1/16
Why does prerenal acute kidney injury lead to an elevated BUN/Cr ratio?
I always assumed the kidney increased urea reabsorption but never gave much thought as to where or how or why?
It's far more interesting than I'd expected...
Why does prerenal acute kidney injury lead to an elevated BUN/Cr ratio?
I always assumed the kidney increased urea reabsorption but never gave much thought as to where or how or why?
It's far more interesting than I'd expected...

2/
Let's start with a question.
Why would prerenal states lead the kidney to hold onto more urea? Put another way, what does the reabsorption of urea lead to?
[PCT = proximal convoluted tubule; CD = collecting duct]
Let's start with a question.
Why would prerenal states lead the kidney to hold onto more urea? Put another way, what does the reabsorption of urea lead to?
[PCT = proximal convoluted tubule; CD = collecting duct]
3/
In order to understand the answer, we'll need to review urea handling along the nephron. Let's start at the glomerulus.
(1) Glomerulus: urea is 100% filtered
(2) Proximal tubule: 50% reabsorbed (this results from a concentration gradient created by water reabsorption)
In order to understand the answer, we'll need to review urea handling along the nephron. Let's start at the glomerulus.
(1) Glomerulus: urea is 100% filtered
(2) Proximal tubule: 50% reabsorbed (this results from a concentration gradient created by water reabsorption)

4/
As urea enters the look of Henle, ~50% of the filtered load remains.
Next:
(3) Thin loops of Henle: Variable secretion (this results in a tubular concentration that is back to [or above] 100% of the filtered load)
(4) Inner medullary collecting duct: Variable reabsorption
As urea enters the look of Henle, ~50% of the filtered load remains.
Next:
(3) Thin loops of Henle: Variable secretion (this results in a tubular concentration that is back to [or above] 100% of the filtered load)
(4) Inner medullary collecting duct: Variable reabsorption

5/
Why does the kidney bother secreting and reabsorbing urea after the proximal tubule has done its work?
Recall: urea contributes ~50% of the osmolarity of the medullary interstitium.
And: a concentrated medullary interstitium is needed for maximal water reabsorption.
Why does the kidney bother secreting and reabsorbing urea after the proximal tubule has done its work?
Recall: urea contributes ~50% of the osmolarity of the medullary interstitium.
And: a concentrated medullary interstitium is needed for maximal water reabsorption.

6/
Here's the key: the urea that contributes to a concentrated medullary interstitium comes from its reabsorption in the collecting duct!
So, if the kidney is invested in reabsorbing more water, it should also be invested in reabsorbing urea from the collecting duct.
Here's the key: the urea that contributes to a concentrated medullary interstitium comes from its reabsorption in the collecting duct!
So, if the kidney is invested in reabsorbing more water, it should also be invested in reabsorbing urea from the collecting duct.
7/
This key point leads to a question:
Given urea's role in creating a concentrated urine, what molecule would you expect to increase its reabsorption in the collecting ducts?
This key point leads to a question:
Given urea's role in creating a concentrated urine, what molecule would you expect to increase its reabsorption in the collecting ducts?
8/
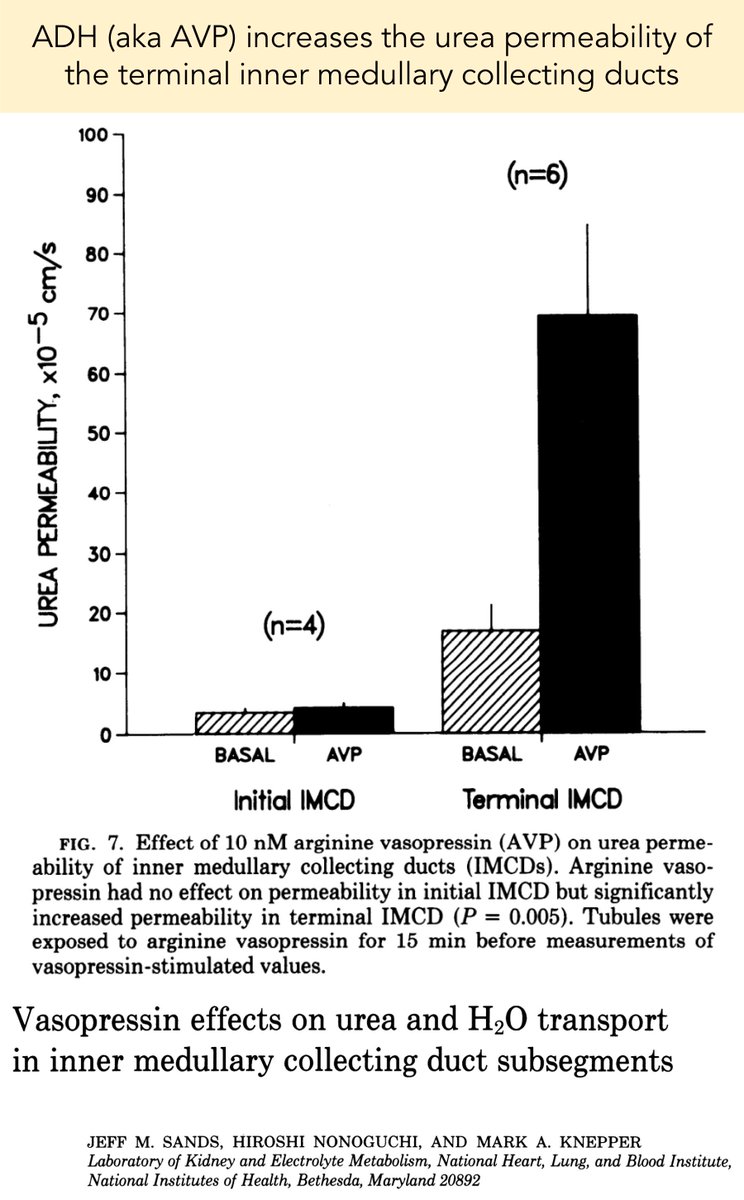
Urea reabsorption in the collecting ducts is under the control of antidiuretic hormone (ADH)!
More specifically, elevated ADH results in the placement of urea transporters (UT-A1 and A3) into the inner medullary collecting duct (see pic in tweet 5).
physiology.org/doi/abs/10.115…
Urea reabsorption in the collecting ducts is under the control of antidiuretic hormone (ADH)!
More specifically, elevated ADH results in the placement of urea transporters (UT-A1 and A3) into the inner medullary collecting duct (see pic in tweet 5).
physiology.org/doi/abs/10.115…
9/ Interim Summary
➢ Urea is reabsorbed, then secreted, then reabsorbed again
➢ Proximal reabsorption follows water reabsorption (not the reverse...)
➢ Distal reabsorption is under the control of ADH and is used to generate a concentrated medullary interstitium
➢ Urea is reabsorbed, then secreted, then reabsorbed again
➢ Proximal reabsorption follows water reabsorption (not the reverse...)
➢ Distal reabsorption is under the control of ADH and is used to generate a concentrated medullary interstitium
10/
Based on the above, which condition would you suspect has a low BUN/Cr ratio?
Based on the above, which condition would you suspect has a low BUN/Cr ratio?
11/
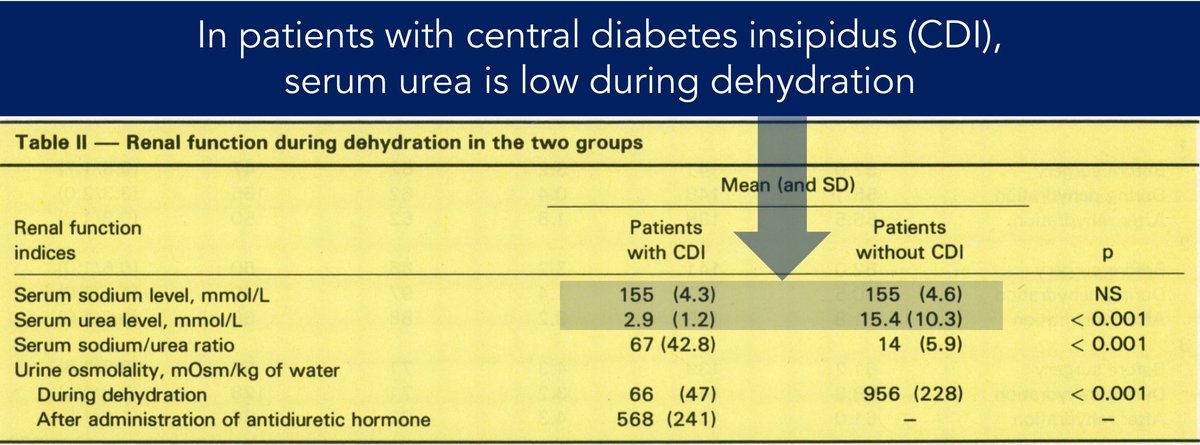
There are some cool studies showing that patients with central diabetes insipidus have a low BUN/Cr.
Without ADH, patients are unable to reabsorb urea in the collecting tubule.
Result: even when dehydrated, their urea is low.
ncbi.nlm.nih.gov/pubmed/3179869
There are some cool studies showing that patients with central diabetes insipidus have a low BUN/Cr.
Without ADH, patients are unable to reabsorb urea in the collecting tubule.
Result: even when dehydrated, their urea is low.
ncbi.nlm.nih.gov/pubmed/3179869
12/
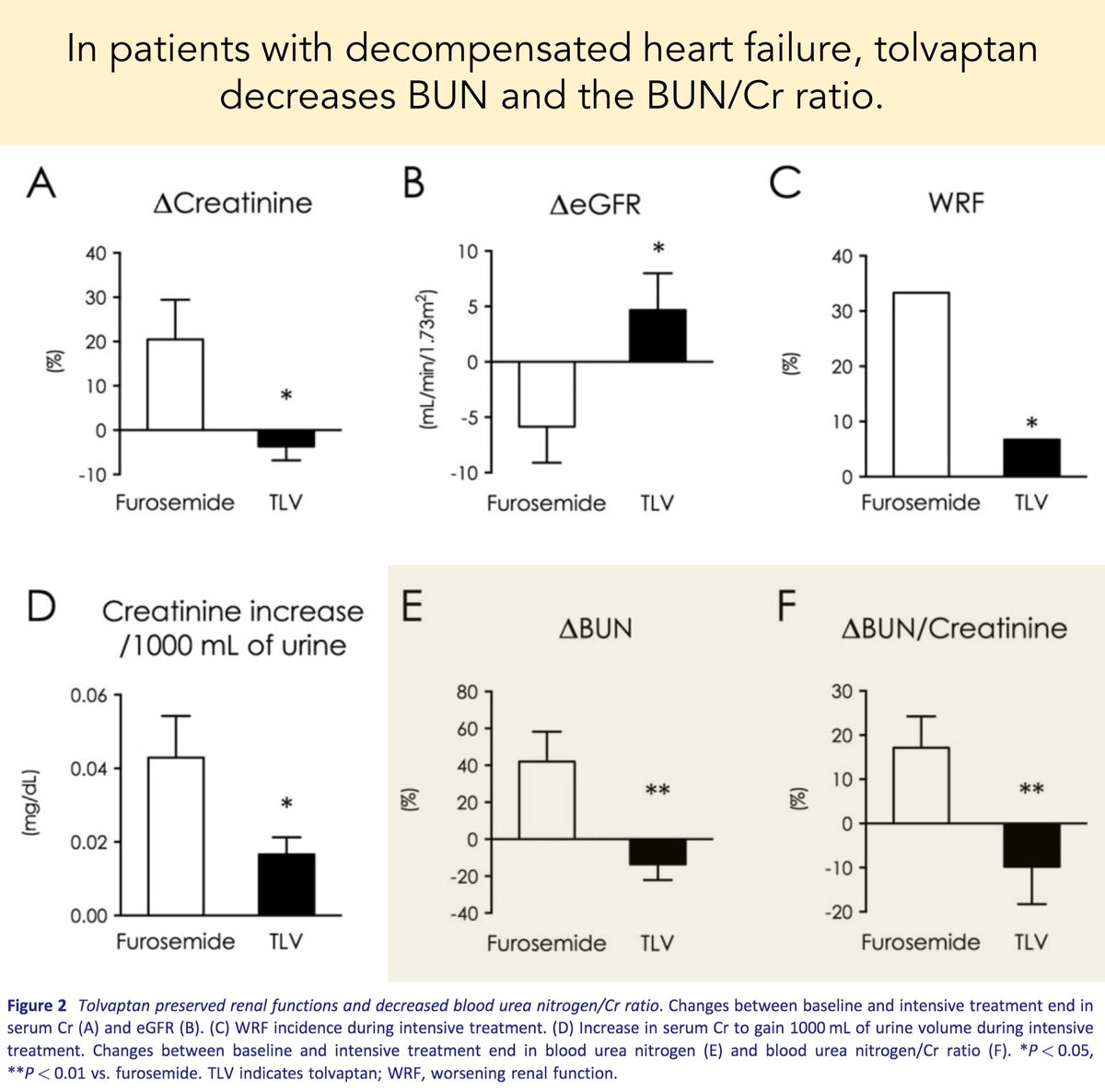
Another interesting observation: in patients with heart failure who receive tolvaptan, the BUN/Cr decreases.
Again, blocking the effects of ADH leads to an inability to reabsorb urea in the collecting ducts.
onlinelibrary.wiley.com/doi/full/10.10…
Another interesting observation: in patients with heart failure who receive tolvaptan, the BUN/Cr decreases.
Again, blocking the effects of ADH leads to an inability to reabsorb urea in the collecting ducts.
onlinelibrary.wiley.com/doi/full/10.10…
13/
Based on the physiology described above, there are two possible sites of increased urea reabsorption that would lead to elevated BUN/Cr in prerenal acute kidney injury?
Which do you think is the more important site?
Based on the physiology described above, there are two possible sites of increased urea reabsorption that would lead to elevated BUN/Cr in prerenal acute kidney injury?
Which do you think is the more important site?
14/
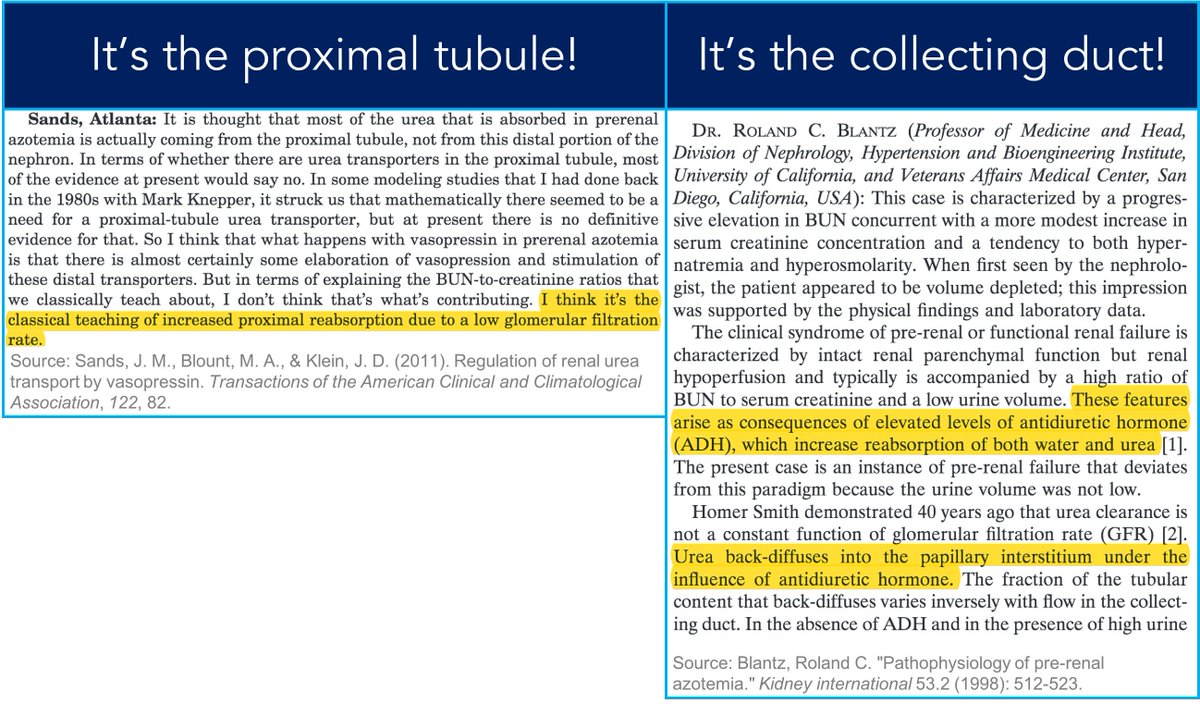
I haven't been able to find a conclusive study showing that either the proximal tubule or the collecting duct is THE site of increased reabsorption that leads to an elevated BUN/Cr.
Some argue for PT: ncbi.nlm.nih.gov/pmc/articles/P…
Others argue for the CD: kidney-international.org/article/S0085-…
I haven't been able to find a conclusive study showing that either the proximal tubule or the collecting duct is THE site of increased reabsorption that leads to an elevated BUN/Cr.
Some argue for PT: ncbi.nlm.nih.gov/pmc/articles/P…
Others argue for the CD: kidney-international.org/article/S0085-…
15/
Before closing, let's re-ask our original question.
Why would prerenal states lead the kidney to hold onto more urea? Put another way, what does the reabsorption of urea lead to?
[PCT = proximal convoluted tubule; CD = collecting duct]
Before closing, let's re-ask our original question.
Why would prerenal states lead the kidney to hold onto more urea? Put another way, what does the reabsorption of urea lead to?
[PCT = proximal convoluted tubule; CD = collecting duct]
16/16
💥Why does prerenal AKI lead to an elevated BUN/Cr ratio?💥
➢ Urea is reabsorbed in the proximal tubule and collecting duct (CD)
➢ ADH controls CD reabsorption and allows for urine concentration
➢ Prerenal AKI may lead to ↑ADH ➔ ↑CD urea reabsorption ➔ ↑BUN/Cr
💥Why does prerenal AKI lead to an elevated BUN/Cr ratio?💥
➢ Urea is reabsorbed in the proximal tubule and collecting duct (CD)
➢ ADH controls CD reabsorption and allows for urine concentration
➢ Prerenal AKI may lead to ↑ADH ➔ ↑CD urea reabsorption ➔ ↑BUN/Cr