,
9 tweets,
5 min read
Read on Twitter
1/ The answer to our last poll: cisplatin
nephsim.com/case-13-diagno…
Below, a brief #tweetorial to walk through a simplified approach to #hyponatremia
Step 1: What type of hypoNa are we dealing with here?
Ex: Na 128 meq/L, glucose 500 mg/dL, BUN 20 mg/dL serum osm 292 mosm/kg
nephsim.com/case-13-diagno…
Below, a brief #tweetorial to walk through a simplified approach to #hyponatremia
Step 1: What type of hypoNa are we dealing with here?
Ex: Na 128 meq/L, glucose 500 mg/dL, BUN 20 mg/dL serum osm 292 mosm/kg
2/
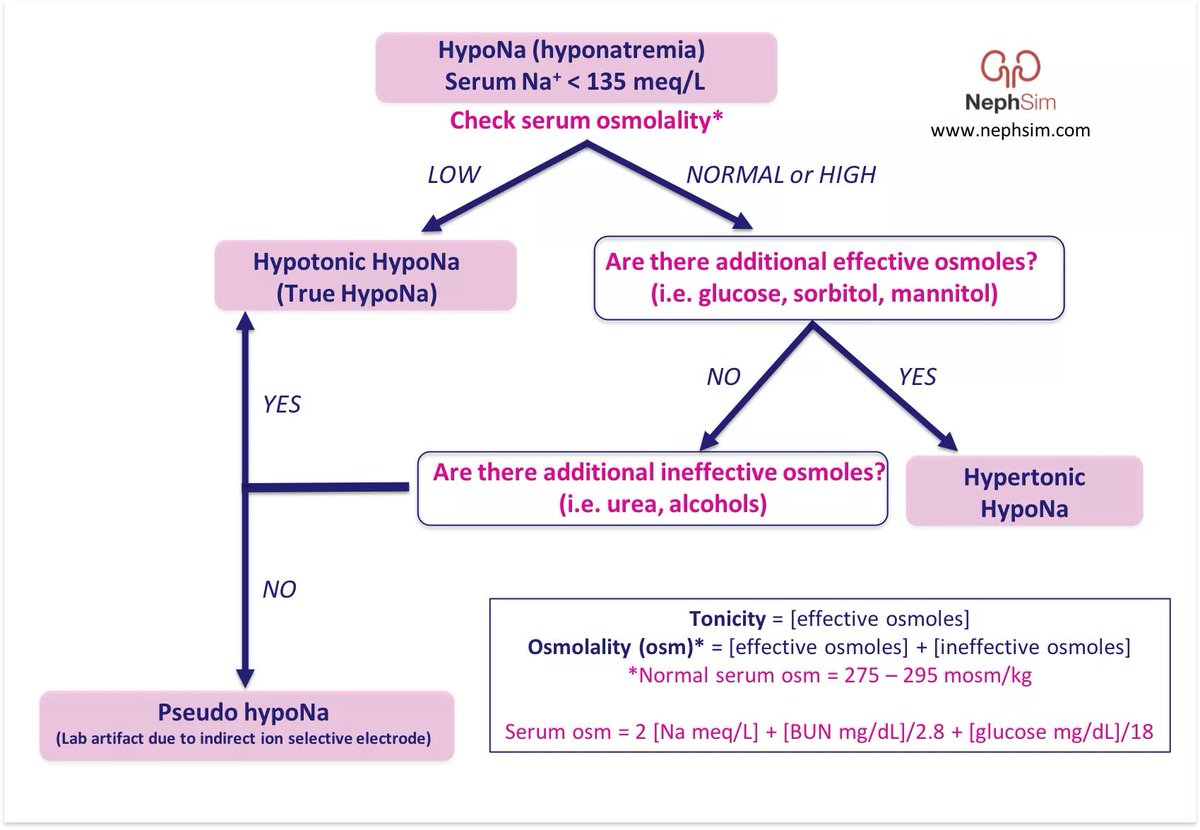
Remember the difference between tonicity (a measure of EFFECTIVE osmoles) & osmolality (measure of both EFFECTiVE & INEFFECTIVE osmoles)
Effective osmoles cannot cross between the ECF and ICF, thus draw water across the cell membrane.
nephsim.com/image-gallery/
Remember the difference between tonicity (a measure of EFFECTIVE osmoles) & osmolality (measure of both EFFECTiVE & INEFFECTIVE osmoles)
Effective osmoles cannot cross between the ECF and ICF, thus draw water across the cell membrane.
nephsim.com/image-gallery/
3/
If serum osm not low with hypoNa, we must look for the presence of ⬆️effective & ineffective osmoles (that ⬆️osmolality)
-If we find⬆️ effective osmoles ➡️ HYPERtonic hypoNa
-If we find ⬆️ INeffective osmoles ➡️ HYPOtonic hypoNa
-If neither ➡️ PseudohypoNa
If serum osm not low with hypoNa, we must look for the presence of ⬆️effective & ineffective osmoles (that ⬆️osmolality)
-If we find⬆️ effective osmoles ➡️ HYPERtonic hypoNa
-If we find ⬆️ INeffective osmoles ➡️ HYPOtonic hypoNa
-If neither ➡️ PseudohypoNa
4/
Back to the case from the poll. Here, we have a serum sodium of 120 meq/L and a serum osm of 268 mosm/kg ➡️ HYPOtonic hypoNa
Next step: what's the effective circulating (or arterial) volume (ECV)? Look to the urine sodium and your physical exam.
nephsim.com/case-13-diagno…
Back to the case from the poll. Here, we have a serum sodium of 120 meq/L and a serum osm of 268 mosm/kg ➡️ HYPOtonic hypoNa
Next step: what's the effective circulating (or arterial) volume (ECV)? Look to the urine sodium and your physical exam.
nephsim.com/case-13-diagno…
5/
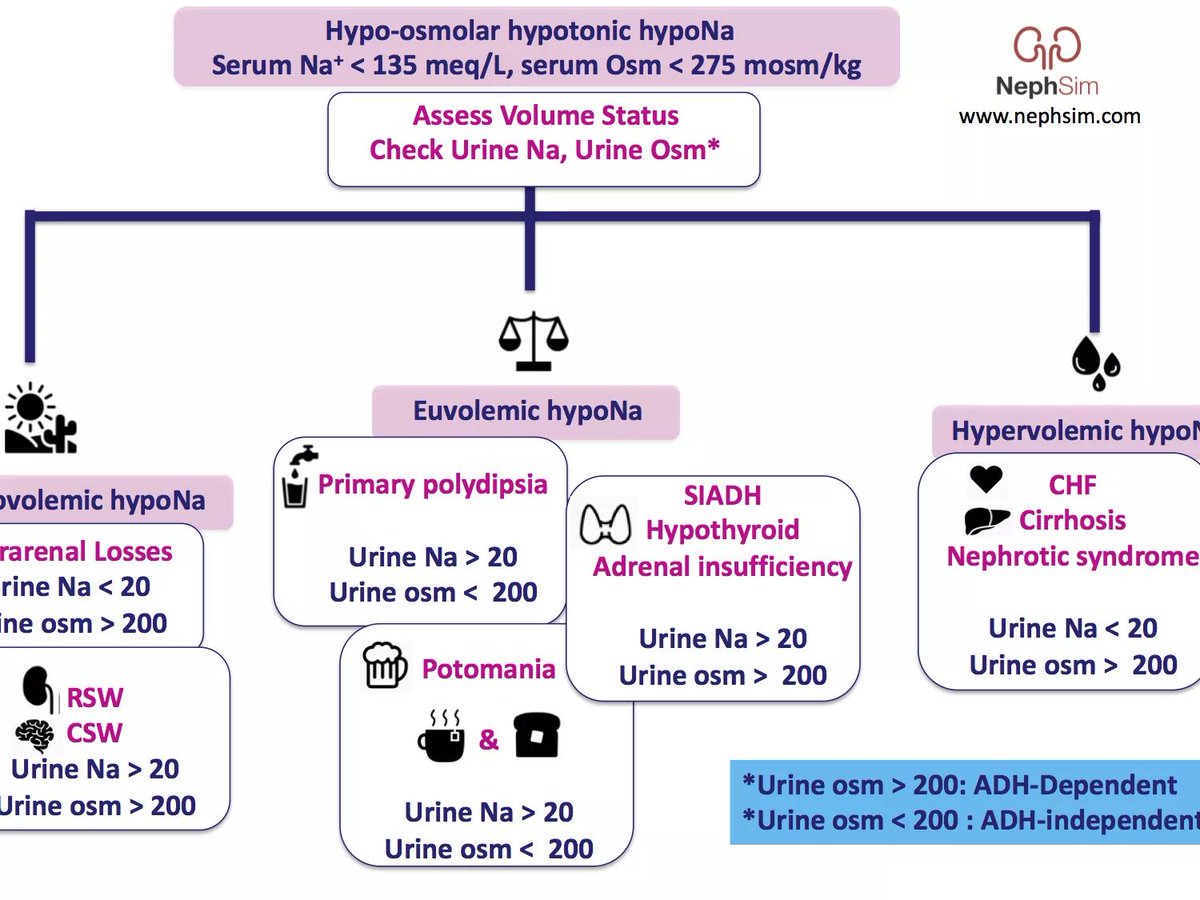
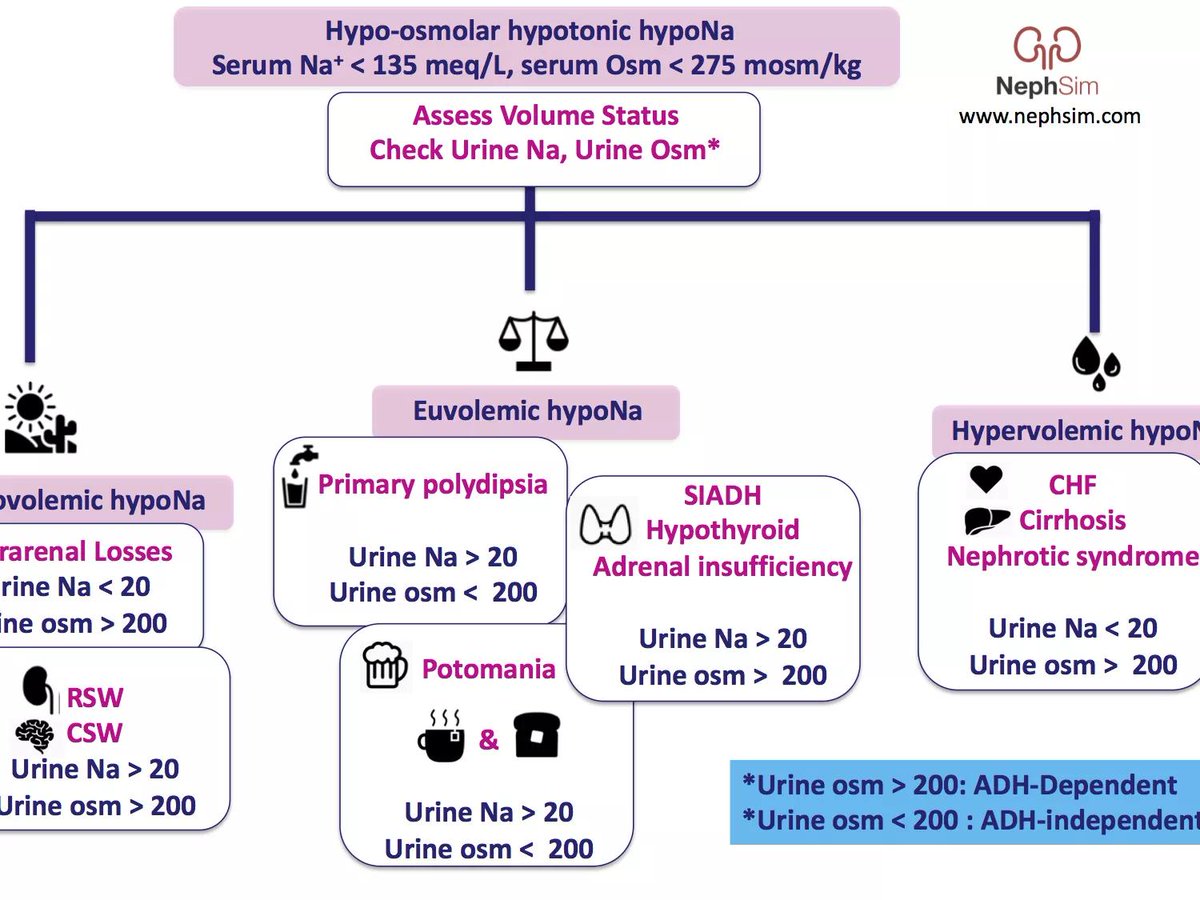
Below is an #infographic outlining hypotonic hypoNa etiologies.
In our case, the pt appears volume depleted.
A urine sodium < 20 often indicates a sodium-avid state of the nephron and thus low ECV. But here the urine sodium is 53...
nephsim.com/case-13-diagno…
Below is an #infographic outlining hypotonic hypoNa etiologies.
In our case, the pt appears volume depleted.
A urine sodium < 20 often indicates a sodium-avid state of the nephron and thus low ECV. But here the urine sodium is 53...
nephsim.com/case-13-diagno…
6/
Next question: is the hypoNa ADH-dependent? The urine osm can help us here.
A high urine osm indicates activity of ADH at the distal nephron. Here, our urine osm is elevated (744 osm/kg!) - suggesting an ADH-driven hypoNa.
nephsim.com/case-13-diagno…
Next question: is the hypoNa ADH-dependent? The urine osm can help us here.
A high urine osm indicates activity of ADH at the distal nephron. Here, our urine osm is elevated (744 osm/kg!) - suggesting an ADH-driven hypoNa.
nephsim.com/case-13-diagno…
7/
So what's driving the ADH? Is it "appropriate"?
Our physical exam revealed that the patient was volume depleted - which will lead to an appropriate increase in ADH release.
Now we have hypovolemic hypoNa, w/ appropriate ADH release. How do we explain the high urine Na?
So what's driving the ADH? Is it "appropriate"?
Our physical exam revealed that the patient was volume depleted - which will lead to an appropriate increase in ADH release.
Now we have hypovolemic hypoNa, w/ appropriate ADH release. How do we explain the high urine Na?
8/
A renal-salt wasting state would explain both hypovolemia and high sodium in the urine, bringing us to our diagnosis of #cisplatin induced renal salt wasting.
🧂🧂🧂
A renal-salt wasting state would explain both hypovolemia and high sodium in the urine, bringing us to our diagnosis of #cisplatin induced renal salt wasting.
🧂🧂🧂
9/
#Hyponatremia take home points:
1. Compare the serum osmolality to the tonicity (tonicity = EFFECTIVE osmoles only)
2. Assess the volume status (physical exam, urine Na)
3. Assess ADH activity (urine osm)
nephsim.com/case-13-diagno…
#FOAMed
#Hyponatremia take home points:
1. Compare the serum osmolality to the tonicity (tonicity = EFFECTIVE osmoles only)
2. Assess the volume status (physical exam, urine Na)
3. Assess ADH activity (urine osm)
nephsim.com/case-13-diagno…
#FOAMed