,
21 tweets,
16 min read
Read on Twitter
1/19
Left Main Bifurcation: When & How to Approach?
from the recent @crtmeeting #CRT2019 #CRT2020 #LM #SBKCathLab
Left Main Bifurcation: When & How to Approach?
from the recent @crtmeeting #CRT2019 #CRT2020 #LM #SBKCathLab
2/19
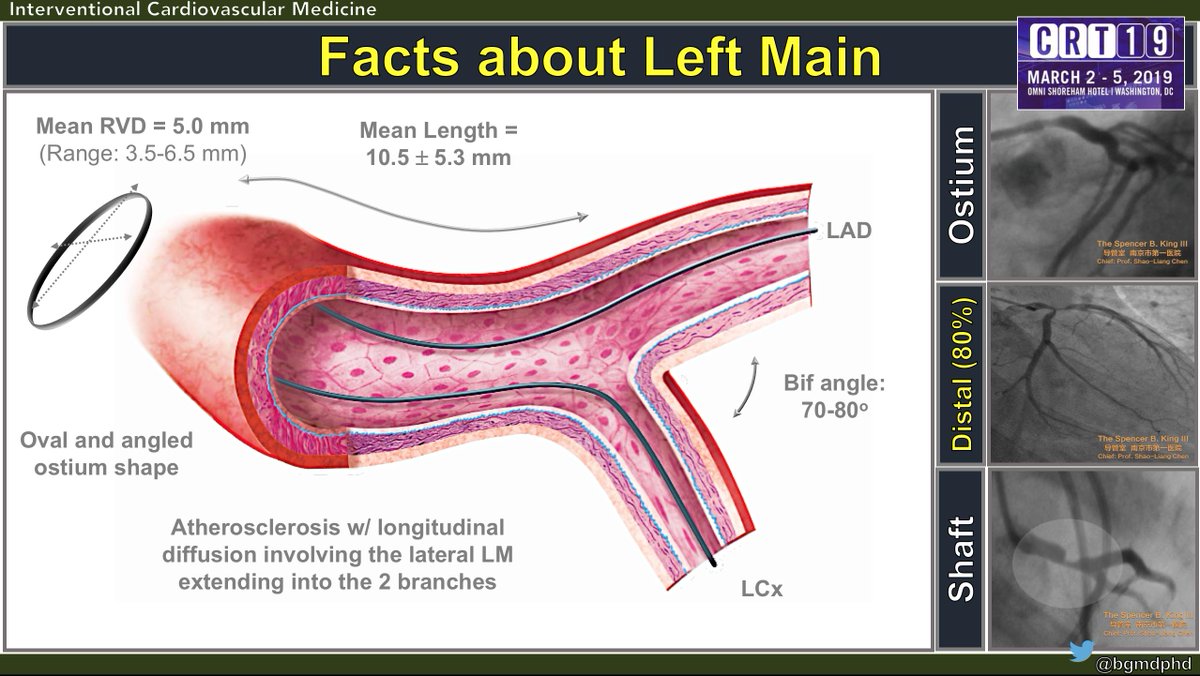
The #LM is oval shaped w/ mean RVD ~ 5mm and mean length ~ 10 mm. The atherosclerotic distribution extends beyond the main shaft to occupy the major side-branches (SB)
The #LM is oval shaped w/ mean RVD ~ 5mm and mean length ~ 10 mm. The atherosclerotic distribution extends beyond the main shaft to occupy the major side-branches (SB)
3/19
The most prevalent location of disease is the distal LM (70%) w/ extension to the LAD/LCx while the remaining 30% comprise the ostium and the mid-shaft.
The most prevalent location of disease is the distal LM (70%) w/ extension to the LAD/LCx while the remaining 30% comprise the ostium and the mid-shaft.

4/19
The criteria that determine LM significance are:
1) Angiographic, w/ DS > 70%
2) IVUS imaging, w/ MLA < 6 mm 2 and
3) Physiologic, w/ FFR < 0.80
The criteria that determine LM significance are:
1) Angiographic, w/ DS > 70%
2) IVUS imaging, w/ MLA < 6 mm 2 and
3) Physiologic, w/ FFR < 0.80

5/19
Treatment starts by assessing anatomic complexity dictated by Syntax (Sx). In Sx<22, ESC guidelines (GL) ▶️ Class I recommendation for PCI while ACC/AHA GL ▶️ Class II. In intermediate 23<Sx<32 both GL agree for PCI as Class II recommendation.
Treatment starts by assessing anatomic complexity dictated by Syntax (Sx). In Sx<22, ESC guidelines (GL) ▶️ Class I recommendation for PCI while ACC/AHA GL ▶️ Class II. In intermediate 23<Sx<32 both GL agree for PCI as Class II recommendation.

6/19
In both LM & non-LM BLs, the SB dictates the treatment strategy. Based on the DEFINITION criteria: SB DS & lesion length will dictate whether the LM or non-LM BL is simple or complex (Cx) which will further guide the stenting strategy.
In both LM & non-LM BLs, the SB dictates the treatment strategy. Based on the DEFINITION criteria: SB DS & lesion length will dictate whether the LM or non-LM BL is simple or complex (Cx) which will further guide the stenting strategy.

7/19
In non-cx distal LM BLs, 1-stent strategy is preferred. 2 wires for the LAD/LCx w/ mandatory POT as stent diameter is sized based on the distal MB RVD. Kissing balloon inflation (KBI) is not mandatory. Switching from 1- to 2-stent strategy depends on the status of the SB.
In non-cx distal LM BLs, 1-stent strategy is preferred. 2 wires for the LAD/LCx w/ mandatory POT as stent diameter is sized based on the distal MB RVD. Kissing balloon inflation (KBI) is not mandatory. Switching from 1- to 2-stent strategy depends on the status of the SB.

8/19
Example of 1-stent strategy in a patient w/ distal LM MEDINA 1,1,0 BL
Example of 1-stent strategy in a patient w/ distal LM MEDINA 1,1,0 BL



11/19
#DKCrush V trial was the most recent RCT that was presented as LBCT @TCTConference @TCTMD in 2017
#DKCrush V trial was the most recent RCT that was presented as LBCT @TCTConference @TCTMD in 2017

13/19
TLF within 1 year occurred in 26 patients (10.7%) assigned to PS, and in 12 patients (5.0%) assigned to DK crush (hazard ratio: 0.42; 95% confidence interval: 0.21 to 0.85; p=0.02)
TLF within 1 year occurred in 26 patients (10.7%) assigned to PS, and in 12 patients (5.0%) assigned to DK crush (hazard ratio: 0.42; 95% confidence interval: 0.21 to 0.85; p=0.02)

14/19
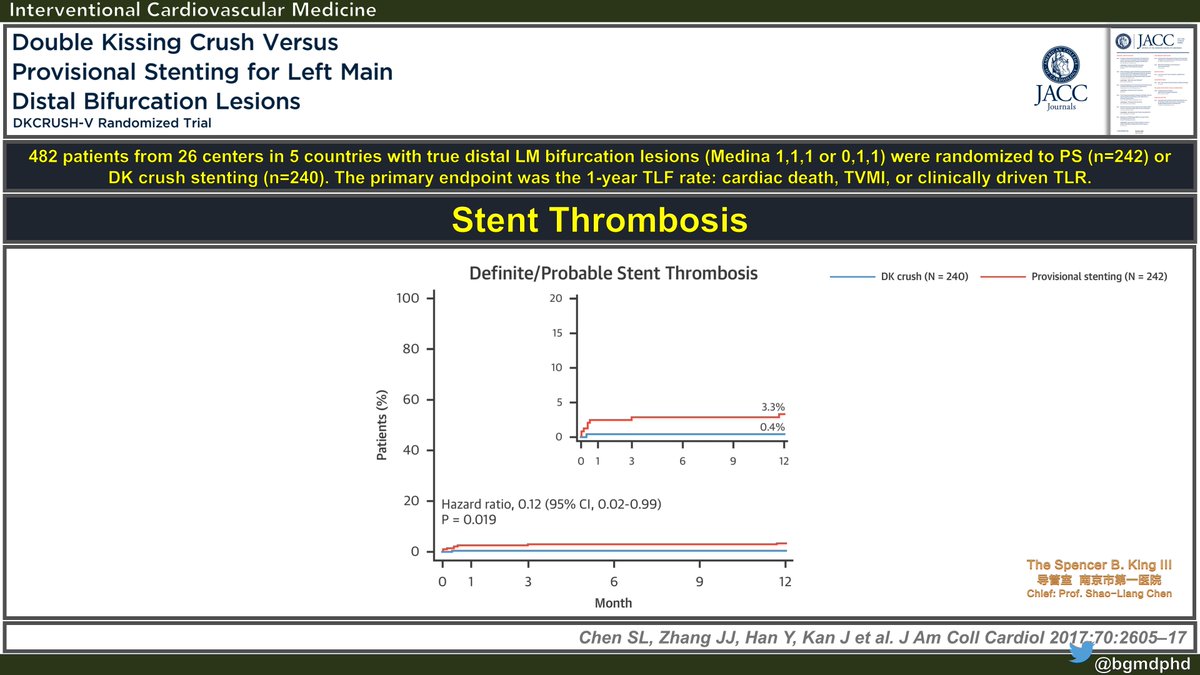
Compared with PS, #DKCrush also resulted in lower rates of definite or probable stent thrombosis: 3.3% vs. 0.4%; p=0.02
Compared with PS, #DKCrush also resulted in lower rates of definite or probable stent thrombosis: 3.3% vs. 0.4%; p=0.02
15/19
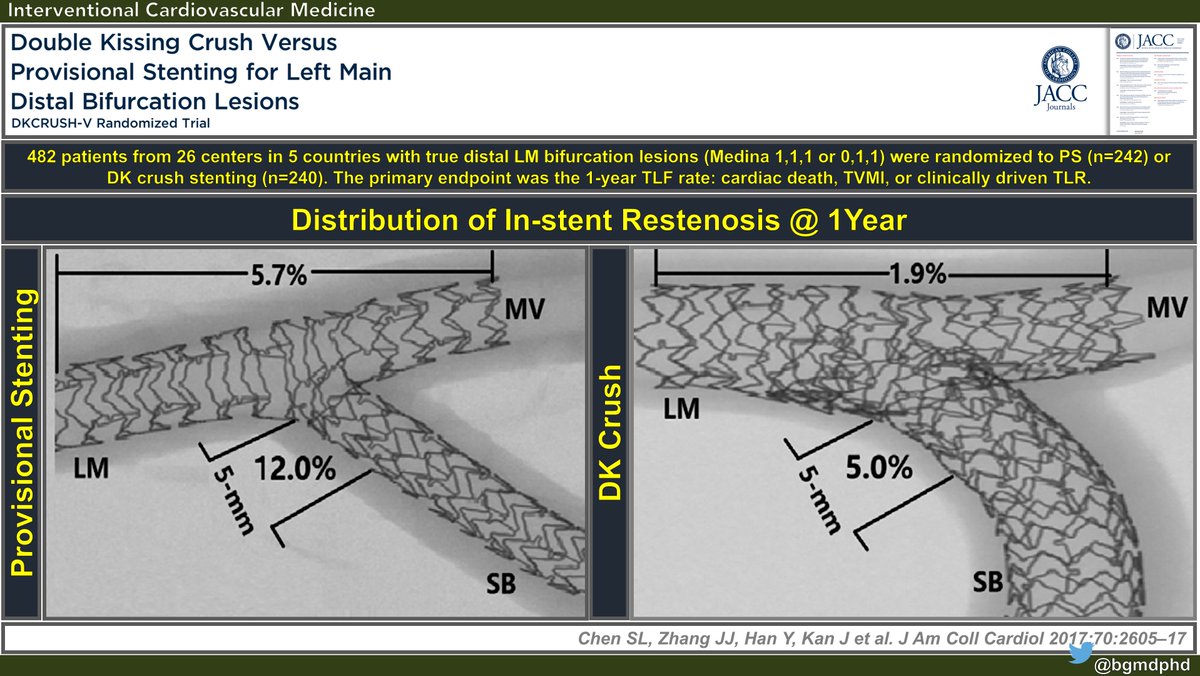
The distribution of ISR was more prevalent in the ostium of the SB. Nevertheless, #DKCrush showed lower restenotic rate compared to PS in this location.
The distribution of ISR was more prevalent in the ostium of the SB. Nevertheless, #DKCrush showed lower restenotic rate compared to PS in this location.
16/19
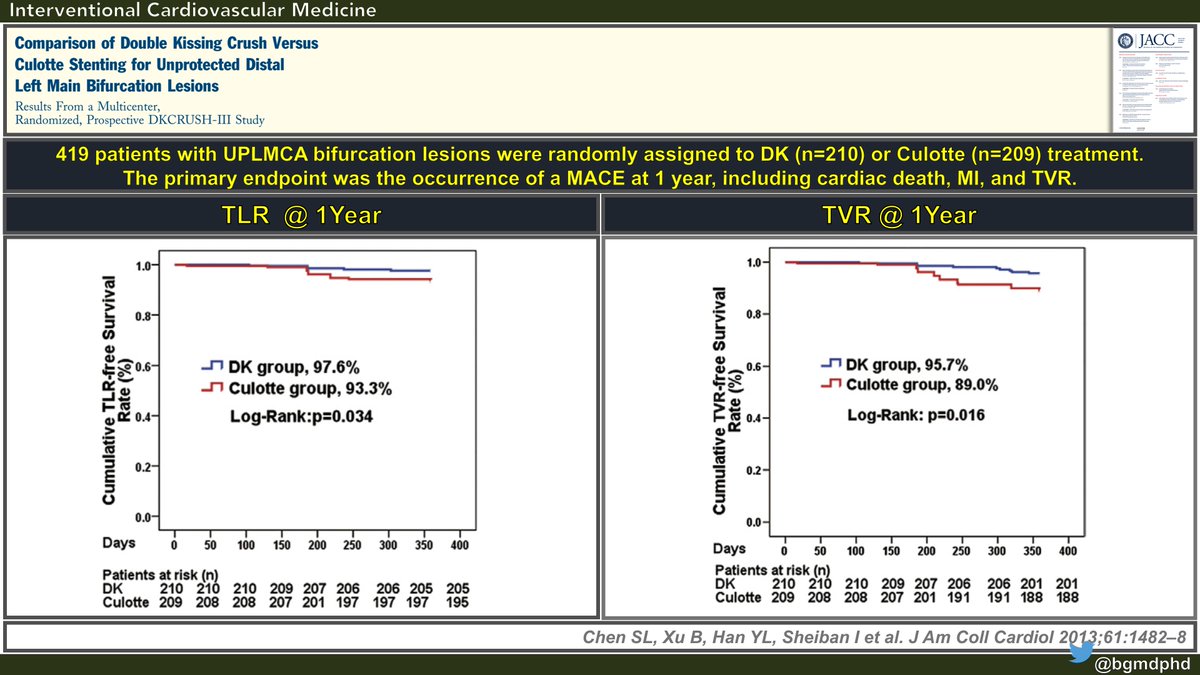
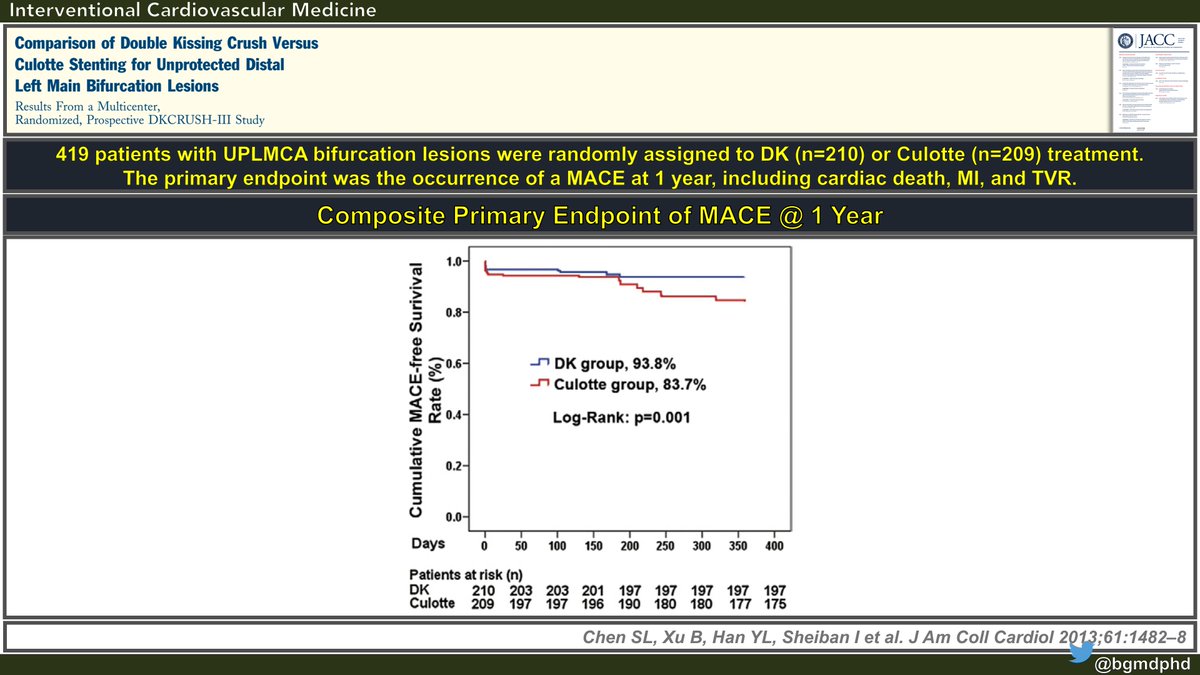
The DKCrush III trial compared the culotte stenting technique with the #DKCrush in Distal UPLM CBLs. 419 patients were enrolled and randomly assigned to DK (n=210) or Culotte (n-209). The primary endpoint was MACE @ 1Y
The DKCrush III trial compared the culotte stenting technique with the #DKCrush in Distal UPLM CBLs. 419 patients were enrolled and randomly assigned to DK (n=210) or Culotte (n-209). The primary endpoint was MACE @ 1Y
17/19
The cumulative MACE-free survival in the #DKCrush group was significantly greater compared to the Culotte group: 93.8% vs. 83.7%, p=0.001
The cumulative MACE-free survival in the #DKCrush group was significantly greater compared to the Culotte group: 93.8% vs. 83.7%, p=0.001
18/19
Similarly, the components of TLR- & TVR-free survival @ 1Y were significantly greater in the #DKCrush group vs. the Culotte group.
Similarly, the components of TLR- & TVR-free survival @ 1Y were significantly greater in the #DKCrush group vs. the Culotte group.