Another day on service and you are starting with answering a page from PACU. "Hi this is nephrology fellow returning your page". "Great! This is Ortho, and our patient post op has low potassium here; I believe you call it HYPOkalemia" #Loveourorthopods #Tweetorial #medthread 
Join us for our electrolyte abnormality du jour and learn how to break it down! #nephtwitter #medtwitter #FOAMED See our full post @RenalFellowNtwk > renalfellow.org/2019/11/14/the…
59 yo F with a hx of HTN, and HLP admitted for a left femur fracture; she was found down by her neighbor 3 days after her fall; awake and in pain. Now, patient is post op; and on labs: (baseline cr: 0.51). UA unremarkable.

On PE, patient is cachectic and ill appearing, s/p ORIF on LLE. Labs interpretation: We believe she has an AKI (low muscle mass, cr rise from b/l by 0.3 mg/dl). In order to further work up hypokalemia; we asked for urine lytes.

You're dealing with an unexplained HYPOkalemia, at this point what do you calculate?
Well, you don't want to calculate TTKG since this paper came out in 2011! ncbi.nlm.nih.gov/pubmed/21788894
FeK: #knowlimitations: Fraction excretion means calculating the percentage of filtered K ending up in the urine. All the filtered K gets reabsorbed in the proximal tubule and loop of henle. K gets secreted into the urine in DCT and MCD. SO, Fek does not sound perfect either!
Urine potassium-to-creatinine ratio (K/Cr): This is more reliable. Normal range <1.5 mmol/mmol (13 mEq/g). So, I would check urine K/urine Cr in this setting.
No evidence of renal losses of K and no hx of intestinal losses. Patient mentions very poor oral intake for the past couple of months. Patient received oral potassium repletion and was started on a regular diet and IVF LR at 50 cc/hr. After 8 hours; repeat labs are as follows:
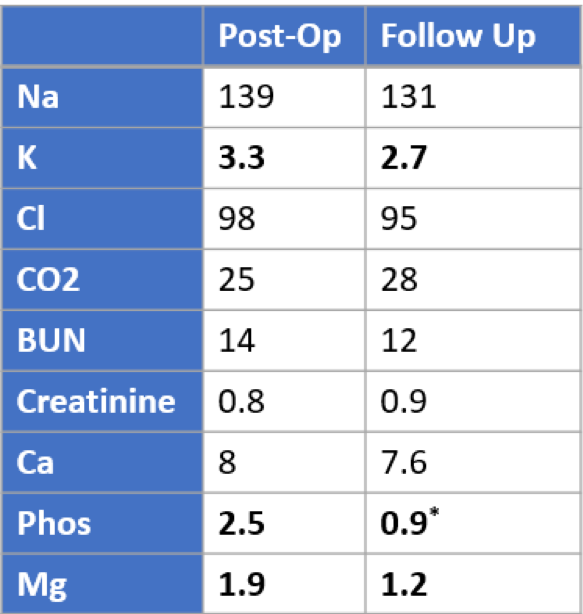
What is going on here? Hypokalemia got worse despite receiving K repletion and starting a diet. Wait phos, mag, are dropping as well? Are we dealing with refeeding syndrome (RFS)?
History check: RFS was first described in prisoners of war after the second world war when they started eating after a long time.
Does our patient have risk factors for developing RFS? √ Cachectic elderly patient with hx of prolonged low energy diet and then high stress unfed for at least 4 days Let’s see how RFS happens.
Prolonged fasting > Initial muscle breakdown followed by preservation of muscle protein by, ↓ Liver gluconeogenesis + ↑ Ketogenesis > ketonemia > stimulating brain and tissues to use ketones as main energy source #physiology
What happens to electrolytes during prolonged fasting? Intracellularly depleted as shifting happens; however, serum concentrations can remain normal for two reasons: shifting from ICF and decrease in kidney excretion.
Malnourished patient starts eating> ↑ insulin and ↓ glucagon secretion > glycogen, fat and protein synthesis stimulated + Intracellular shifting of K (via NA/K ATPase), Mg & phos > ↓↓ serum levels (K, Mg & phos)
Hypophosphatemia is the hallmark of RFS. Phosphorus is needed to generate adenosine triphosphate from adenosine diphosphate and adenosine monophosphate
How to manage RFS? See NICE guidelines>

Summary: • RFS is preventable in the setting of early detection and management • Identify high risk patients; check K, Ca, P, & Mg • Serum electrolyte levels may be normal prior to refeeding; BEWARE! Total body and intracellular depletion have occurred.
Thank you! Let us know what you think. Special thanks to @kidney_boy @TheSkeletonKG.