,
32 tweets,
26 min read
Read on Twitter
#WeeklyCardioReview Left main: #PCI or #CABG? A methodological review of #EXCELtrial and #NOBLEtrial, research in context and final answer to what should I do with my patient with #LMdisease. Stay tuned, enjoy and comment
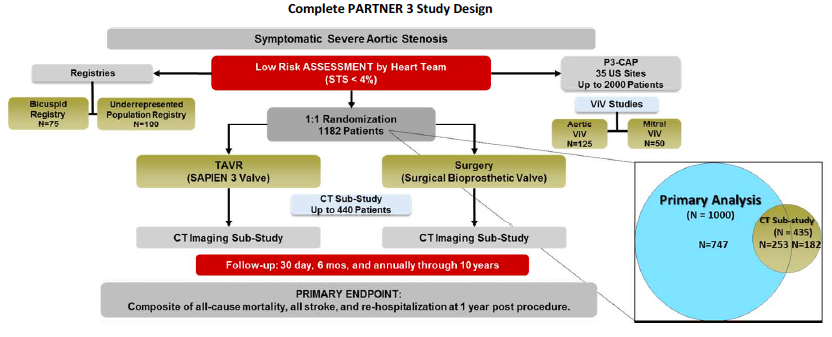
#EXCELtrial Intended population: 2010-2014
1. LM >70% visually, or >50% hemodynamically significant
2. Heart team suitable for both Tx
3. SYNTAX score <32
1. LM >70% visually, or >50% hemodynamically significant
2. Heart team suitable for both Tx
3. SYNTAX score <32
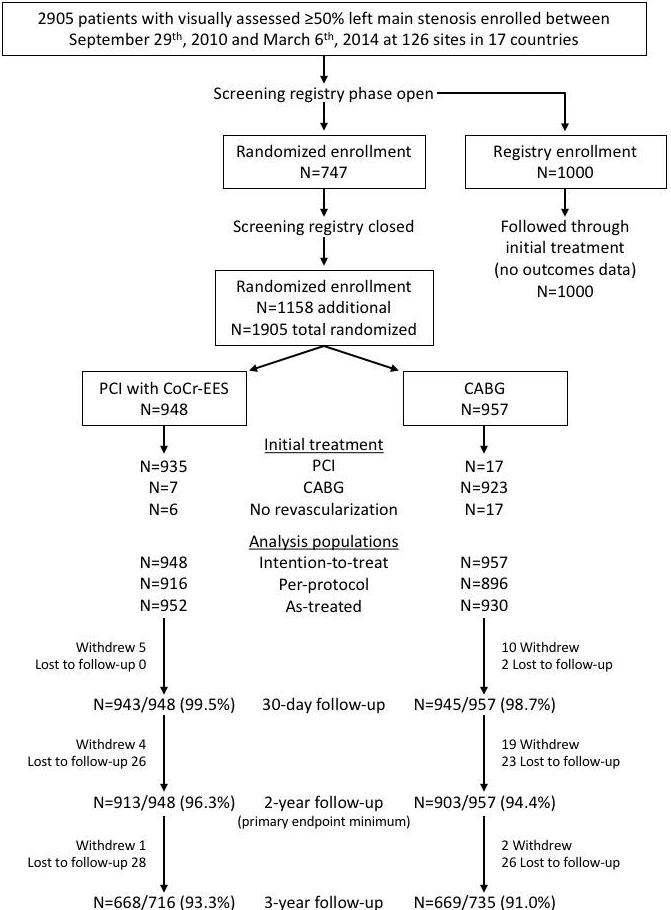
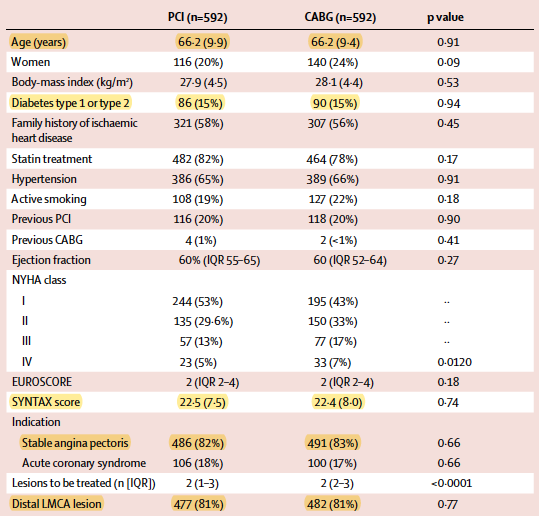
Actual population:
Core lab detected high SYNTAX score (≥33) in 24.2%
Distal LM 80.5%
2 or 3 VD 51.3%
Most common exclusion criteria: Disease too complex for PCI (31.9%)
1905 pts randomized, small cross overs, balanced LTFU
Core lab detected high SYNTAX score (≥33) in 24.2%
Distal LM 80.5%
2 or 3 VD 51.3%
Most common exclusion criteria: Disease too complex for PCI (31.9%)
1905 pts randomized, small cross overs, balanced LTFU


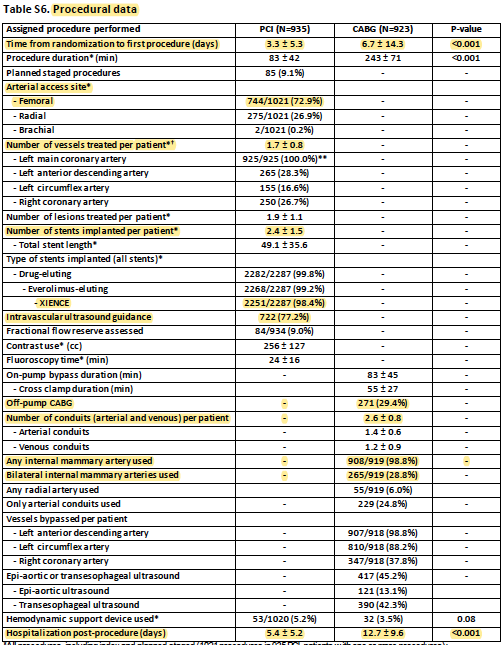
Intervention:
#PCI: #RadialFirst only 26.9%, 1.7 vessesls Tx, 2.4 stents, DES 99.8%, IVUS 77.2%. hospital stay 5.4 d
#CABG: off-pump 29.4%, 2.6 grafts, IMA 98.8%, BIMA 28.8%, 24.8 arterial only. hospital stay 12.7
#PCI: #RadialFirst only 26.9%, 1.7 vessesls Tx, 2.4 stents, DES 99.8%, IVUS 77.2%. hospital stay 5.4 d
#CABG: off-pump 29.4%, 2.6 grafts, IMA 98.8%, BIMA 28.8%, 24.8 arterial only. hospital stay 12.7
Outcomes: death-stroke-MI 3 years, 2ry at 30 days, and adding MACE+revasc at 3 years. Noninferiority margin 4.2 absolute % for upper 97.5% limit (agreed by study cardiac surgeons and interventional cardiologists). Periprocedural MI systematically collected (enzymes and EKG)
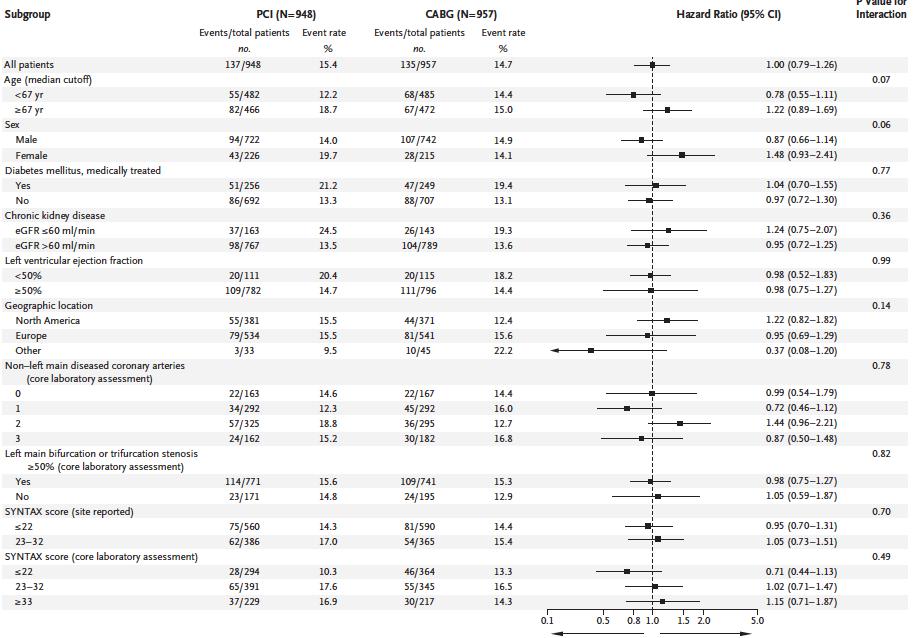
Results: Median FU 3.0yrs. 1ry death-stroke-MI 3yrs 5.4% PCI vs 14.7% CABG group (P = 0.02 noninferiority; HR, 1.00; 0.79-1.26; P = 0.98 superiority). At 30d 4.9% PCI vs 7.9% CABG (P=0.008 superiority), 3yrs MACE+revasc 23.1% PCI vs19.1% CABG group (P = 0.01 for noninferiority)


This was robust to intention to treat, as treated or per protocol analysis. Landmark analysis shows the superiority of PCI at 30 days and inferiority of PCI from 30 days to 3 years (the latter is a not a pure randomized comparison since has immortal type of bias)


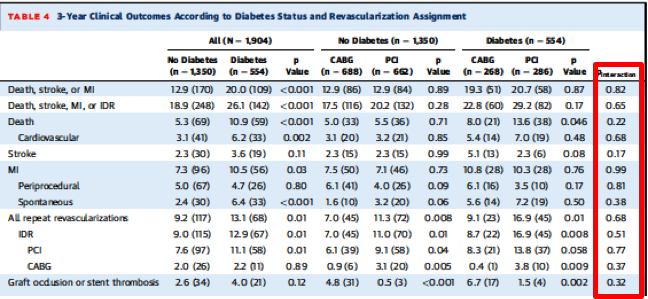
No significant interaction seen, including diabetes and syntax score (the expected trend is observed though).
MAJOR adverse peri procedural events, large reduction by PCI, NNT to avoid one of these patient-important complications was 6.7. This table highlight that 1 in 4 people with CABG will suffer from at least one mayor complication (vs less than 1 in 10 with PCI)

Limitations:
1. 1/4 actually had high SYNTAX score with core lab
2. 3-year, although not short, longer is preferred for more definitive conclusions
3. Definite non-CV death higher in PCI group, while CV death similar, bad luck?
1. 1/4 actually had high SYNTAX score with core lab
2. 3-year, although not short, longer is preferred for more definitive conclusions
3. Definite non-CV death higher in PCI group, while CV death similar, bad luck?
Conclusions: Death-stroke-MI PCI noninferior at 3 years and superior to CABG at 30 days, with marked less morbitidy. Long term trends with better outcomes with CABG to be better determined with 5+ years FU @GreggWStone @djc795 @philgenereux @Drroxmehran @AKappetein 👏
Q for @f2harrell (PHREG master): ok to present results as overall 3-year HR? if 0-30 days the HR favors one intervention and then 30day-3years favors the other (like interaction with time). Does this violate the proportional hazards assumption? how authors should deal with this?
#NOBLEtrial Population: symptomatic CAD plus LM ≥50% visual or FFR ≤0.80, with no more than three additional noncomplex lesions. 1201 randomized, median FU 3.1yrs.
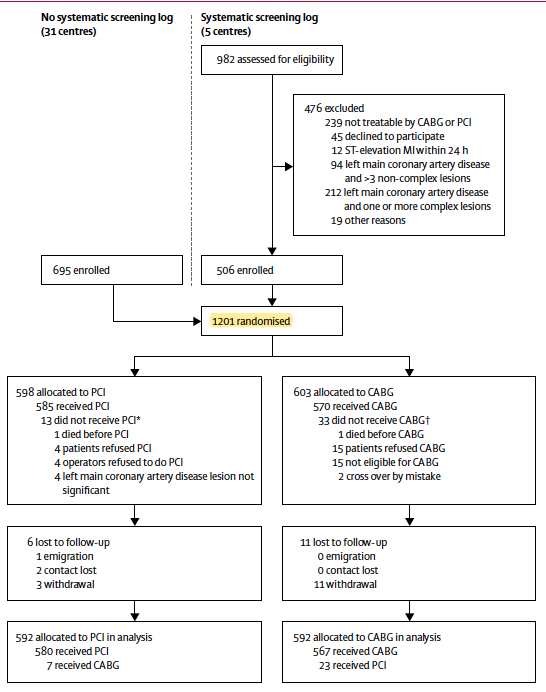


Outcomes: death-stroke-mi-revasc after median of 3 years for 1.35% relative risk difference of non-inferiority. CABG was superior, curve separates after 1 year. Differences driven by MI and revasc, and stroke (latter not consistent with prior literature)



Another atypical behavior is the SYNTAX score subanalysis, moving in the opposite direction of the expected one

Limitations:
1.Repeat revasc in primary outcome: revasc far way less patient-important than death-stroke-mi, and many other methodological aspects favoring CABG
2.Periproedural MI (even large) likely missed (not systematically measured)
3.Frist gen DES used in some patients
1.Repeat revasc in primary outcome: revasc far way less patient-important than death-stroke-mi, and many other methodological aspects favoring CABG
2.Periproedural MI (even large) likely missed (not systematically measured)
3.Frist gen DES used in some patients
Conclusions: CABG superior than PCI for death-stroke-mi-revasc.
Now on, a few key articles...
Now on, a few key articles...
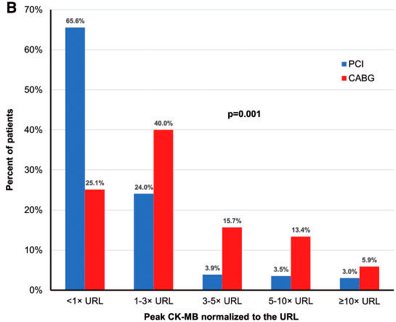
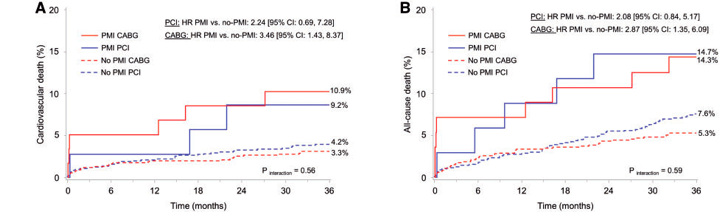
Does periop MI happen more often with CABG? (Figure 1) and is prognostically important? (Figure 2). 75% (vs 35% with PCI) will elevate enzymes, and x5 Ck-MB 20% (vs 6.5% with PCI). NNT 7 to prevent a large prognostic MI with PCI ncbi.nlm.nih.gov/pubmed/30919909
Diabetes: EXCEL (largest individual data analysis of LM) did not observe interaction with diabetes (vs 3VD literature suggesting superiority of CABG over PCI in diabetes with complex CAD) ncbi.nlm.nih.gov/pubmed/30947913
Does SYNTAX score matter? IMO yes. High SYNTAX scores likely benefit from CABG, regardless of LM compromise, and ilkely driven by the extent of CAD rather than LM itself. Is PCI superior to CABG is score is low in LM disease? (Figure) a trend but unknown yet

Quality of life: PCI no worse in symptom control to 36 months and interim analyses, other indices are equal and superior close to the intervention. My guess: if more measurements were done within 3-6 months, more benefit likely



What RCT meta-analysis say? no difference for death-stroke-MI with reasonably narrow confidence intervals, even including the outlier (NOBLE) that did not measure periprocedural MI.

What guidelines say? SYNTAX Score low IA, intermediate IIa and high IIIB. To me is unkown if the data conditioning lower rec for intermediate SS is driven by diabetic status, like in 3VD.

How should I manage my patient with LM?
1. Heart team (minimum: clinical card, surgeon, and IC)
2. Shared decision making: involve the patient in the discussion and incorporate values and preferences
3. Be aware of ur center results (CABG and PCI) for RCT external validity
1. Heart team (minimum: clinical card, surgeon, and IC)
2. Shared decision making: involve the patient in the discussion and incorporate values and preferences
3. Be aware of ur center results (CABG and PCI) for RCT external validity
Opinions: We do not know current benefit of CABG (the historical standard) over med Tx, so difficult to put a line and say: we are sacrificing this X amount of uncertainty of effectiveness (noninferiority margin) of CABG to get the justify the benefit of lower morbidity with PCI
EXCEL longer-term data (5+yrs) lacking, but is not a comparison to see what is better, and even if non-inferiority is not maintained, inferiority is very unlikely to happen given data so far, so question of how much efficacy of long term CABG efficacy can be sacrificed may remain
@threadreaderapp unroll
Those who like to finish with a case. 80+ lady with severe AS and CA on LM CT scan, cath pre TAVR... that calcium is suspicious? would you IVUS? (I personally dont trust FFR in severe AS, despite of "validation" data), happy to discuss