,
9 tweets,
5 min read
Read on Twitter
1/9
Why is “HIT Testing in Low Probability Patients” a TWDFNR?
This tweetorial is a complement to the review published in the June 2019 issue of @JHospMedicine by authors Amanda Li, Lisa Hicks, and @efan75.
journalofhospitalmedicine.com/jhospmed/artic…
Why is “HIT Testing in Low Probability Patients” a TWDFNR?
This tweetorial is a complement to the review published in the June 2019 issue of @JHospMedicine by authors Amanda Li, Lisa Hicks, and @efan75.
journalofhospitalmedicine.com/jhospmed/artic…
2/
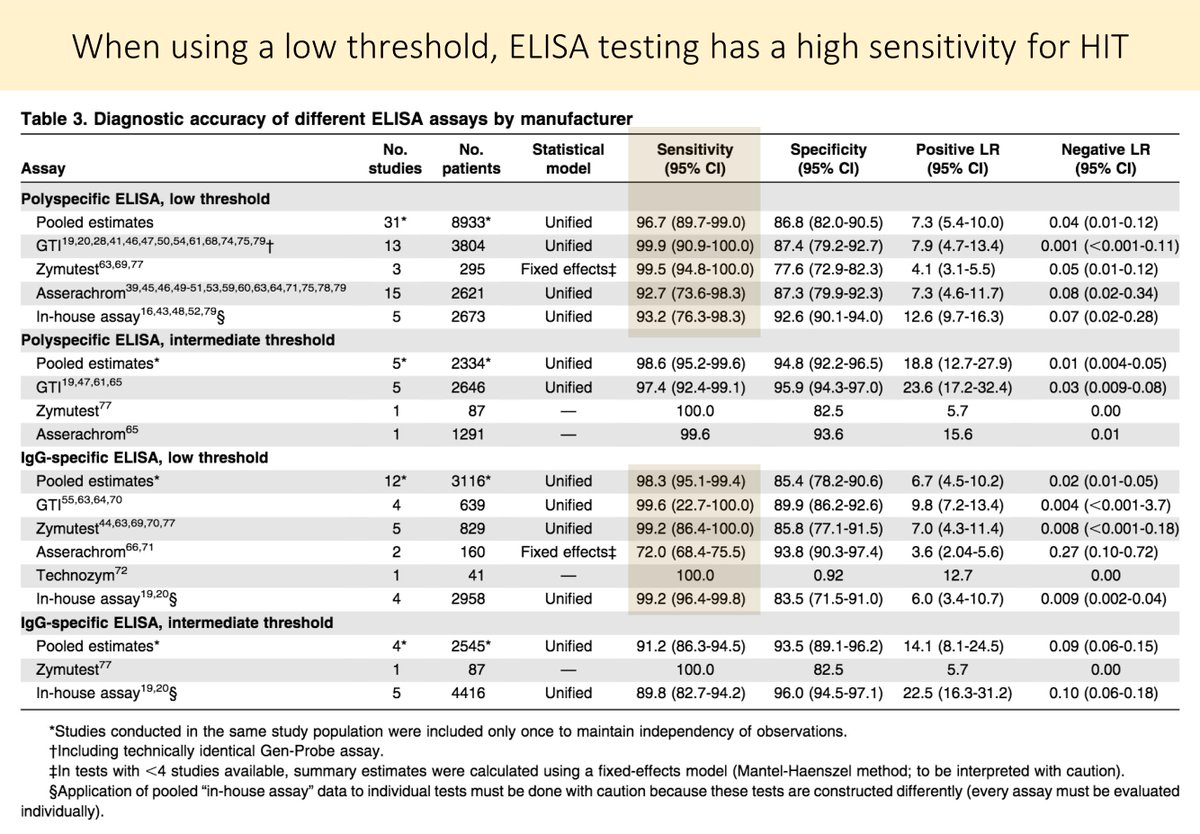
As the authors note, the ELISA test has a sensitivity >95% when the optical density threshold is low. The high sensitivity of the ELISA may make one inclined to use it liberally to evaluate for HIT.
ncbi.nlm.nih.gov/pubmed/26518436
As the authors note, the ELISA test has a sensitivity >95% when the optical density threshold is low. The high sensitivity of the ELISA may make one inclined to use it liberally to evaluate for HIT.
ncbi.nlm.nih.gov/pubmed/26518436
3/
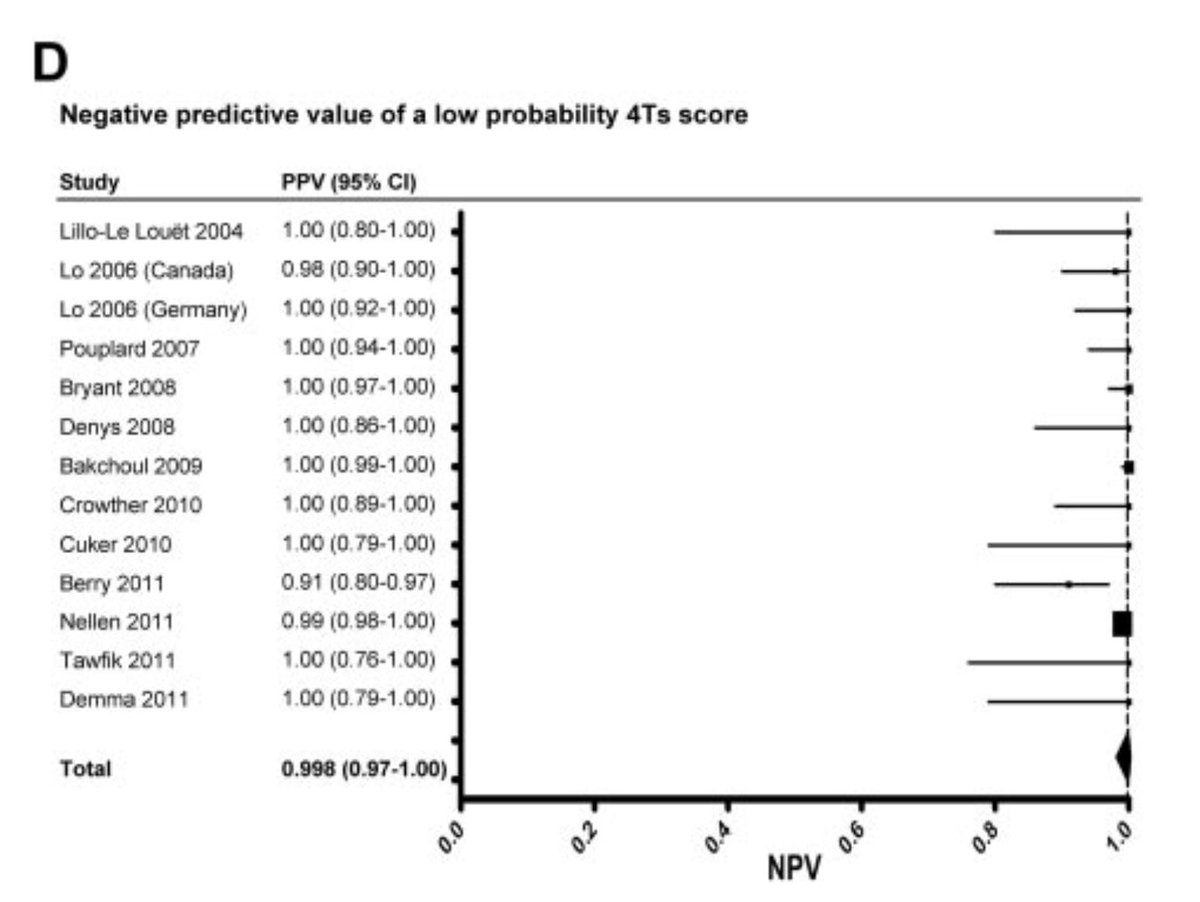
But, there is another way one can effectively rule-out HIT: the 4Ts score.
A 2012 meta-analysis determined that the negative predictive value of a low probability 4Ts score was 99.8%. And, it didn't matter who "performed" the scoring.
ncbi.nlm.nih.gov/pubmed/22990018
But, there is another way one can effectively rule-out HIT: the 4Ts score.
A 2012 meta-analysis determined that the negative predictive value of a low probability 4Ts score was 99.8%. And, it didn't matter who "performed" the scoring.
ncbi.nlm.nih.gov/pubmed/22990018
4/
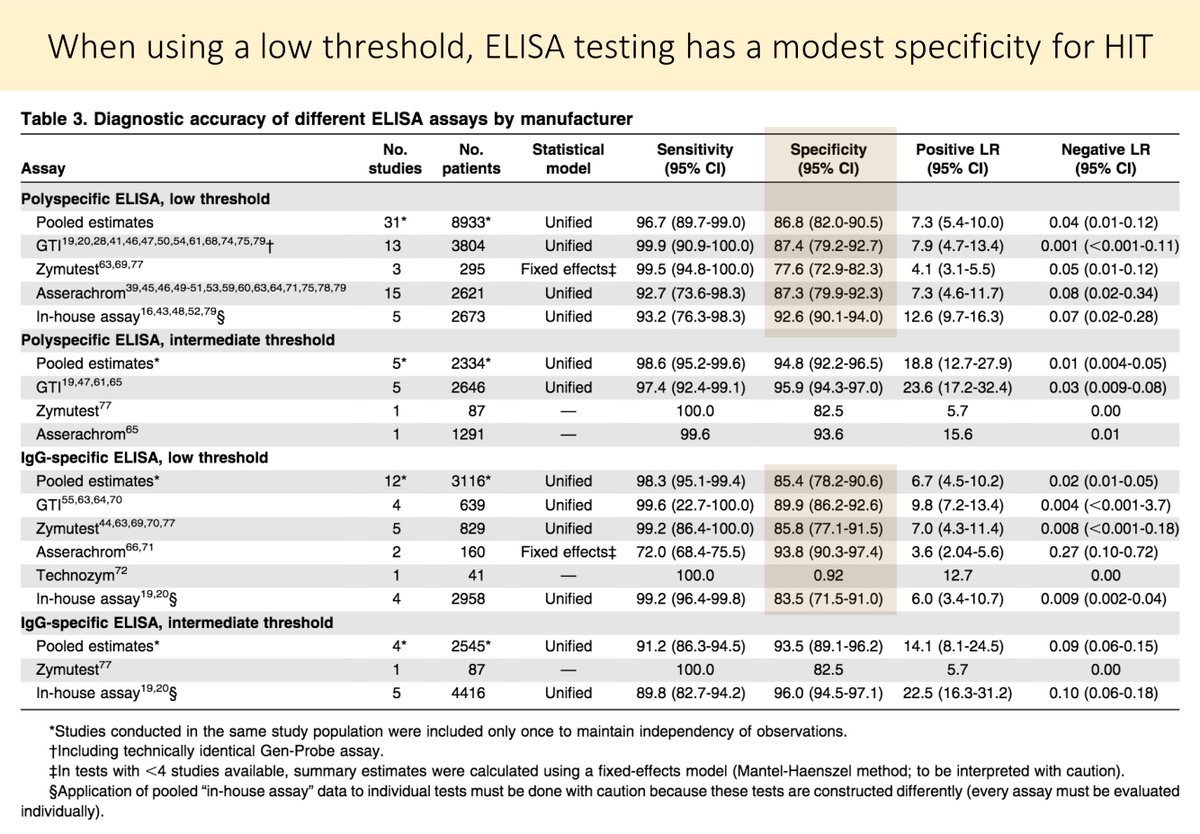
The problem with ELISA testing for HIT is the lack of 100% specificity.
Again using a low optical density threshold, the specificity is more modest (85-90%).
ncbi.nlm.nih.gov/pubmed/26518436
The problem with ELISA testing for HIT is the lack of 100% specificity.
Again using a low optical density threshold, the specificity is more modest (85-90%).
ncbi.nlm.nih.gov/pubmed/26518436
5/
Based on the following values, what percent of patients with a positive HIT ELISA would have HIT?
➜ Pre-test probability: 0.2% (based on a low-probability 4Ts Score) - see tweet 4
➜ Specificity: 90% (i.e., false positive rate of 10%) - see tweet 5
Based on the following values, what percent of patients with a positive HIT ELISA would have HIT?
➜ Pre-test probability: 0.2% (based on a low-probability 4Ts Score) - see tweet 4
➜ Specificity: 90% (i.e., false positive rate of 10%) - see tweet 5
6/
The answer is 2 (see the picture for the calculations).
Applying the ELISA for HIT to patients with a low pre-test probability results in far more false positives than true positives.
The answer is 2 (see the picture for the calculations).
Applying the ELISA for HIT to patients with a low pre-test probability results in far more false positives than true positives.

7/
And, as the authors of the review note, the high false positive rate can result in more testing, unnecessary treatment with medications like argatroban, and inappropriate assignment of heparin allergies.
And, as the authors of the review note, the high false positive rate can result in more testing, unnecessary treatment with medications like argatroban, and inappropriate assignment of heparin allergies.
8/
The authors close with a discussion of situations in which ELISA testing for HIT may be warranted and what one should do instead. Here are their full recommendations.
The authors close with a discussion of situations in which ELISA testing for HIT may be warranted and what one should do instead. Here are their full recommendations.

9/9
To read more about why HIT Testing in Low Probability Patients is a #TWDFNR, check out the full Open Access review by Amanda Li, Lisa Hicks, and @efan75 published in this month's @JHospMedicine
journalofhospitalmedicine.com/jhospmed/artic…
To read more about why HIT Testing in Low Probability Patients is a #TWDFNR, check out the full Open Access review by Amanda Li, Lisa Hicks, and @efan75 published in this month's @JHospMedicine
journalofhospitalmedicine.com/jhospmed/artic…