,
16 tweets,
5 min read
Read on Twitter
@Me4Trauma @me4_so A #tweetorial for my #medtwitter and #trauma colleagues.
You assess a patient with a stab wound to the left chest in respiratory distress. Chest XR shows a large hemopneumothorax, and you insert a large-bore chest tube. Do you give antibiotics?
You assess a patient with a stab wound to the left chest in respiratory distress. Chest XR shows a large hemopneumothorax, and you insert a large-bore chest tube. Do you give antibiotics?
Most surgeons are taught that there is no role for antibiotics in chest tube insertion. Few people can cite the evidence for this topic. Most of us are taught about chest tubes as residents and never actually review the primary literature - frankly, they are not a sexy topic.
First, a history lesson. You are now a military trauma surgeon. It's 1952 and you are serving in Korea. A young soldier is brought to you with a GSW to the chest, respiratory distress, decreased air entry, and hypoxia. Do you insert a chest tube?
Until the 1960s, closed chest drainage was considered "seldom necessary and often dangerous" (Valle). The 1958 NATO guidelines suggested repeated percutaneous aspiration without drain insertion for traumatic hemothorax. Chest tubes were considered harmful.
ctsnet.org/article/histor…
ctsnet.org/article/histor…
When closed chest drainage caught on, the debate was not "if" to prescribe antibiotics, it was "for how long" do you prescribe them? In 1981 Dr. Stone et al showed that continuous antibiotics for the duration of the chest drain (+2 days) decreased infections compared to placebo. 

Ten years later, Dr. Demetriades et al compared long-course antibiotics versus prophylactic antibiotics given as a single dose and found no impact on infectious complications. It seems that a long-course is not necessary and we de-escalate our antibiotic durations.

However, evidence was still overwhelmingly opposed to routine antibiotics. The following negative studies favoured no antibiotics: Grover, Stone, Leblanc, Mandal, Locurto, Brunner, Cant, Nichols, Gonzalez, Maxwell, Villegas Carlos, Heydari. Twelve negative studies. Consensus?
Yes, consensus. Every single study was negative. Or rather, statistically insignificant. But were they actually powered to answer the question?
We know that the incidence of infectious complications from chest tubes is around 2.5%. That's around what Stone and Demetriades reported (see above). Also what Ball found. Kwiatt reviews, in depth, chest-drain complications with infection incidence of 1-25%.


So let's look at power. The largest negative study is Maxwell et al, 2004, with n=224.
If antibiotics reduced infection by 75%, and infection incidence is 2.5%, what sample size do we need at a=0.05 b=0.2?
We'd need 1372 patients in our sample. So n=224 ain't cutting it.
If antibiotics reduced infection by 75%, and infection incidence is 2.5%, what sample size do we need at a=0.05 b=0.2?
We'd need 1372 patients in our sample. So n=224 ain't cutting it.
Those 12 prior studies ranging from n=52 to n=224 aren't even close to powered to answer this question. So we need to do a meta analysis. This is what Bosman et al did in 2012 and Ayoub did in 2019.

And here, visually, is precisely WHY we do meta analyses (from Ayoub):

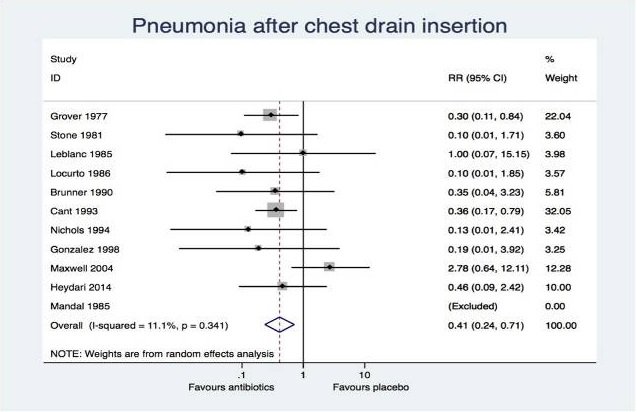
That's 12 under-powered negative studies that, combined, yield a cohort of 1263 patients. Still under-powered but close! And combined, there's a clear statistical advantage shown to giving antibiotics. Notably, EVERY previous study showed a trend to this effect for empyema!
Currently, we estimate that 1 in 40 patients suffers an infectious complication of their chest tube without antibiotics. With 75% empyema and 59% pneumonia reductions by giving antibiotics, that number would be more like 1 in 120. No study was powered for length of stay.
So...
You assess a patient with a stab wound to the left chest in respiratory distress. Chest XR shows a large hemopneumothorax, and you insert a large-bore chest tube. Do you give antibiotics?
You assess a patient with a stab wound to the left chest in respiratory distress. Chest XR shows a large hemopneumothorax, and you insert a large-bore chest tube. Do you give antibiotics?
Would love to hear the current practices around the trauma world on this topic. Are you giving antibiotics? If no, are you intrigued by these meta analyses? If not, what is your reservation? Thoughts, feedback, and discussion welcome.