at ordinary doctors/nurses, not specialist anaesthetists.
Enjoy! Nice video too.
vortexapproach.org
It's brilliant because it is aimed at ordinary doctors/nurses, not specialist anaesthetists.
Enjoy! Nice video too.
vortexapproach.org










