🚨 New Working Paper 🚨
Long-Term Care Hospitals: A Case Study in Waste
Me + Liran Einav + Amy Finkelstein
ssrn.com/abstract=32393…
This is my first new working paper thread. Thanks to @nomadj1s, @ProfNoto, @SteveCicala, and many others for inspiration.
\begin{thread}
Long-Term Care Hospitals: A Case Study in Waste
Me + Liran Einav + Amy Finkelstein
ssrn.com/abstract=32393…
This is my first new working paper thread. Thanks to @nomadj1s, @ProfNoto, @SteveCicala, and many others for inspiration.
\begin{thread}
Near-consensus there is lots of “waste” in US healthcare system, but little agreement on how to reduce this waste.
We identify a specific and substantial source of waste: Long-Term Care Hospitals (LTCHs), a type of post-acute care facility.
We identify a specific and substantial source of waste: Long-Term Care Hospitals (LTCHs), a type of post-acute care facility.
Tl;dr: We argue that Medicare could save $4.6 billion per year -- without harming patient outcomes -- by not using LTCHs
First, the institutional history. LTCHs came into being through historical accident and aggressive exploitation by the largely for-profit LTCH sector
In 1982, CMS established lump-sum payment system for hospitals (PPS). At the time, there were 40 hospitals that had very long stays and would be put out of business. To keep these hospitals afloat, CMS excluded these 40 hospitals from PPS. These hospitals were the original LTCHs
Today, there are over 400 LTCHs. Unlike regular hospitals, the majority are for-profit. The 2 largest LTCH operators generate profits margins between 16% and 29%. Because of this institutional history, we argue the burden of proof is on LTCHs to show that they create value. 

Now the research design: We use an event-study design based on the entry of LTCHs into local hospital markets. We show reduced form results on the impact of LTCH entry and IV specifications where we use LTCH entry as an instrument for whether a patient is discharged to an LTCH
Since many patients not “at risk” of LTCH discharge, we use ML techniques to identify patients w high ex-ante prob of LTCH discharge. We then allow the first stage to vary with this predicted prob. Approach does not change parameter estimates but shrinks standard errors.
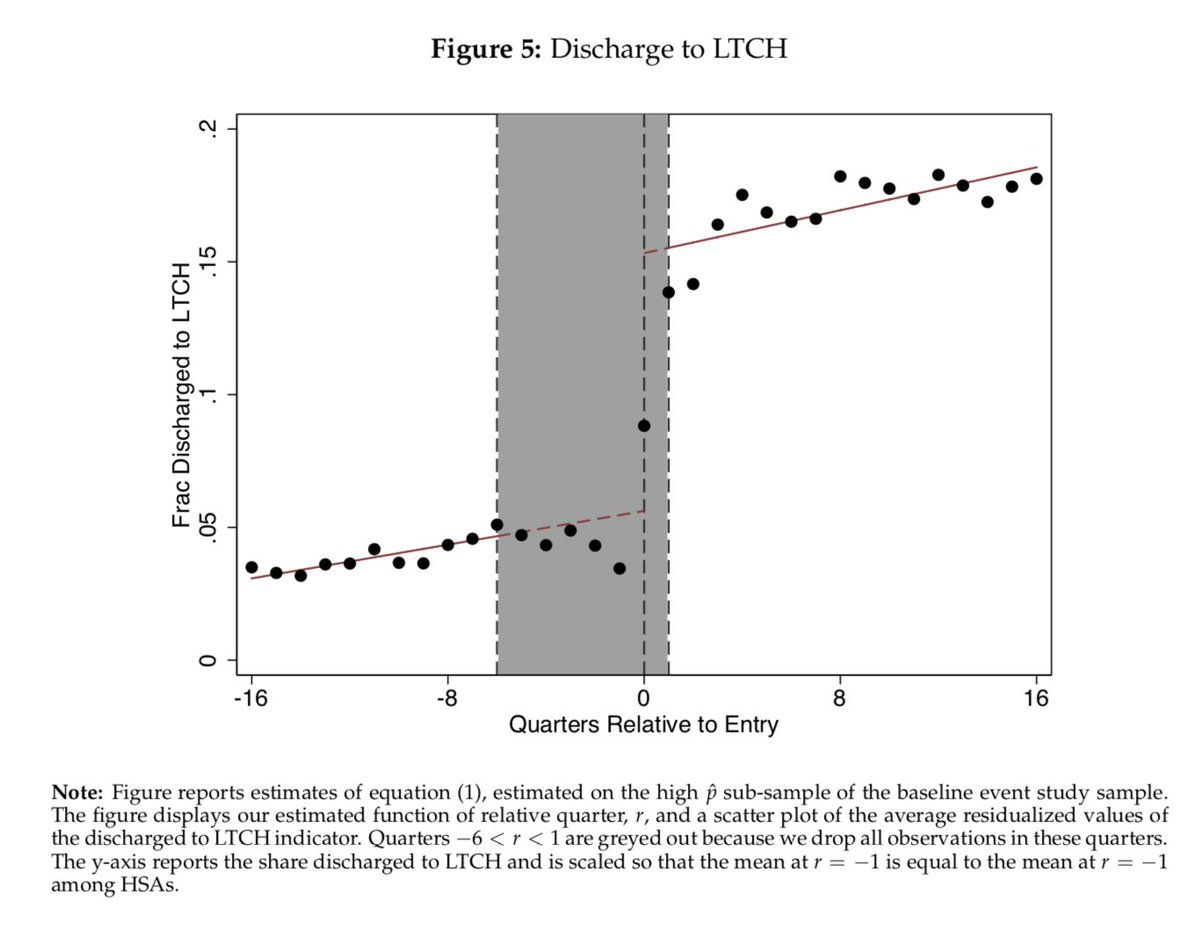
Here’s the first stage of LTCH entry on LTCH discharge in the “high risk” sample. Roughly 9 pp increase discharges to LTCH
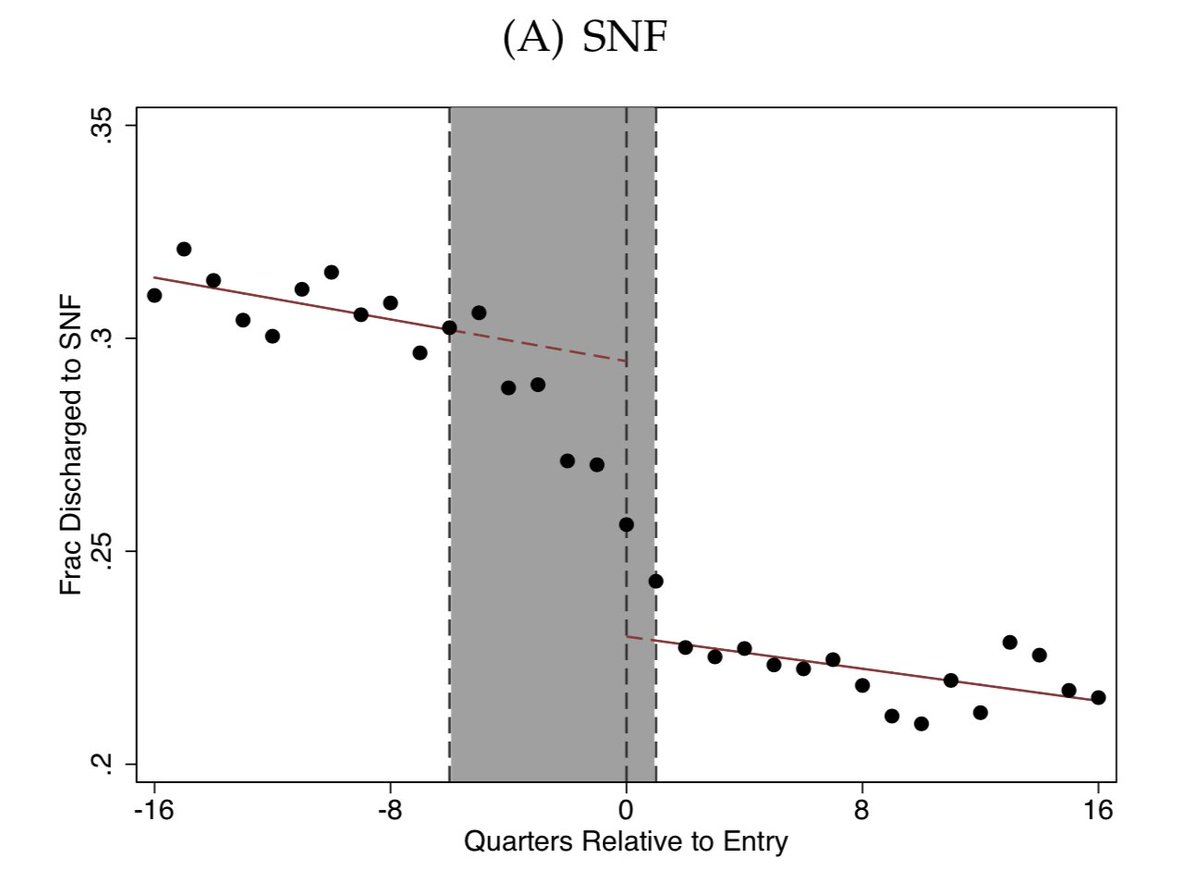
Where are these patients “coming from”? Here’s the event study on discharges to SNFs, another type of post-acute care facility. Drop is roughly 75% of the increase in discharges to LTCHs, implying that 75% of LTCH patients are substituted away from SNFs
What does this mean Medicare costs? A lot. LTCHs are reimbursed $1,400 per day versus $450 per day at SNFs. IV estimates show that for each patient discharged to an LTCH, Medicare spending increases by about $33,000. Here’s the reduced form on costs:

What about patient outcomes? Patients don’t seem to benefit. They owe more money out of pocket, and we find no evidence that they spend less time in institutional care or have better mortality outcome
Caveat 1: Of course, absence of effect is not the same as evidence of its absence. However, institutional history of LTCHs (regulatory carve-out exploited by for-profit industry) suggests “burden of proof” should be to show LTCHs provide medical benefits that justify their costs.
Caveat 2: What about outcomes we don’t measure. Fair point: If LTCHs receive rents, they might do things to recruit more patients. E.g., make it easier for hospitals to discharge to LTCHs, which hospitals might like, or increase the amenities of LTCHs, which patients might like
Of course, this argument could be applied in defense of any form of “excess” health care spending. Again, we take the perspective that the burden of proof is to show that the value of any additional activities justifies the excess costs
Q: SNFs aren’t medically appropriate for all LTCH patients. Wouldn't shutting down LTCH make these patients worse off?
A: We find that LTCH entry reduces length of stay at regular hospitals, suggesting that some patients would be kept at regular hospitals if LTCHs didn’t exist
A: We find that LTCH entry reduces length of stay at regular hospitals, suggesting that some patients would be kept at regular hospitals if LTCHs didn’t exist
Q: Should this excess Medicare spending be classified as “waste”?
A: Depends on your perspective: For gov’t agency that seeks to improve health at lowest cost, spend is wasteful. From perspective of social planner, some of spend is a transfer and should be considered a rent
A: Depends on your perspective: For gov’t agency that seeks to improve health at lowest cost, spend is wasteful. From perspective of social planner, some of spend is a transfer and should be considered a rent
Q: Why haven’t we fixed this problem already?
A: If a sizeable share of the $4.6 billion in incremental spending are rents, the LTCH industry has strong incentives to lobby against regulatory change, which might explain their continued existence. Stay tuned...
\end{thread}
A: If a sizeable share of the $4.6 billion in incremental spending are rents, the LTCH industry has strong incentives to lobby against regulatory change, which might explain their continued existence. Stay tuned...
\end{thread}