,
10 tweets,
4 min read
Read on Twitter
THREAD
1/
Eponyms are falling out of favor in medicine. They aren't descriptive and essentially require twice the memory space to recall both the name & the associated term.
But pancreaticoduodenectomy doesn't exactly roll off the tongue so I suspect the Whipple is here to stay.
1/
Eponyms are falling out of favor in medicine. They aren't descriptive and essentially require twice the memory space to recall both the name & the associated term.
But pancreaticoduodenectomy doesn't exactly roll off the tongue so I suspect the Whipple is here to stay.
2/
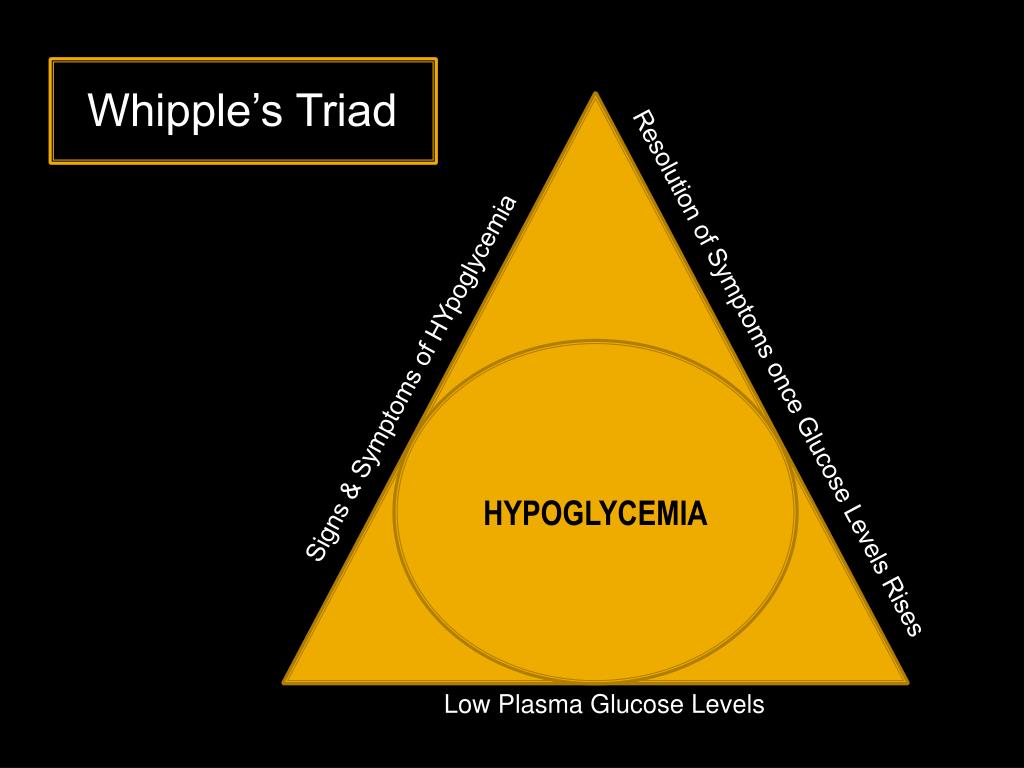
Dr. Allen Whipple was a pioneering surgeon whose contributions to the field also include a still-relevant understanding of insulinomas (see also: Whipple's triad).
Still his incisive approach to the pancreas, small intestine, and bile ducts remains why he is best-remembered
Dr. Allen Whipple was a pioneering surgeon whose contributions to the field also include a still-relevant understanding of insulinomas (see also: Whipple's triad).
Still his incisive approach to the pancreas, small intestine, and bile ducts remains why he is best-remembered
3/
I have no operative skills myself so I like to describe that the Whipple-performing surgeon does to the upper abdomen what Picasso did to faces: radical rearrangements that, in the end, bare some vague semblance to the original orientation of features.
I have no operative skills myself so I like to describe that the Whipple-performing surgeon does to the upper abdomen what Picasso did to faces: radical rearrangements that, in the end, bare some vague semblance to the original orientation of features.

4/
When I had to undergo the surgery myself two years ago @IntermtnMedCtr, I made the somewhat bizarre, deliberately exhibitionist request that the procedure be live-Tweeted so that the step-by-step process could be visualized for other patients contemplating the operation.
When I had to undergo the surgery myself two years ago @IntermtnMedCtr, I made the somewhat bizarre, deliberately exhibitionist request that the procedure be live-Tweeted so that the step-by-step process could be visualized for other patients contemplating the operation.
5/
My surgeons graciously agreed to have the wonderful @intermountain social media team in the OR and they documented the events of the day sequentially, which you can revisit here: wakelet.com/wake/e82752c4-…
My surgeons graciously agreed to have the wonderful @intermountain social media team in the OR and they documented the events of the day sequentially, which you can revisit here: wakelet.com/wake/e82752c4-…
6/
I am so grateful to have this documentation, both for my own surreal out-of-body experience but much more so for the demystification of a much-feared procedure.
I firmly believe that knowledge empowers patients and can dispel at least some of oncology's anxious uncertainty.
I am so grateful to have this documentation, both for my own surreal out-of-body experience but much more so for the demystification of a much-feared procedure.
I firmly believe that knowledge empowers patients and can dispel at least some of oncology's anxious uncertainty.
7/
To be clear, this surgery is not to be taken lightly.
Dr. Whipple died in 1963; over a half-century later, his namesake intervention still carries significant morbidity & mortality (I was cited a 3% risk of death, a number that loomed large the sleepless night before the op)
To be clear, this surgery is not to be taken lightly.
Dr. Whipple died in 1963; over a half-century later, his namesake intervention still carries significant morbidity & mortality (I was cited a 3% risk of death, a number that loomed large the sleepless night before the op)
8/
This @nejm study validates that the procedure is least risky when performed in a high-volume center, so it is entirely appropriate for patients to ask their operative team about caseload and outcomes:
nejm.org/doi/full/10.10…
This @nejm study validates that the procedure is least risky when performed in a high-volume center, so it is entirely appropriate for patients to ask their operative team about caseload and outcomes:
nejm.org/doi/full/10.10…
10/
And so, I do recognize the profound privilege I received on August 7th, 2017: a new lease on life and a forever-altered perspective on what it means to be a patient.
I send all those in the oncology community my sincere gratitude and solidarity.
oftumorsandmen.com/whipple-blog/2…
And so, I do recognize the profound privilege I received on August 7th, 2017: a new lease on life and a forever-altered perspective on what it means to be a patient.
I send all those in the oncology community my sincere gratitude and solidarity.
oftumorsandmen.com/whipple-blog/2…