1/ I'm very worried that we don't have a clear strategy for #COVID19 response
We need to clearly define when the public health goal is containment-trying to keep the virus from circulating- and when the goal shifts to mitigation-working to reduce the peak impact of the outbreak
We need to clearly define when the public health goal is containment-trying to keep the virus from circulating- and when the goal shifts to mitigation-working to reduce the peak impact of the outbreak
2/ Let me first voice my tremendous respect for the public health experts at the @CDCgov & state/local governments
I'm proud to have worked as a CDC Epidemic Intelligence Service Officer, and I never had smarter, harder working colleagues than during my 12 yrs at @nycHealthy
I'm proud to have worked as a CDC Epidemic Intelligence Service Officer, and I never had smarter, harder working colleagues than during my 12 yrs at @nycHealthy
3/ Let me next acknowledge that it has been over 10 years since I was involved in an epidemiological/outbreak investigation or surveillance
What I'm going to describe is informed by my past experience and conversations w experts, but I am not an expert in #COVID19
What I'm going to describe is informed by my past experience and conversations w experts, but I am not an expert in #COVID19
4/ Here's the nub of my worry.
We are treating the outbreak in the US as if we are in containment mode- case identification, contact tracing, quarantine and active monitoring of exposed individuals
But I fear that in many locales there is already sustained community spread
We are treating the outbreak in the US as if we are in containment mode- case identification, contact tracing, quarantine and active monitoring of exposed individuals
But I fear that in many locales there is already sustained community spread
5/ New cases are being identified every day that do not have a travel history or connection to a known case
*and we know that these are just the tip of the iceberg* because of the delays in testing
That means that in the next two weeks the number of diagnosed cases will explode
*and we know that these are just the tip of the iceberg* because of the delays in testing
That means that in the next two weeks the number of diagnosed cases will explode
6/ Trying to do containment when there is exponential community spread is like focusing on putting out sparks when the house is on fire.
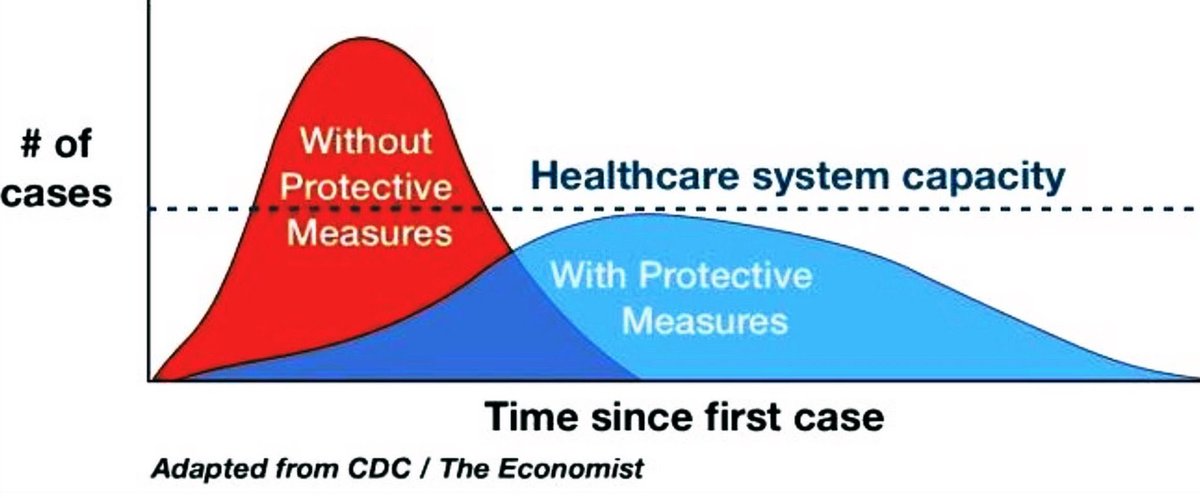
when that happens, we need to switch strategies to mitigation- taking protective measures to slow spread & reduce peak impact on healthcare
when that happens, we need to switch strategies to mitigation- taking protective measures to slow spread & reduce peak impact on healthcare
7/ Exhausting our public health workforce with contact tracing, asymptomatic testing and active monitoring when the cat is out of the bag is not just wasteful, it actively undermines our ability to mount an effective response to an outbreak that is just beginning to explode.
8/ And continuing to pursue a failed containment strategy can also delay making the hard decisions involved in mitigation.
Closing schools
Cancelling events.
Telling people to stay home.
I see no guidance as to which localities are at this stage, and what they should do.
Closing schools
Cancelling events.
Telling people to stay home.
I see no guidance as to which localities are at this stage, and what they should do.
9/ I can't tell you how many people have asked me if they should travel to certain cities- we are left to our own devices to figure out where there is sustained community transmission. I can find no official webpage that updates this key status for the US.
@CDCgov must do better
@CDCgov must do better
10/ Most alarming, I don't see any public-facing transparency on whether #COVID19 has resulted in noticeable increases in people going to the emergency room, or being hospitalized
And here's the thing-we invested hundreds of millions of dollars to develop exactly this capability
And here's the thing-we invested hundreds of millions of dollars to develop exactly this capability
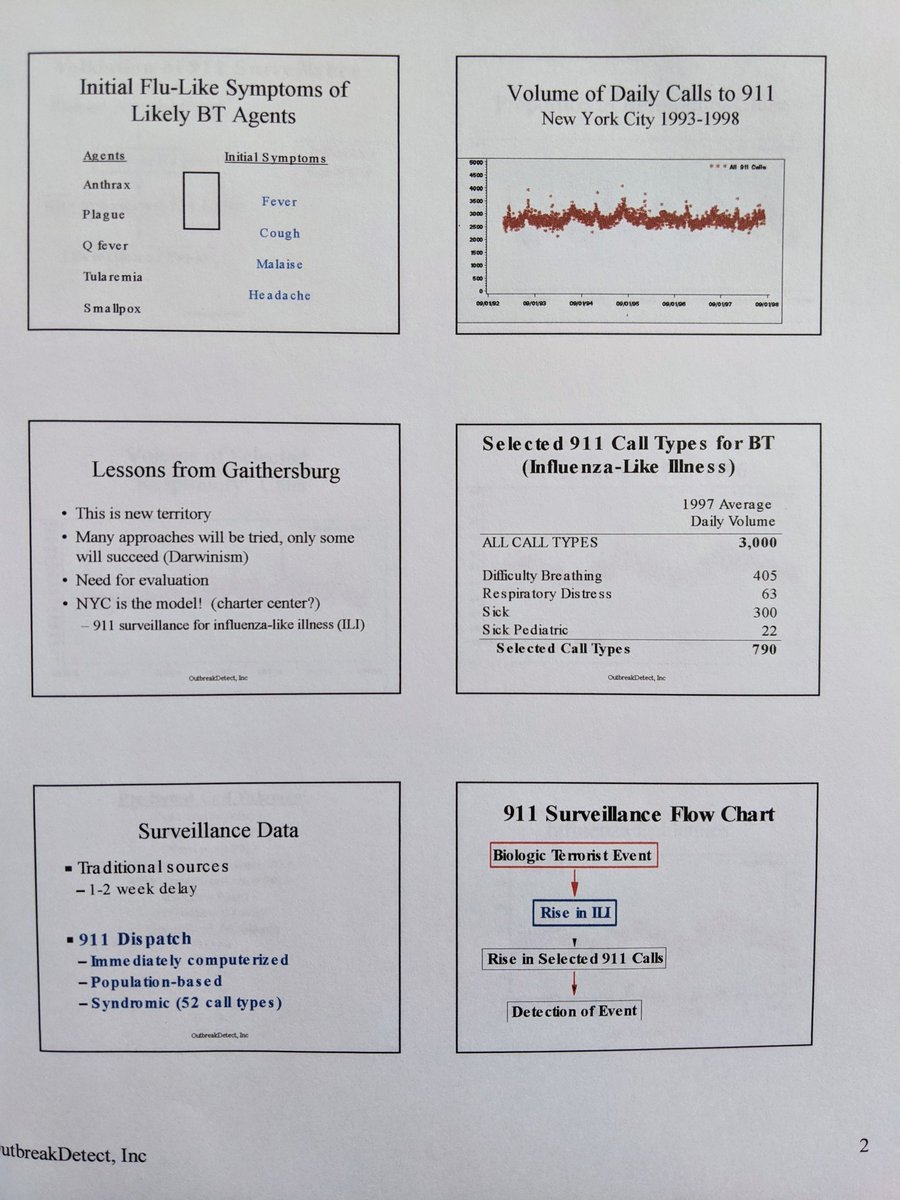
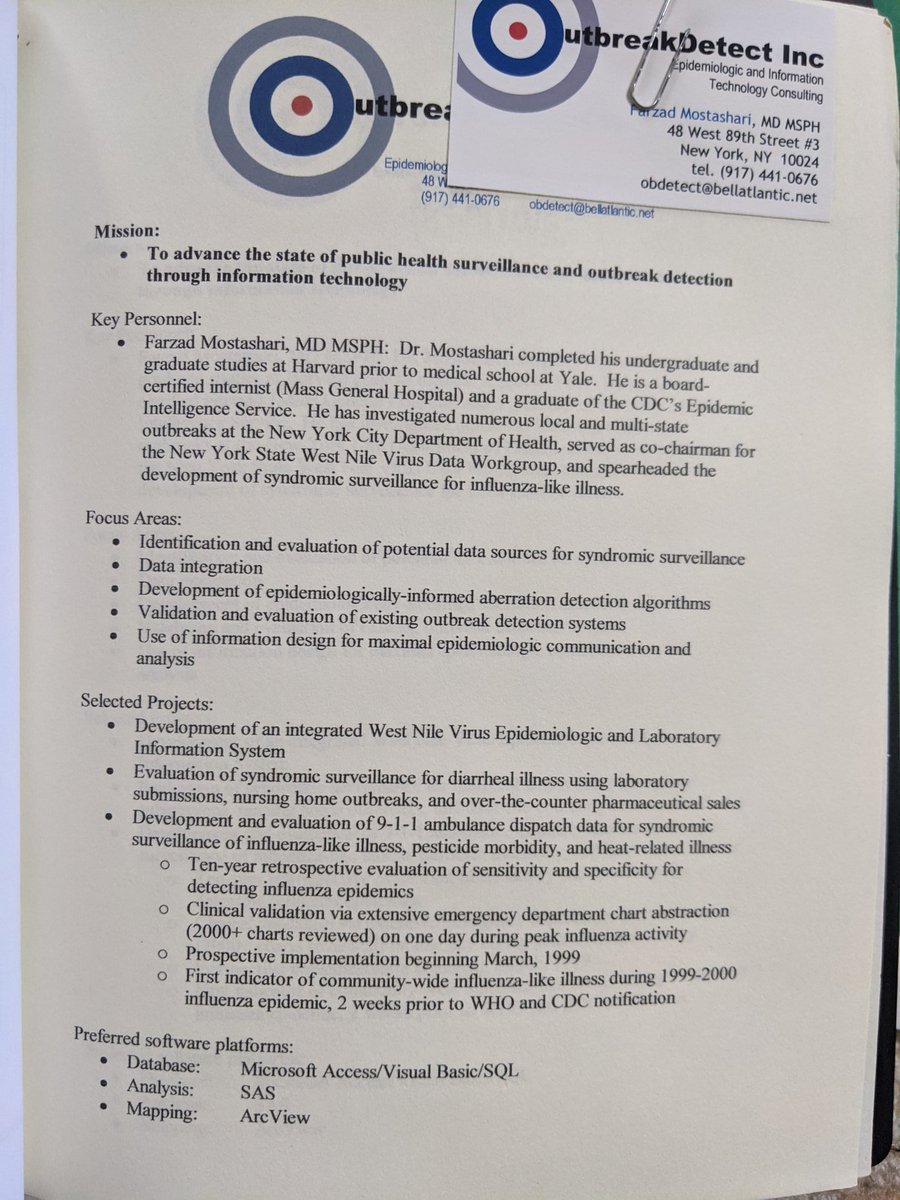
11/ On this, I am an expert.
After 9/11, I was part of a group of what would now be called Data Scientists who pioneered "syndromic surveillance"- monitoring things like emergency department registration data for real-time public health surveillance
academic.oup.com/jamia/article/…
After 9/11, I was part of a group of what would now be called Data Scientists who pioneered "syndromic surveillance"- monitoring things like emergency department registration data for real-time public health surveillance
academic.oup.com/jamia/article/…
12/ We established data feeds to all sorts of ongoing data, adapted statistical methods, developed standards, and privacy frameworks, and put these types of surveillance programs into practice across the country.
I was in one of the leading centers, NYC
wwwnc.cdc.gov/eid/article/10…
I was in one of the leading centers, NYC
wwwnc.cdc.gov/eid/article/10…
13/ When I joined feds @ONC_HealthIT to roll out EHRs, we included sending data to public health, including syndromic surveillance, as elements of "meaningful use" for hospitals
Over 70% of hospitals in the US are sending realtime data to public health now
cdc.gov/nssp/index.html
Over 70% of hospitals in the US are sending realtime data to public health now
cdc.gov/nssp/index.html
14/ This what it looks like- daily rates of influenza like illness presenting to emergency departments in NYC, as of last week-
reassuringly, you can see the peak of influenza activity rising each year, and subsiding.
reassuringly, you can see the peak of influenza activity rising each year, and subsiding.
15/ This is what the ILI data in NYC looks like now.
It looks like there is a clear signal now of increasing influenza-like illness (cough and fever) in NYC
I don't know if this is "worried well" or a resurgence of flu, or what the age distribution is, but those are answerable
It looks like there is a clear signal now of increasing influenza-like illness (cough and fever) in NYC
I don't know if this is "worried well" or a resurgence of flu, or what the age distribution is, but those are answerable

16/ And the only reason I'm using NYC as an example here is that we made the decision to make this data publicly available on the web
I don't know if federal authorities are tightly monitoring fever/cough ER visit trends across the country and investigating if #COVID19 I hope so
I don't know if federal authorities are tightly monitoring fever/cough ER visit trends across the country and investigating if #COVID19 I hope so
17/ If we are already seeing a detectable increase in symptomatic ER visits due to COVID19, at this stage of the outbreak, should we expect 20x that burden of illness in 4 weeks if doubling time is 6 days?
We need to be working URGENTLY on expanding/protecting healthcare capacity
We need to be working URGENTLY on expanding/protecting healthcare capacity
18/ ...and you know what doesn't help?
An "abundance of caution" in CDC guidance to impose airborne precautions/N95 masks (as for TB) vs droplet precautions (as in flu)
we don't have enough N95 masks.
cdc.gov/infectioncontr…
An "abundance of caution" in CDC guidance to impose airborne precautions/N95 masks (as for TB) vs droplet precautions (as in flu)
we don't have enough N95 masks.
cdc.gov/infectioncontr…
19/ And if a healthcare worker is "exposed" (because they weren't wearing an N95 mask they probably don't need) to a patient who later tests positive for coronavirus, should they then be taken out of circulation, quarantined for 14 days?
What does that do to healthcare capacity?
What does that do to healthcare capacity?
20/ And you know what doesn't help?
Pushing testing of asymptomatic contacts or mild cases (no-copay, "if you want a test you can get it") after you already have widespread community transmission
That further exposes other patients and healthcare workers, and saps resources
Pushing testing of asymptomatic contacts or mild cases (no-copay, "if you want a test you can get it") after you already have widespread community transmission
That further exposes other patients and healthcare workers, and saps resources
21/ we need a strategy
like this:
1) Severe Acute Respiratory Illness (SARI) surveillance, Active case finding, contact tracing, quarantine.... UNTIL we have evidence of sustained community transmission (multiple community-acquired cases, validated non-flu ED ILI signal)
THEN
like this:
1) Severe Acute Respiratory Illness (SARI) surveillance, Active case finding, contact tracing, quarantine.... UNTIL we have evidence of sustained community transmission (multiple community-acquired cases, validated non-flu ED ILI signal)
THEN
22/ Then switch to containment. Let everyone know when you make the switch and why
Stop routine testing in mild/asymptomatic
Stop contact tracing
Cancel mass gatherings
we urgently need to find out if children are infectious, not just infected, and whether school closures work
Stop routine testing in mild/asymptomatic
Stop contact tracing
Cancel mass gatherings
we urgently need to find out if children are infectious, not just infected, and whether school closures work
23/ needless to say, all the positive steps that people are taking on changing our habits are good at every stage and may be bringing down the reproductive rate
not shaking hands
washing hands, using hand sanitizer
practicing not touching your face (good luck)
working from home
not shaking hands
washing hands, using hand sanitizer
practicing not touching your face (good luck)
working from home
24/ China's unprecedented success in containment has led us down the wrong path.
We can't do what they did.
Not just in terms of open society, but in sheer resources.
In Wuhan >1,800 TEAMS of epidemiologists, min 5 people/team, were tracing tens thousands of contacts a day
We can't do what they did.
Not just in terms of open society, but in sheer resources.
In Wuhan >1,800 TEAMS of epidemiologists, min 5 people/team, were tracing tens thousands of contacts a day
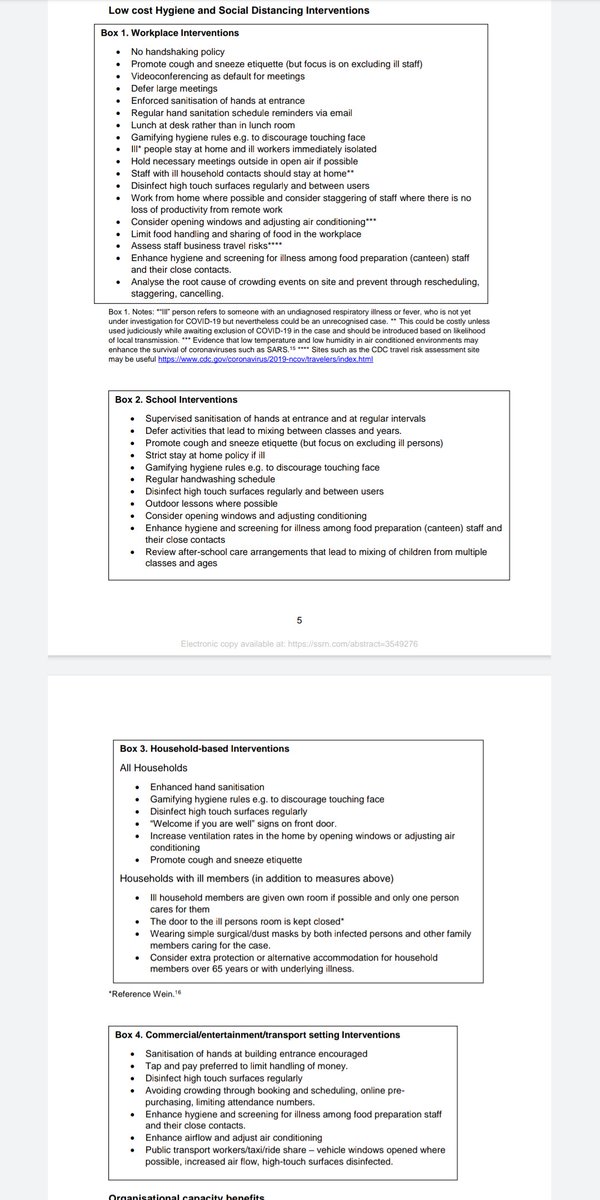
This is the best description of what an expanded set of such "Pre-Emptive Low Cost Social Distancing and Enhanced Hygiene" measures could be.
Also, excellent clear writing from @CraigBDalton
papers.ssrn.com/sol3/papers.cf…
Also, excellent clear writing from @CraigBDalton
papers.ssrn.com/sol3/papers.cf…
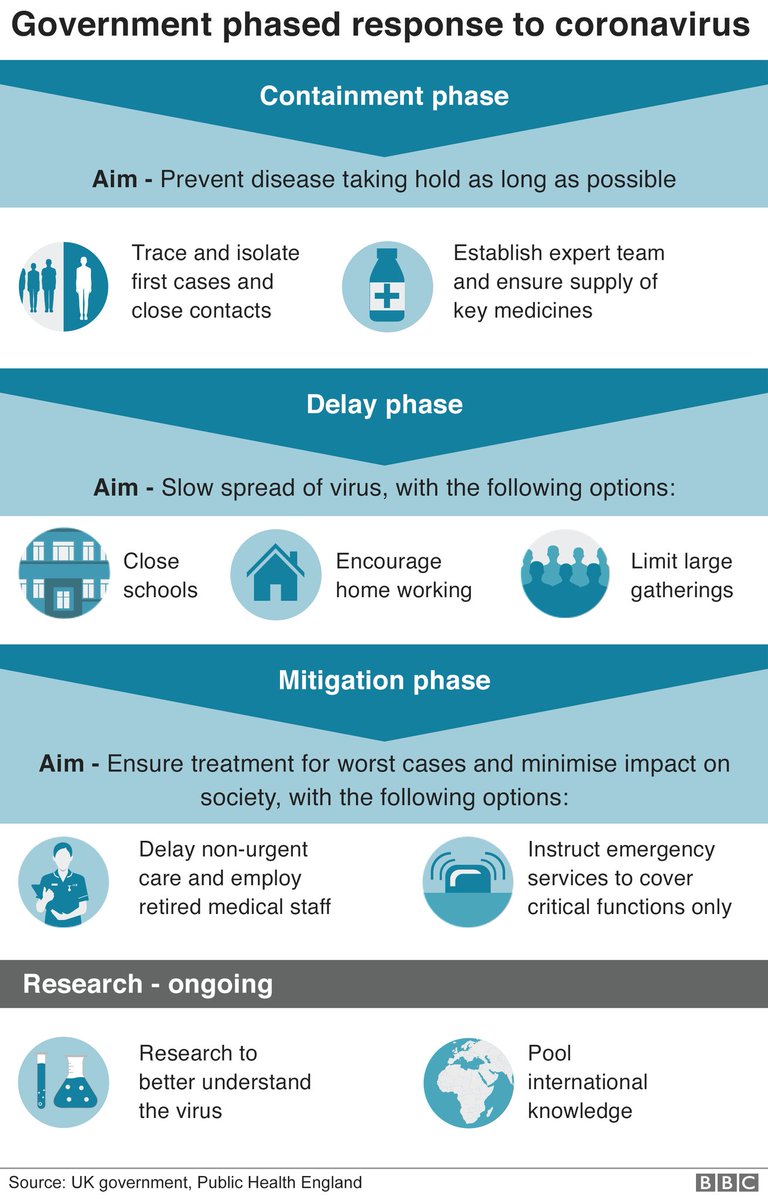
25/ grateful to those who have pointed out that other countries have provided exactly this sort of clarity of strategy.
Of course with a country as large/heterogenous as US, different locales will step through at own pace, not nationwide.
Here's the UK's
bbc.co.uk/news/amp/uk-51…
Of course with a country as large/heterogenous as US, different locales will step through at own pace, not nationwide.
Here's the UK's
bbc.co.uk/news/amp/uk-51…
Credit for graphic @drewaharris