
,
19 tweets,
5 min read
Read on Twitter
1: What causes triglyceride elevation in pleural fluid studies?
My previous understanding of this diagnostic test was recently challenged and lends credence to the fascinating diversity of pleural effusions/dz.
(A #MedTwitter and #Tweetorials contribution).
My previous understanding of this diagnostic test was recently challenged and lends credence to the fascinating diversity of pleural effusions/dz.
(A #MedTwitter and #Tweetorials contribution).
2: A middle aged woman OSH patient was transferred with LEFT pleural effusion that developed 5 days post-CABG.
Initial pleural fluid studies:
protein <0.8 LDH 2300 glucose 278 RBC 400 WBC 17.5k trigs 204 cholesterol 225 chylomicrons (-)
What type of effusion is this?
Initial pleural fluid studies:
protein <0.8 LDH 2300 glucose 278 RBC 400 WBC 17.5k trigs 204 cholesterol 225 chylomicrons (-)
What type of effusion is this?
3: This is not a case of hemothorax despite the presence of (many) RBCs. A true hemothorax diagnosis requires EITHER of the following:
1.Pleural fluid hematocrit (hct) >50% peripheral hematocrit
2.RBC/100,000 (estimate for pleural fluid hct if not obtained) >50% peripheral hct
1.Pleural fluid hematocrit (hct) >50% peripheral hematocrit
2.RBC/100,000 (estimate for pleural fluid hct if not obtained) >50% peripheral hct
4: An initial diagnosis of chylothorax was made due to elevated triglycerides >100. This was thought 2/2 thoracic duct (TD) injury during CABG 5 days prior. Left chest tube was placed, and chylothorax-directed management initiated. How do you treat a chylothorax?
TF = tube feeds
TF = tube feeds
5: Pt was started on low-fat diet and octreotide, w/ chest tube outputs remaining >200cc daily. OSH IR attempted TD embolization but unsuccessful at cannulating duct. Transferred to this hospital for further management.
Review of chylothorax management:
academic.oup.com/ejcts/article/…
Review of chylothorax management:
academic.oup.com/ejcts/article/…
6: In general, if chest tube output <500cc/day, conservative management is targeted. In this pt, low-fat TF’s and octreotide were continued following transfer. How does octreotide work in chylothorax management?
Circ = circulation
Absorb = absorption (from enterocytes)
Circ = circulation
Absorb = absorption (from enterocytes)
7: Octreotide is thought to work through combination of the above. Octreotide was previously shown to ⬇ lymph flow & trig enterocyte absorption in dogs (Nakabayashi 1981; PMID 6112179). It is also known to ⬇ splanchnic circ. and ⬇ GI motility (Kalomenidis 2006; PMID 16825878).
8: Upon our pt’s arrival from OSH, pleural fluid cx's grew E. coli, E. faecalis, Citrobacter, candida. How often do chylothoraces become infected?
9: Chylothoraces are typically NOT infected. Chyle is bacteriostatic, even when sitting at room temp for several weeks (Lampson 1948; PMID 18102742).
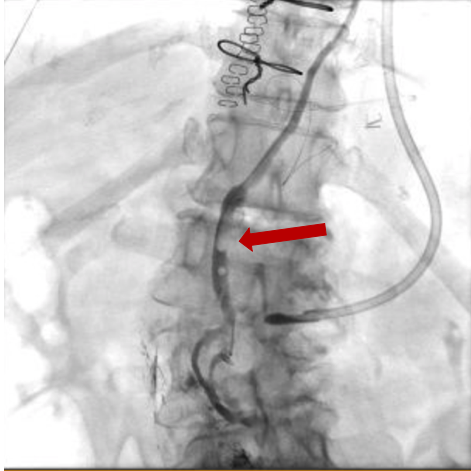
10: Despite conservative management, output remained >200cc/day. A second attempt at T ductogram showed partial obstruction of TD.
Why chylo if TD not obstructed? Review initial pleural fluid studies: triglycerides 204, chylomicrons (-)… is this truly consistent w/ chylothorax?
Why chylo if TD not obstructed? Review initial pleural fluid studies: triglycerides 204, chylomicrons (-)… is this truly consistent w/ chylothorax?
11: Chyle is mostly composed of chylomicrons (a form of triglycerides), which are large spherical proteins that transport large amounts of dietary fat absorbed by enterocytes to lymph. Chylomicrons must be elevated in a chylothorax.
12: Therefore, the definition of chylothorax is the following pleural fluid parameters:
Triglycerides >100 AND ⬆ chylomicrons (gold standard).
Triglycerides >100 AND ⬆ chylomicrons (gold standard).
13: To recap: this patient presented with elevated triglycerides but no chylomicrons in pleural fluid, only partial (not complete) obstruction of TD, and polymicrobial-positive pleural fluid cultures. What is the more likely diagnosis?
14: Subsequently, there became concern for esophageal perforation as complication from CABG (now ~1 month prior). Barium esophagram was then obtained and showed perforation of left distal esophagus with moderate extravasation of contrast into left lower hemithorax.

15: Pleural fluid characteristics consistent with esophageal perforation/rupture:
- ⬆ amylase
- ⬇ pH
- multiple pathogens on pleural fluid culture
- Triglycerides can be elevated in setting of esophageal perforation depending on PO intake
- ⬆ amylase
- ⬇ pH
- multiple pathogens on pleural fluid culture
- Triglycerides can be elevated in setting of esophageal perforation depending on PO intake
16: Anchoring caused delay in diagnosis during this interesting case. Triglyceride elevation (irrespective of chylomicron elevation) was used to entertain the diagnosis of chylothorax. Actual diagnosis was esophageal perforation during CABG.
Let’s go over a few learning points:
Let’s go over a few learning points:
17:
1/ The chylothorax diagnostic gold standard is elevated chylomicrons (trigs can be used as screen)
2/ Thoracic duct crosses (R-->L) at T4-T6 ➡ therefore chylothoraces are typically bilateral if thoracic duct injury above T5 or right-sided if injury below T5 (anatomy below):
1/ The chylothorax diagnostic gold standard is elevated chylomicrons (trigs can be used as screen)
2/ Thoracic duct crosses (R-->L) at T4-T6 ➡ therefore chylothoraces are typically bilateral if thoracic duct injury above T5 or right-sided if injury below T5 (anatomy below):

18:
3/ Low-fat TF’s + octreotide are often successful conservative management, but if chylous output >500cc daily, may require TD embolization/ligation
4/ Chylothoraces are RARELY infected and if multiple pathogens on pleural fluid culture -> suspect esophageal perforation
3/ Low-fat TF’s + octreotide are often successful conservative management, but if chylous output >500cc daily, may require TD embolization/ligation
4/ Chylothoraces are RARELY infected and if multiple pathogens on pleural fluid culture -> suspect esophageal perforation
19:
Thanks for reading! #FOAMed #MedEd
@thecurbsiders, @DoctorWatto: new episode idea -> pleural disease diagnosis/simple mgmt. Malignancy vs infection vs alternative. Fascinating diagnostics and management!
Thanks for reading! #FOAMed #MedEd
@thecurbsiders, @DoctorWatto: new episode idea -> pleural disease diagnosis/simple mgmt. Malignancy vs infection vs alternative. Fascinating diagnostics and management!








