1/ @UCSF is one of the top medical schools in US, think {Harvard, Johns Hopkins, Penn, Stanford, UCSF, in some order or other, depending on topic}. @Bob_Wachter is Head of Dept of Medicine (& author of fine books Internal Bleeding, The Digital Doctor...} He does daily updates.
2/ On March 19, he ran a panel of @UCSF experts.
This is well-worth watching, although non-expert eyes will glaze over at a few parts. Don't worry about that.
There's important stuff, like on drugs being hyped before serious trials happen, as per Trump.
This is well-worth watching, although non-expert eyes will glaze over at a few parts. Don't worry about that.
There's important stuff, like on drugs being hyped before serious trials happen, as per Trump.
3/ Since that's hot, I'll start there, with a few excerpts, but listen to Dr Luetkemeyer. Treatment is no substitute for vaccines (we don't have) or distancing we can do, but doctors who see patients must evaluate research on treatments.


4/ She gives overview: who should we treat (critically ill or those with moderate disease), and what kinds of treatment? Says what we know and what we don't.
This is way serious people talk about something that is complex.
This is way serious people talk about something that is complex.

5/ When has horse left barn in treatment?
Early: high viral load, but not when people sickest, some therapies were helpful with SARS.
Later: those therapies don't help so much, then maybe anti-inflammatories vs lung & myocardial (heart) injury
Early: high viral load, but not when people sickest, some therapies were helpful with SARS.
Later: those therapies don't help so much, then maybe anti-inflammatories vs lung & myocardial (heart) injury

6/ So HOW do we treat people?
(Now we hear about some of the names of drugs people are throwing around.)
Right NOW, we do not have any FDA-approved therapies, but we have others used for other diseases & off-label drugs being heavily investigated.
(Now we hear about some of the names of drugs people are throwing around.)
Right NOW, we do not have any FDA-approved therapies, but we have others used for other diseases & off-label drugs being heavily investigated.

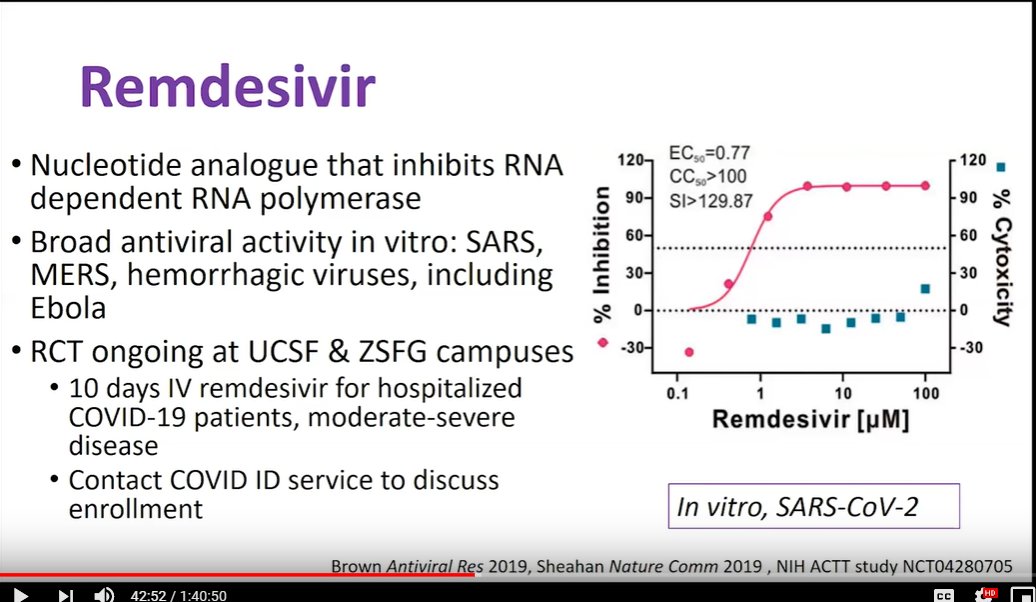
7/ Remdesivir
RCT = Randomized Controlled Trial, not anecdotes.
en.wikipedia.org/wiki/Randomize…
In-vitro = test-tubes, not humans
en.wikipedia.org/wiki/In_vitro
"without accompanying cytotoxicity (toxic to cells)" (blue squares)
at least 5 RCTs evaluating, incl UcSF+ZSFG
RCT = Randomized Controlled Trial, not anecdotes.
en.wikipedia.org/wiki/Randomize…
In-vitro = test-tubes, not humans
en.wikipedia.org/wiki/In_vitro
"without accompanying cytotoxicity (toxic to cells)" (blue squares)
at least 5 RCTs evaluating, incl UcSF+ZSFG
8/ Chloroquine (has been in news lately)
"We can argue whether immune modulating activity good or bad"
No data from RCTs, but many ongoing.
500mg doses off chart to right, may lead to concerns about toxiticy and drug-drug interaction.
DOSAGE MATTERS!
"We can argue whether immune modulating activity good or bad"
No data from RCTs, but many ongoing.
500mg doses off chart to right, may lead to concerns about toxiticy and drug-drug interaction.
DOSAGE MATTERS!

9/ Hydroxycholoroquine
May be more tolerable, data published last week.
Jury still out on appropriate dose.
(This is way knowledgeable people speak:
looks interesting, but we don't know, are studying as hard as possible.)
Graphs: up = more effective
May be more tolerable, data published last week.
Jury still out on appropriate dose.
(This is way knowledgeable people speak:
looks interesting, but we don't know, are studying as hard as possible.)
Graphs: up = more effective

10/ Hydroxycholoroquine + Azithromycin
Interesting article from day before
Non-RCT, small numbers, so many caveats.
Offered to take, with or without Az.
Interpret with GREAT CAUTION,
but indicates in-vivo (in humans) effects, being studied widely.
Interesting article from day before
Non-RCT, small numbers, so many caveats.
Offered to take, with or without Az.
Interpret with GREAT CAUTION,
but indicates in-vivo (in humans) effects, being studied widely.

11/ No effect of Lopinavir / ritonavir in RCT
Older treatment for HIV, MERS, SARS.
Day before, study published.
Unclear if steroids help/hurt.
Very sick population, so antivirals may be less useful.
(This is challenge, health pros try to help, but...)
Older treatment for HIV, MERS, SARS.
Day before, study published.
Unclear if steroids help/hurt.
Very sick population, so antivirals may be less useful.
(This is challenge, health pros try to help, but...)

12/ Many more!
(If you hear about some new wonder-drug on twitter, the pro's haven't been ignorant.)
(If you hear about some new wonder-drug on twitter, the pro's haven't been ignorant.)

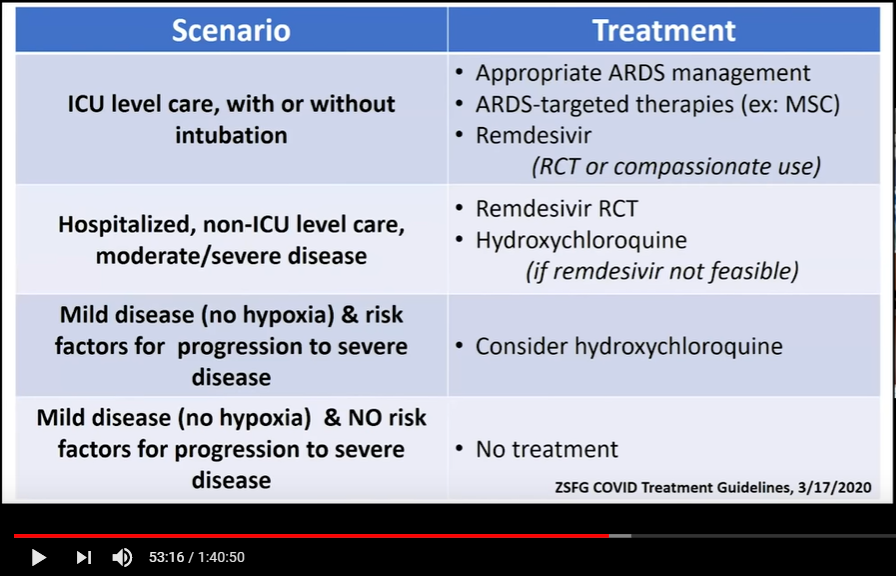
13/ Scenarios & Treatment guidelines (ZSFG, UCSF)
ARDS = Acute respiratory distress syndrome
en.wikipedia.org/wiki/Acute_res…
Compassionate use: mayoclinic.org/healthy-lifest…
ARDS = Acute respiratory distress syndrome
en.wikipedia.org/wiki/Acute_res…
Compassionate use: mayoclinic.org/healthy-lifest…
14/ Prophylaxis (efforts to *prevent* disease, not treat it)
dictionary.com/browse/prophyl…
Much concern, active investigation
dictionary.com/browse/prophyl…
Much concern, active investigation
15/ Then they go into Q&A, but
Now, back to the beginning of 100-minute video, briefly over other talks.
I'm no expert (although I'm on an advisory board for at @UCSF), but these are experts. Listen to them, starting with @Bob_Wachter
Now, back to the beginning of 100-minute video, briefly over other talks.
I'm no expert (although I'm on an advisory board for at @UCSF), but these are experts. Listen to them, starting with @Bob_Wachter
16/ Over last week or so, staggering amount of new information.
1st talk - overview
1st talk - overview

17/ "COVID-19" disease caused by "SARS-CoV-2" virus
(not the "Wuhan" or "Chinese" virus.)
(not the "Wuhan" or "Chinese" virus.)

18/ History of outbreak in Wuhan
Key Epidemiologic Questions: source, transmissions
Viral burden: early peak, high levels (contagious)
Cruise ships
Global spread
Flattening curve
Effective reproductive number (Re)
Wuhan & China: Case declines & Modelled Re
Lessons from 1918-19
Key Epidemiologic Questions: source, transmissions
Viral burden: early peak, high levels (contagious)
Cruise ships
Global spread
Flattening curve
Effective reproductive number (Re)
Wuhan & China: Case declines & Modelled Re
Lessons from 1918-19
19/ COVID-19 Clinical Manifestations

20/ Clinical Presentation
Good to watch if you are a doctor.
Good to watch if you are a doctor.

21/ Acute Respiratory Distress Syndrome (ARDS)
Another one good to watch if doctor, pathology pretty detailed.
Another one good to watch if doctor, pathology pretty detailed.

22/ High Flow for Early Hypoxic Respiratory Syndrome
(for doctors)
"not everybody will need intubation" (tube down throat)
"high flow nasal oxygen more effective in saving patients"
(up = good)
Specific detailed advice, incl "prone" position (not supine)
(for doctors)
"not everybody will need intubation" (tube down throat)
"high flow nasal oxygen more effective in saving patients"
(up = good)
Specific detailed advice, incl "prone" position (not supine)

23/ Last talk done in detail 3/-14/,
followed by ~40 minutes of Q&A, Q's submitted by audience. Some of this is for doctors, detailed but worth watching.
followed by ~40 minutes of Q&A, Q's submitted by audience. Some of this is for doctors, detailed but worth watching.

24/ That was a sample of high-quality information from experts in fast-developing situation.
Epidemiology is not simple.
Don't expect vaccines tomorrow.
Treatments need real RCTs to know what really works, safe, not hyped.)
Now, follow @Bob_Wachter or other experts at top places.
Epidemiology is not simple.
Don't expect vaccines tomorrow.
Treatments need real RCTs to know what really works, safe, not hyped.)
Now, follow @Bob_Wachter or other experts at top places.