1/13
How does the subcutaneous (SC) insulin work?
Given that the oral delivery of insulin is difficult, SC injection is the mainstay. I always found this mystifying. What happens to insulin after its injected? Why isn’t it all just dumped into the blood?
Let's have a look!
How does the subcutaneous (SC) insulin work?
Given that the oral delivery of insulin is difficult, SC injection is the mainstay. I always found this mystifying. What happens to insulin after its injected? Why isn’t it all just dumped into the blood?
Let's have a look!
2/
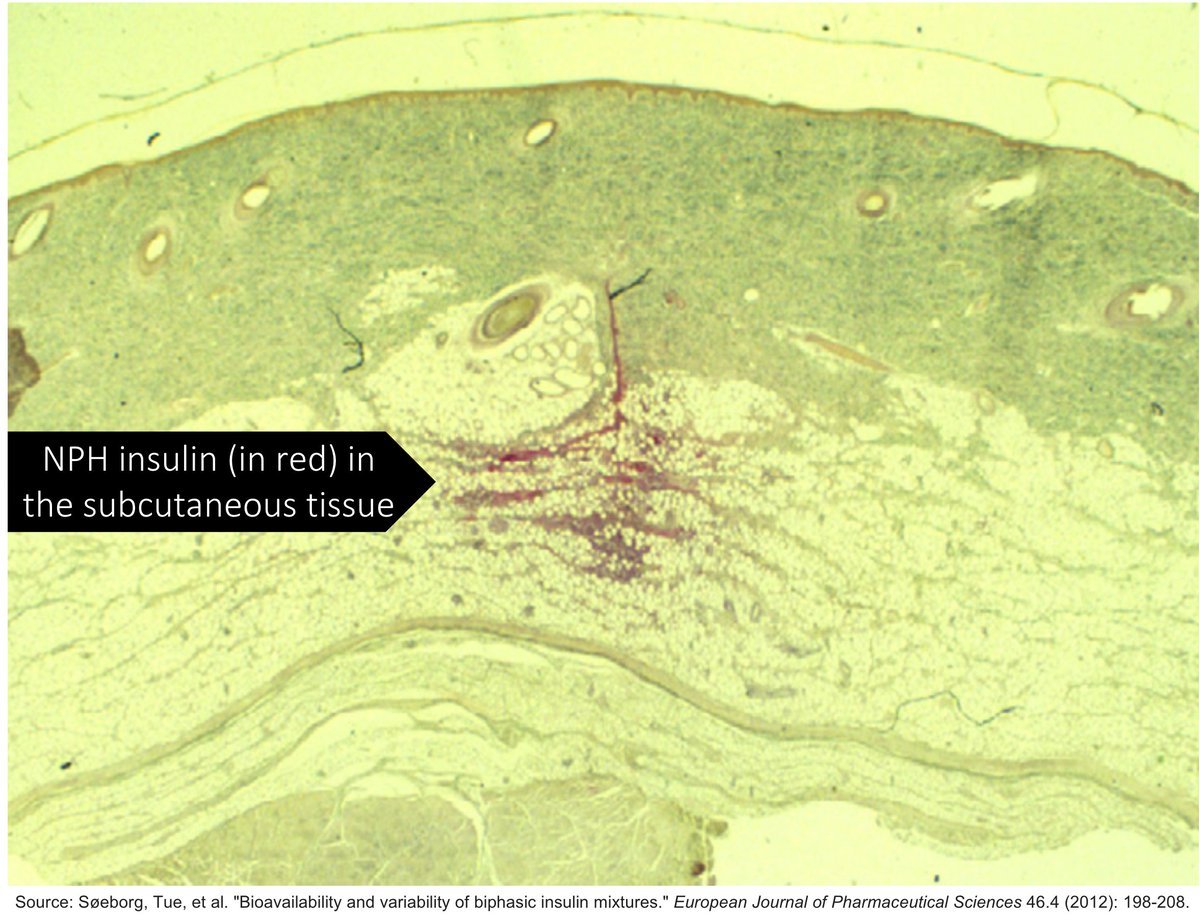
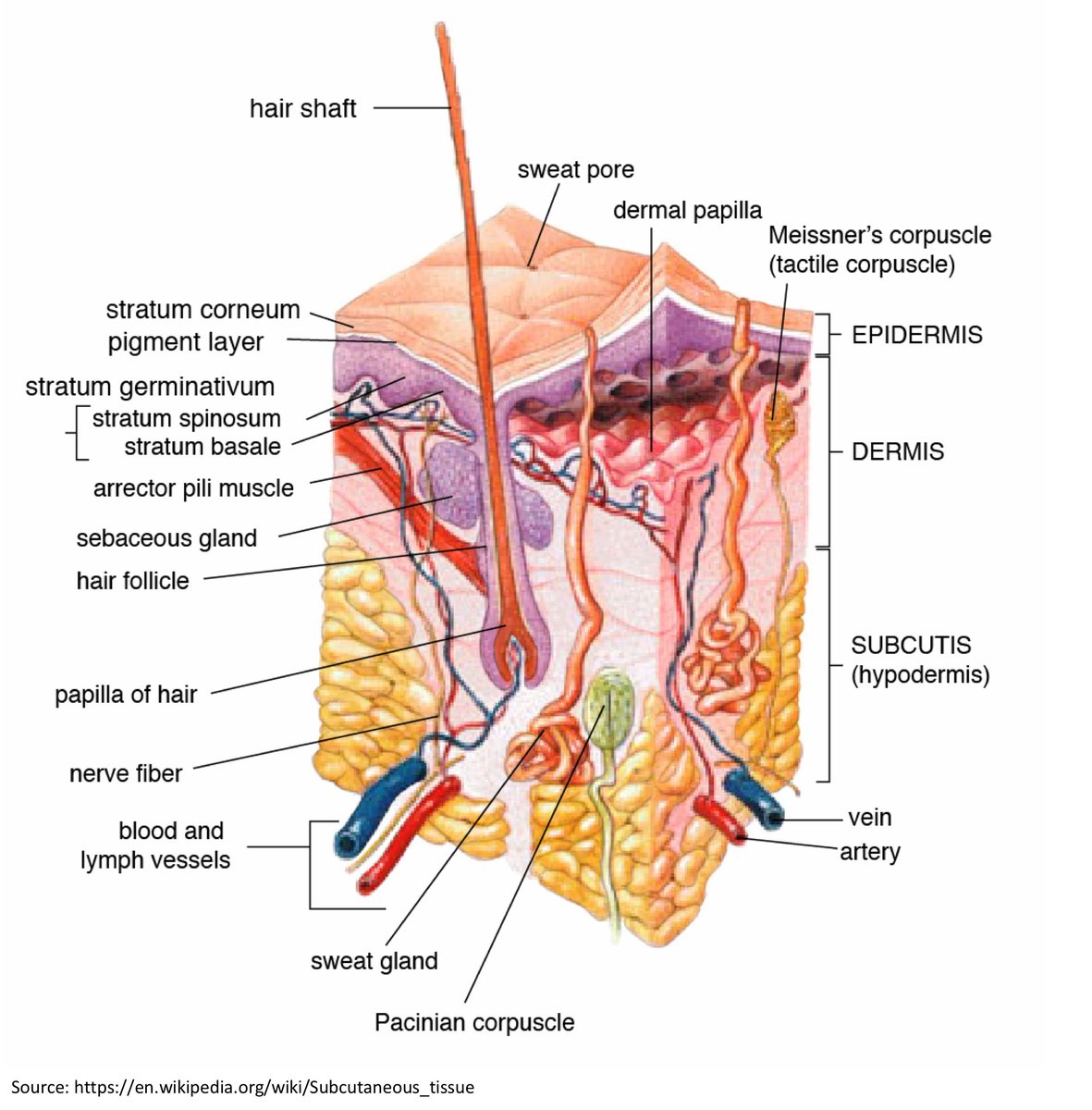
As a reminder, the SC tissue (i.e., hypodermis) is:
90% fat cells
10% extracellular matrix (ECM)
It is the ECM is the barrier through which insulin must navigate through to gain access to the blood via capillaries.
ncbi.nlm.nih.gov/pubmed/30116732
As a reminder, the SC tissue (i.e., hypodermis) is:
90% fat cells
10% extracellular matrix (ECM)
It is the ECM is the barrier through which insulin must navigate through to gain access to the blood via capillaries.
ncbi.nlm.nih.gov/pubmed/30116732
3/
Molecules <16 kDa can diffuse from the SC tissue into capillaries. Larger molecules must use the lymphatics.
Recall that insulin is 5.8 kDa so it can access this capillary route.
ncbi.nlm.nih.gov/pubmed/22619041
Molecules <16 kDa can diffuse from the SC tissue into capillaries. Larger molecules must use the lymphatics.
Recall that insulin is 5.8 kDa so it can access this capillary route.
ncbi.nlm.nih.gov/pubmed/22619041
4/
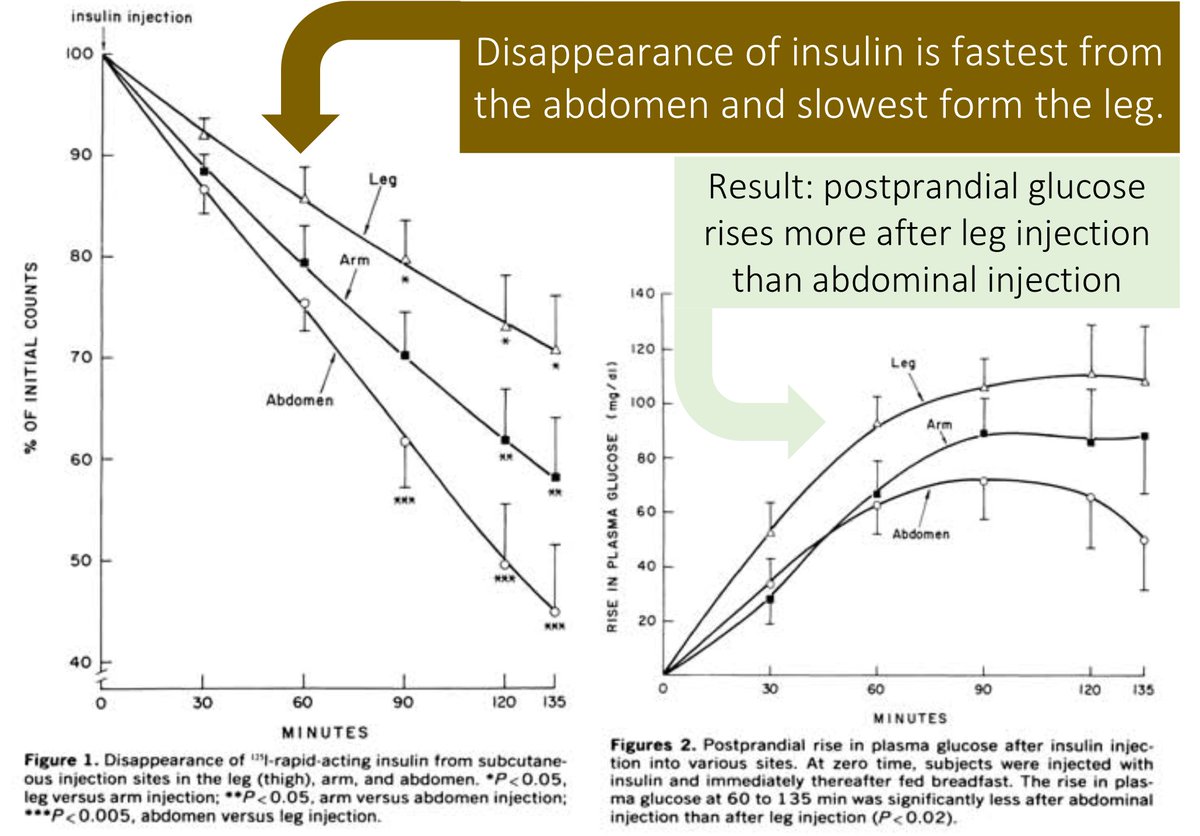
Blood flow to the SC tissue is a factor determining the capillary absorption of insulin.
Given that thighs have fewer capillary loops than the abdomen, absorption is slower when insulin is injected into the leg.
ncbi.nlm.nih.gov/pubmed/6444267
Blood flow to the SC tissue is a factor determining the capillary absorption of insulin.
Given that thighs have fewer capillary loops than the abdomen, absorption is slower when insulin is injected into the leg.
ncbi.nlm.nih.gov/pubmed/6444267
5/
If blood flow to the SC tissue is a factor determining the capillary absorption, what else might increase the absorption of insulin?
If blood flow to the SC tissue is a factor determining the capillary absorption, what else might increase the absorption of insulin?
6/
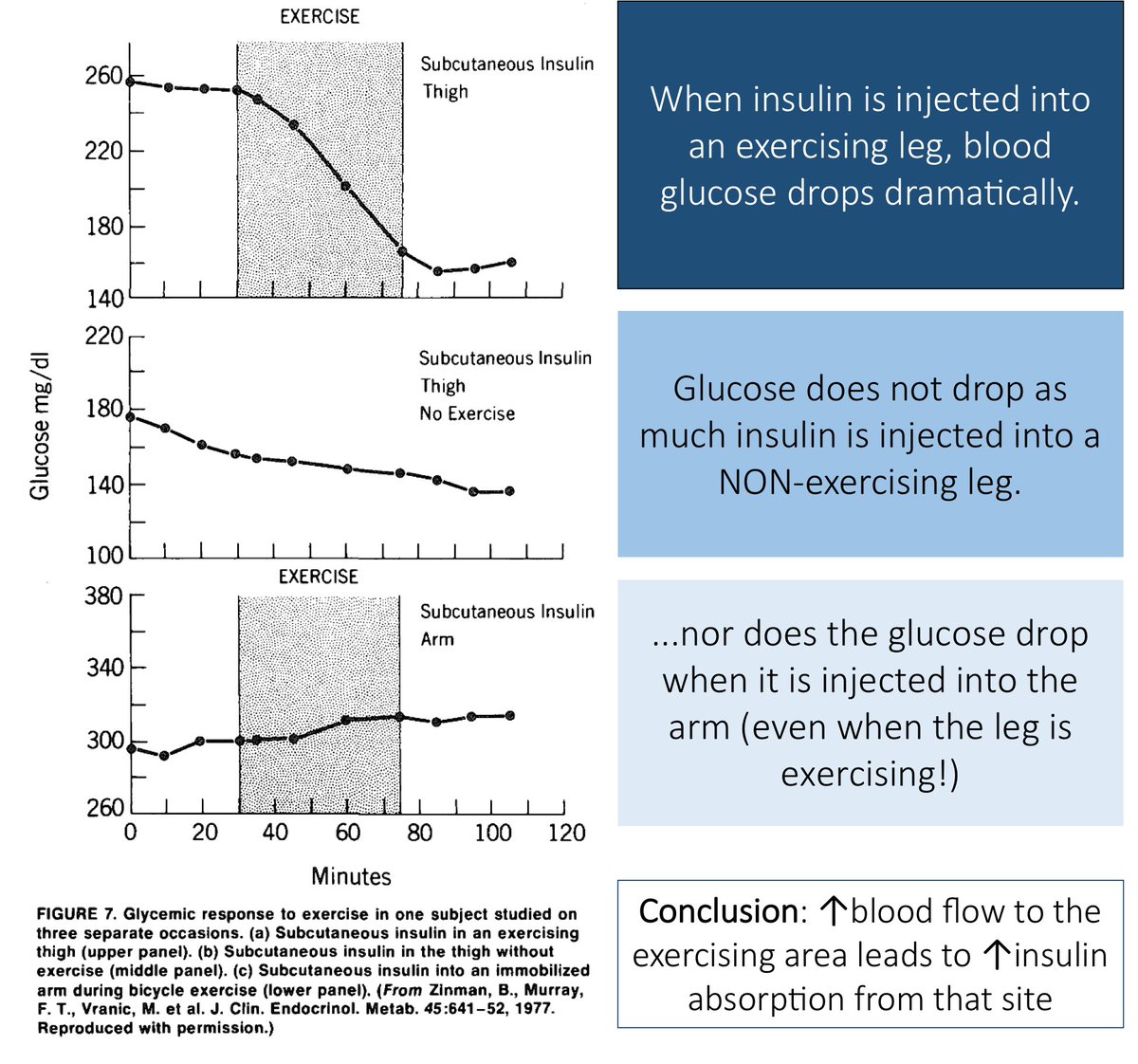
Anything that increases capillary blood flow might be expected to increase the absorption of insulin. Things like:
• Heat
• Exercise
• Massage
ncbi.nlm.nih.gov/pubmed/761718
ncbi.nlm.nih.gov/pubmed/6376015
Anything that increases capillary blood flow might be expected to increase the absorption of insulin. Things like:
• Heat
• Exercise
• Massage
ncbi.nlm.nih.gov/pubmed/761718
ncbi.nlm.nih.gov/pubmed/6376015
7/
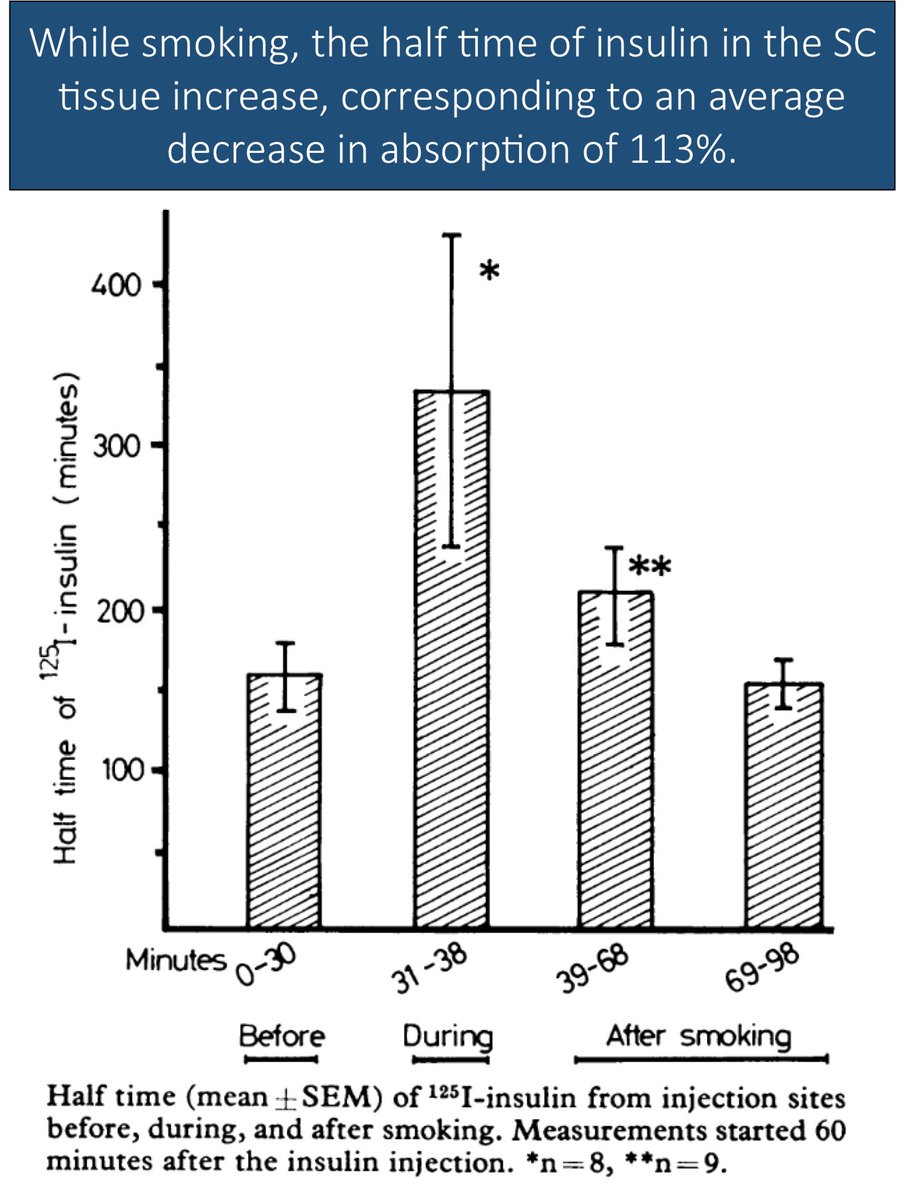
Smoking leads to vasoconstriction. This means that smoking can cause a DECREASE in insulin absorption from the SC tissue into the capillary blood.
ncbi.nlm.nih.gov/pubmed/6799119
Smoking leads to vasoconstriction. This means that smoking can cause a DECREASE in insulin absorption from the SC tissue into the capillary blood.
ncbi.nlm.nih.gov/pubmed/6799119
8/
So, insulin diffuses from the ECM of the SC space to the capillaries to gain access to blood.
Once insulin enters the blood, its half-life is <10 minutes.
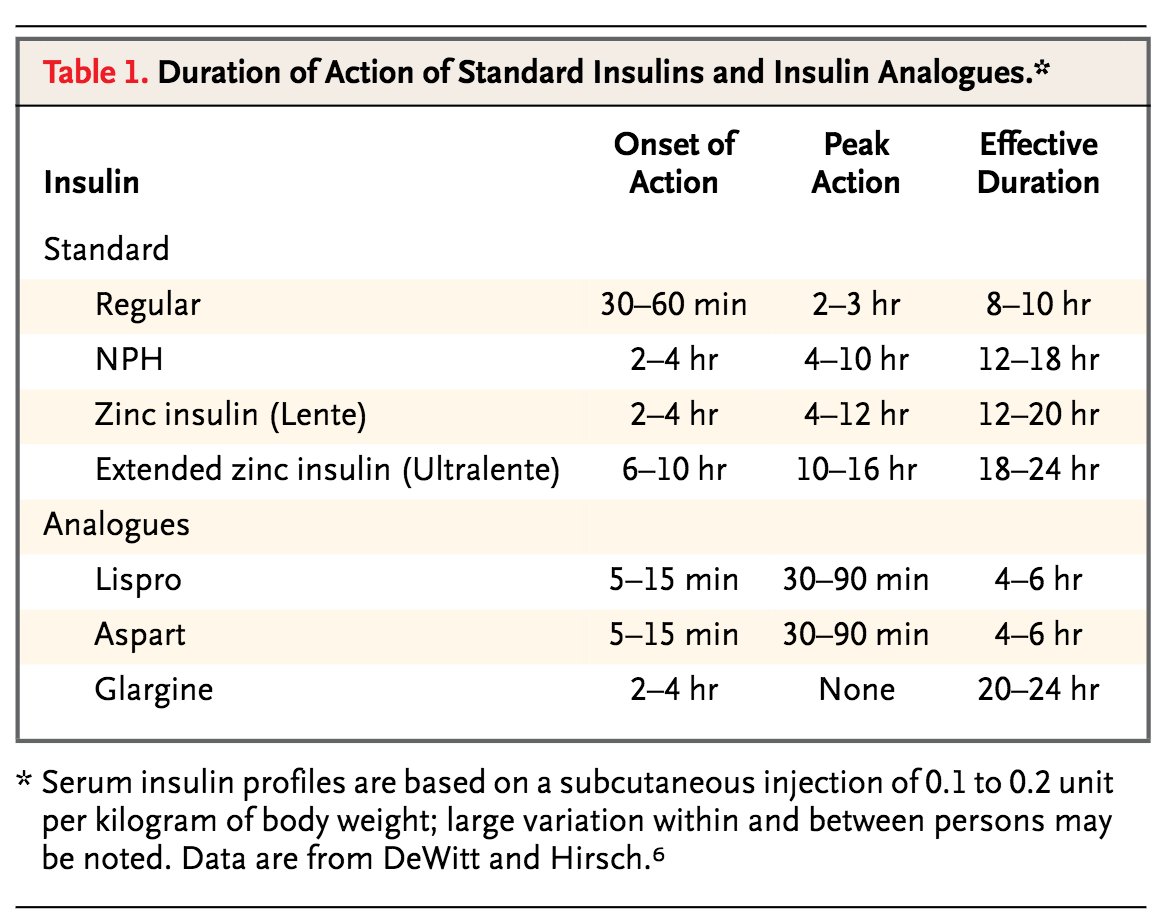
Why then do insulin types have markedly different onsets of action and durations of effect? Let's address this next.
So, insulin diffuses from the ECM of the SC space to the capillaries to gain access to blood.
Once insulin enters the blood, its half-life is <10 minutes.
Why then do insulin types have markedly different onsets of action and durations of effect? Let's address this next.
9/
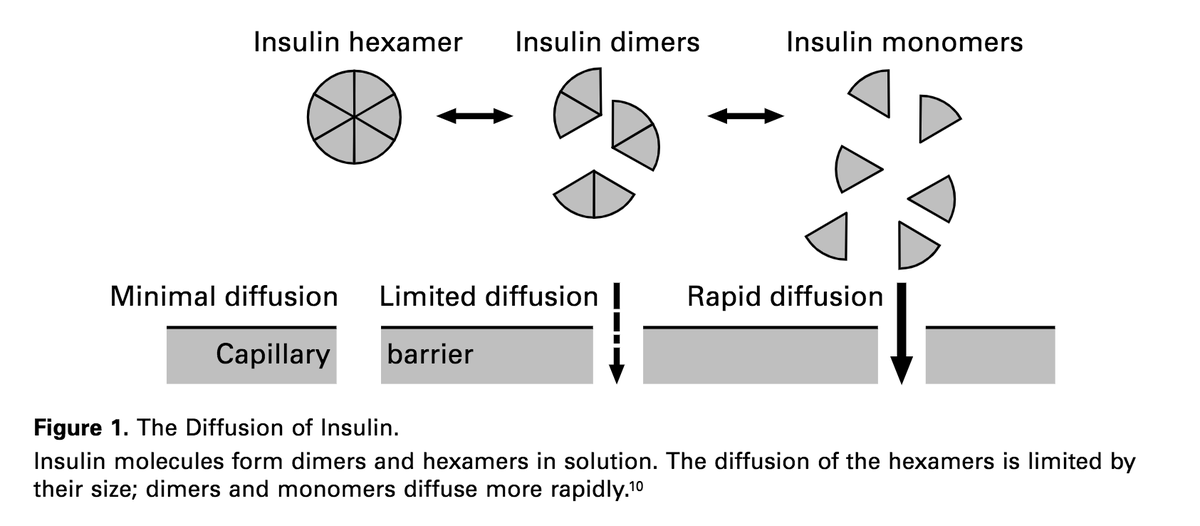
To understand how this is possible, it is important to know that insulin consists of different oligomers, including monomers, dimers, and hexamers.
Monomers diffuse into capillaries more easily than hexamers.
ncbi.nlm.nih.gov/pubmed/9219705
To understand how this is possible, it is important to know that insulin consists of different oligomers, including monomers, dimers, and hexamers.
Monomers diffuse into capillaries more easily than hexamers.
ncbi.nlm.nih.gov/pubmed/9219705
10/
Adding protamine or zinc causes insulin to form hexamers. Hexamers do not diffuse well and therefore have slower onsets of action.
Two examples:
• NPH (i.e., Neutral PROTAMINE Hagedorn)
• Regular insulin (contains zinc atoms)
ncbi.nlm.nih.gov/pubmed/15647580
Adding protamine or zinc causes insulin to form hexamers. Hexamers do not diffuse well and therefore have slower onsets of action.
Two examples:
• NPH (i.e., Neutral PROTAMINE Hagedorn)
• Regular insulin (contains zinc atoms)
ncbi.nlm.nih.gov/pubmed/15647580
11/
Rapid-acting insulins (e.g., lispro) dissociate into monomers more quickly. These smaller monomers are then able to enter capillaries faster than dimers or hexamers.
Result: quicker onset of action and shorter effective duration of action.
Rapid-acting insulins (e.g., lispro) dissociate into monomers more quickly. These smaller monomers are then able to enter capillaries faster than dimers or hexamers.
Result: quicker onset of action and shorter effective duration of action.
12/
There are other factors involved beyond what's covered in this thread.
These articles provide very nice reviews.
ncbi.nlm.nih.gov/pubmed/30116732
ncbi.nlm.nih.gov/pubmed/22619041
There are other factors involved beyond what's covered in this thread.
These articles provide very nice reviews.
ncbi.nlm.nih.gov/pubmed/30116732
ncbi.nlm.nih.gov/pubmed/22619041
13/13 [SUMMARY]
💥How does the subcutaneous (SC) insulin work?💥
➣ Insulin diffuses from SC tissue into capillaries
➣ ↑capillary blood flow (e.g., exercise) leads to ↑absorption
➣ Monomers diffuse more quickly than hexamers. This is relevant for short/long-acting insulins
💥How does the subcutaneous (SC) insulin work?💥
➣ Insulin diffuses from SC tissue into capillaries
➣ ↑capillary blood flow (e.g., exercise) leads to ↑absorption
➣ Monomers diffuse more quickly than hexamers. This is relevant for short/long-acting insulins
If you want to read more about insulin, here's my other tweetorial on the topic.