,
15 tweets,
4 min read
Read on Twitter
Beef with maintenance fluids.
This salty #tweetorial will pose some questions and explore common pitfalls of using IV fluids “for maintenance.”
This salty #tweetorial will pose some questions and explore common pitfalls of using IV fluids “for maintenance.”
Poll: how would you describe dripping 100 mL (a third of a coke can) per hour of NS or LR into a patient who has a heart rate of 100 and a high BUN?
Good choice!
If someone is volume down, give them a bolus.
“Maintenance fluids” are often the wrong choice because they’re not enough.
If someone is volume down, give them a bolus.
“Maintenance fluids” are often the wrong choice because they’re not enough.
More often, those MFs are too much.
What’s the harm in a little extra IV fluid, you say? Let’s do some easy math.
What’s the harm in a little extra IV fluid, you say? Let’s do some easy math.
Quick background:
Isotonic fluids
- Normal saline: 154 mEq Na, 154 Cl
- Lactated ringers: 130 Na, 110 Cl, 28 lactate, some K and Ca
Hypotonic fluids
- Half/quarter NS: divide above by 2 or 4
- D5W: 50g dextrose (200 calories) per L
Can add dextrose or K to any fluid.
Isotonic fluids
- Normal saline: 154 mEq Na, 154 Cl
- Lactated ringers: 130 Na, 110 Cl, 28 lactate, some K and Ca
Hypotonic fluids
- Half/quarter NS: divide above by 2 or 4
- D5W: 50g dextrose (200 calories) per L
Can add dextrose or K to any fluid.
But what’s up with the 0.9% of normal saline? This means 0.9% by mass. As in 9g NaCl per 1000g (1L) water.
100cc/hr NS = 2.4 L/day = 22 grams of IV salt per day. After day. After day.
Few hearts/kidneys are healthy enough to handle that.
100cc/hr NS = 2.4 L/day = 22 grams of IV salt per day. After day. After day.
Few hearts/kidneys are healthy enough to handle that.
But we don’t use NS anymore, we’ve been SALT-ED and SMARTed into using LR!
bit.ly/2XFF7AR
bit.ly/2XL1akV
Yep. But as far as salt load and potential for overload, LR is about the same.
bit.ly/2XFF7AR
bit.ly/2XL1akV
Yep. But as far as salt load and potential for overload, LR is about the same.
Random question.. did anybody here wake up at 3 am last night to eat 6 pickles and drink a liter of regular coke?
Me neither.
We’re all NPO after midnight. Being NPO overnight isn’t a reason to start someone in IV fluids.
Me neither.
We’re all NPO after midnight. Being NPO overnight isn’t a reason to start someone in IV fluids.
Ok fine, there ARE times you need maintenance fluids. If someone’s not gonna be eating/drinking for days (awaiting a PEG over weekend, altered or sedated, refractory nausea, etc), please don’t allow hypernatremia... talk about “not nice.”
But usual insensible losses are not normal saline (or LR)
Breath caries free water
Sweat is ~1/4 normal
Staying alive does cost calories
bit.ly/2YTsj6q
So if it’s those losses we’re maintaining, 1-2L per day of D5-1/4NS or D5–1/2NS +/- some K makes most sense.
Breath caries free water
Sweat is ~1/4 normal
Staying alive does cost calories
bit.ly/2YTsj6q
So if it’s those losses we’re maintaining, 1-2L per day of D5-1/4NS or D5–1/2NS +/- some K makes most sense.
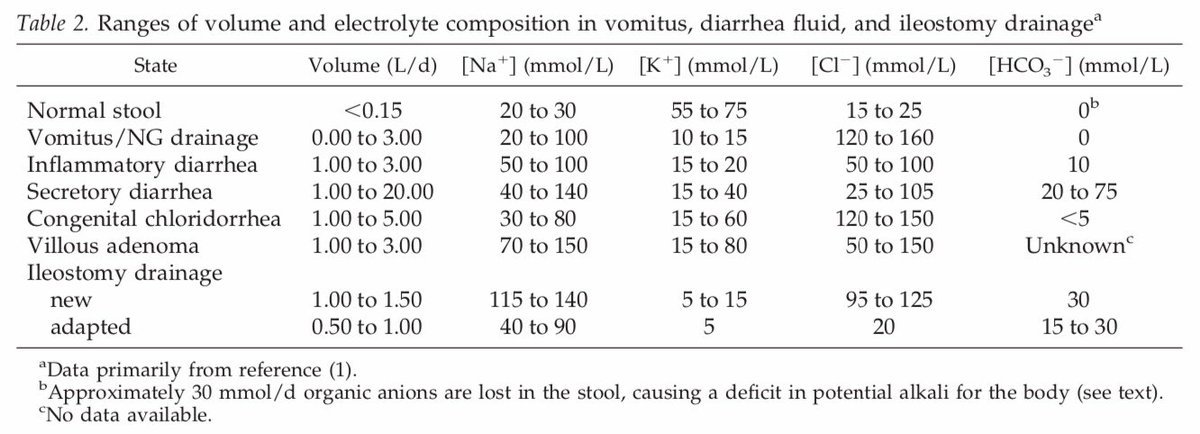
By contrast, if someone is having significant diarrhea, their losses may be closer to isotonic, and if they are not keeping up with PO, continuous LR could be reasonable after bolusing to euvolemia.
bit.ly/30wMxU4
bit.ly/30wMxU4
P.S. Thanks to our med-peds residents, I’ve seen the data that isotonic MF in kids cause less hypoNa. Makes sense, sick folks make ADH. But the hypoNa is rare, and in adults, I see volume OD from fluids >10x as often as hypoNa. So my default remains hypotonic.
Last poll: (Note - I would call this a scenario about replacement fluids, not maintenance)
Lady with pyelo, temp 102, WBC 20. Got abx and 2.5 LR in ED, BP recovered, pulse too, 110 -> 70s. JVP, lung exam normal. She’s eating drinking fine.
What fluids do you order now:
Lady with pyelo, temp 102, WBC 20. Got abx and 2.5 LR in ED, BP recovered, pulse too, 110 -> 70s. JVP, lung exam normal. She’s eating drinking fine.
What fluids do you order now:
Either LR or nothing are justifiable:
Nothing: “Looks like we’ve resuscitated enough, why give more? I’ll reassess soon and if HR/BP drift again, I’ll bolus”
LR: “There’s no way she’s done third-spacing. Let’s keep up.” Key here is best-guessing a finite volume.
Individualize.
Nothing: “Looks like we’ve resuscitated enough, why give more? I’ll reassess soon and if HR/BP drift again, I’ll bolus”
LR: “There’s no way she’s done third-spacing. Let’s keep up.” Key here is best-guessing a finite volume.
Individualize.
Take away recs:
- If someone is volume down, bolus LR
- We overuse maintenance fluids and cause lots of iatrogenic HF / volume OD. Be thoughtful about whether indicated.
- If indicated (eg NPO for days), D5-1/2NS @ 75cc/hr may be best default to match hypotonic insensible losses
- If someone is volume down, bolus LR
- We overuse maintenance fluids and cause lots of iatrogenic HF / volume OD. Be thoughtful about whether indicated.
- If indicated (eg NPO for days), D5-1/2NS @ 75cc/hr may be best default to match hypotonic insensible losses