
1) Welcome to a new #accredited #tweetorial, Update on New HFrEF Data from ESC 2022 with a Focus on Vericiguat. Our expert author is Giuseppe Galati MD, MMSc in Heart Failure, FHFA, @GiuseppeGalati_ , Consultant #Cardiologist #HeartFailure & #Cardiomyopathies 

2) @GiuseppeGalati_ is at San Raffaele Research Hospital, Milan 🇮🇹 @SanRaffaeleMI. This program is intended for #healthcare professionals & is accredited for 0.75h CE/#CME credit for #physicians #physicianassistants #nurses #nursepractitioners #pharmacists.
3) This program is supported by an educational grant from Bayer. See archived programs still open for credit at cardiometabolic-ce.com. Statement of accreditation & faculty disclosures at cardiometabolic-ce.com/disclosures/.🙏 FOLLOW US !
4) The prevalence & incidence of #HeartFailure (#HF) is constantly growing over the last decades, severely impacting expectancy and quality of life. These numbers justify why #HF has been defined as a real pandemic (even before and after the #Covid19 #pandemic)

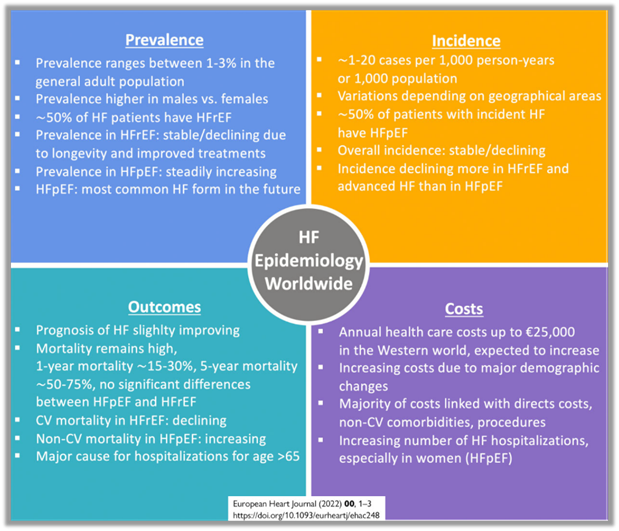
5) #HF is characterized by several hospitalizations during its natural history. Moreover, the rate of re-hospitalization is high both within 30 days & 12 months after hospitalization for #AcuteHF


6) After each #HF hospitalization (#HHF) survival is reduced almost of 50% and after the initial worsening #HF event each subsequent event becomes longer in duration and is separated by shorter intervals.
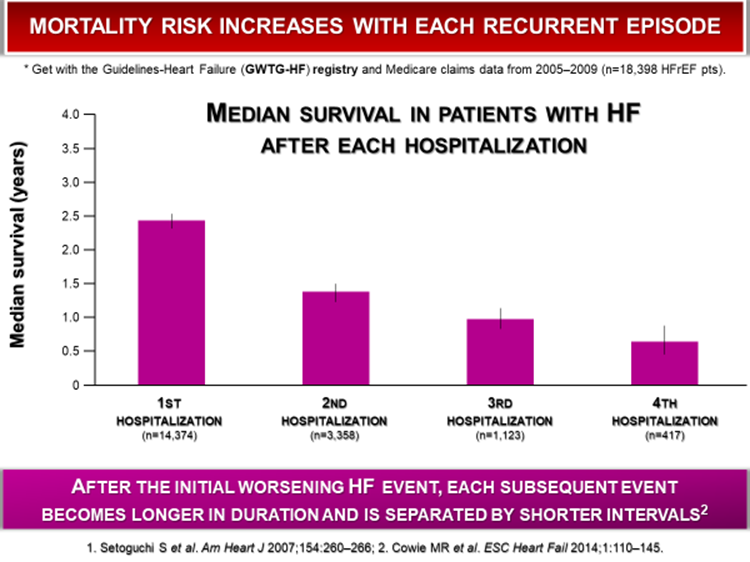

7) #HF progression is not linear and is punctuated by periods of worsening. #WorseningHF event are characterized by #HF signs & symptoms requiring therapy intensification. They include: Need for IV diuretics, for an urgent #HF visit or #HHF.

8) Patients with #WorseningHF are a distinct population characterized by a 4 times higher mortality when compared to chronic “stable” #HF and higher also to patients with #DeNovoHF. This is true both for #HFrEF and for #HFpEF. See the data of IN-HF outcome.


9) Moreover #CV_Death residual risk is high despite quadruple therapy and even on top of #OmecamtivMecarbil in #GALACTIC_HF. This trial enrolled a more severe #HF population with a 25% of patients currently hospitalized for #AHF
See
See

10) The residual risk of #CV_Death+ #HHF + #WorseningHF is high even in both #EMPEROR_Reduced and #DAPA_HF that enrolled a less sick population respect to #GALACTIC_HF. 1 of 7 pts in these #RCTs experienced a primary #EP event despite #ARNI, #BB, #MRA , #SGLT2i
See
See


11) Hypotension is a major limiting factor for pharmacological therapy especially in #HFrEF. #AHA/#ACC/#HFSA include hypotension in the criteria for #AdvancedHF. New therapies with low or no impact in ⬇️#bloodpressure in this population are a major change for these patients.

12) #HeartFailure is characterized by an oxidative stress that ➡️ #NO / #cGMP & #PKG deficiency contributing to both #vascular & #myocardial dysfunction. The NO/cGMP/PKG pathway is a regulator of several mechanisms & is also involved in the #PulmonaryHypertension pathophysiology


13a) In what class of medications is the #HFrEF drug vericiguat?
a. ACEi
b. SGLT2i
c. soluble guanylate cyclase (sGC) stimulator
d. RAASi
a. ACEi
b. SGLT2i
c. soluble guanylate cyclase (sGC) stimulator
d. RAASi
13b) It’s C. #Vericiguat is a drug with a unique mechanism of action that selectively stimulates and boosts the NO/cGMP/PKG pathway restoring its physiological activity with positive effect on the #heart, the #vessels and the #kidney

14) #Vericiguat stimulates the NO/cGMP/PKG pathway through two different actions: enhancing the sensitivity of soluble guanylate cyclase (#sGC) to endogenous #NO by stabilizing the NO-sGC binding site and directly stimulating the #sGC through a binding site independent of #NO.


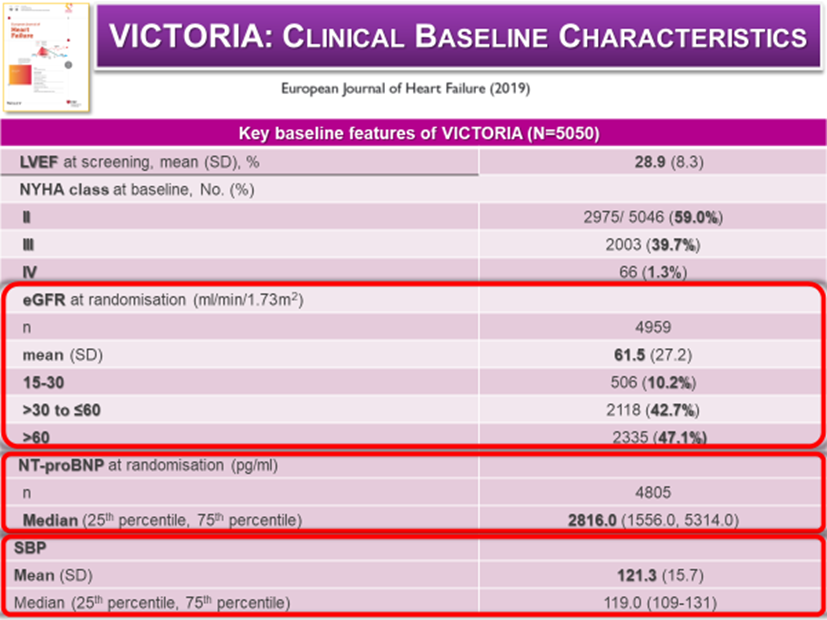
15) This specific mechanism of action & its positive effect has been tested in the large #VICTORIA RCT. This RCT enrolled >5000 #HFrEF patients with the following inclusion criteria (fig) to take #vericiguat once daily (biweekly uptitrated to the target 10 mg/day dose) vs placebo

16) #VICTORIA enrolled a particularly severe #HF population when compared to other RCTs: higher NYHA III class 39.7%, mean LVEF 28.9%, very high levels of NTproBNP (median) 2,816 pg/ml, ~84% had a HHF within 6 months & the other ~16% on IV diuretics managed as outpts.

17) The #HFrEF optimal medical therapy of #VICTORIA was comparable to that of #DAPA_HF & #EMPEROR_Reduced and included 14.5% of patients on ARNI, 59.7% on triple therapy (ACE-I/ARB/ARNI, β-blocker, MRA), 27.8% with an ICD and 14.7% with a CRT

18) After only 10.8 months of mean follow-up #VICTORIA showed significant ⬇️ in the primary #EP (#CV_Death + 1st #HHF) in #HFrEF with a RRR = 10 % (p =0.02). However, the benefit was significant for the 1st #HHF (p=0.048, RRR 10%) but not for #CV_death (p=0.269, RRR=7%).


19) The secondary endpoints analysis confirmed the benefit on #HHF, indeed total (first and recurrent) HHF were significantly reduced (p=0.02, RRR 9%) with no significant effect on #all-cause death (p=0.38, RRR:5%)

20) The benefit on primary #EP in #VICTORIA in terms of #AbsoluteRR was comparable to that of #DAPA_HF & even higher than that of #PARADIGM_HF. Despite the populations of these #RCTs were very different this benefit was achieved in a very short mean follow-up.


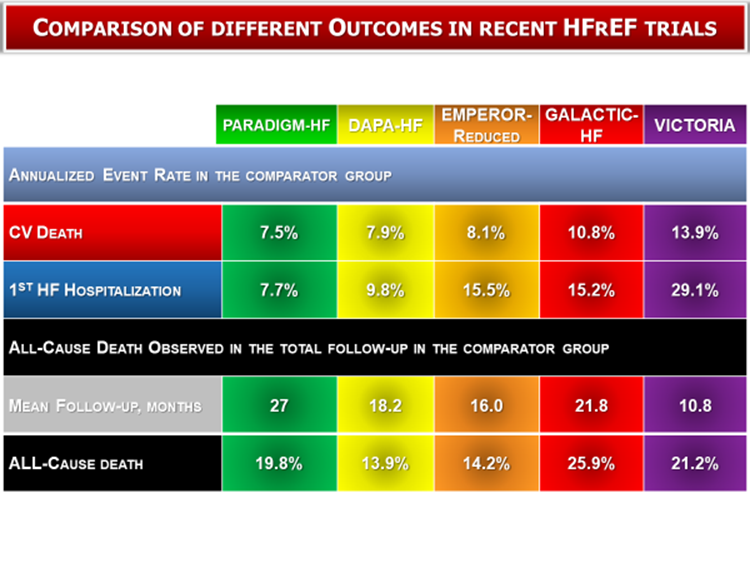
21) Although at a 1st glance the results achieved in #VICTORIA don't seem remarkable, the understanding of the population characteristics explains the important impact on #HFrEF. Indeed, pts enrolled in #VICTORIA had very severe #HFrEF when compared to all the #HFrEF RCTs


22) The #HFrEF severity of #VICTORIA’s pts is well described by the annualized event rate in the comparator group. The annual rate of #CV_death was 2 times higher than that of #PARADIGM_HF, #DAPA_HF, & #EMPEROR_R. The same happened for 1st #HHF and for #all_cause_death
23a) So what have you learned? #Vericiguat showed to be highly beneficial to a specific population with severe #HF, covering an unmet need of patients with #HF with which of the following characteristics?
23b) Enter your response & return TOMORROW for the correct answer & the remainder of this #accredited #tweetorial! 👍to @GoggleDocs @DrMarthaGulati @mmamas1973 @SABOURETCardio @HanCardiomd @SeguraCardio @ValleAlfonso @gcfmd @purviparwani @hvanspall @mirvatalasnag @gbiondizoccai
24a) Welcome back! We are reviewing HFrEF management with a focus on #Vericiguat. I am @GiuseppeGalati_ & I encourage you to follow @cardiomet_ce for all your #cardiometabolic CE/#CME needs! 👏to @butler @bianchinifra92 @edurontoFF #FOAMed #cardiotwitter
24b) Yesterday's knowledge ✔️: scroll back up to 23a & answer if you didn't already! The answer is d. In pts w/ #HFrEF a recent #HHF (< 6 m), eGFR>15 ml/min/1.78m2, SBP≥100 mmHG #vericiguat showed to be highly beneficial in covering an unmet need of this specific #HF population
25) #Vericiguat showed a high level of safety in #VICTORIA. Indeed, there were no significant differences in terms of Adverse Events (AEs) between #vericiguat and placebo. Only 6-7% of pts discontinued the drug because of #AEs .

26) #Vericiguat was safe, especially regarding the rate of hypotension & syncope. Indeed, there were no significant differences between the #vericiguat & the placebo group in terms of symptomatic hypotension & syncope (together or split).
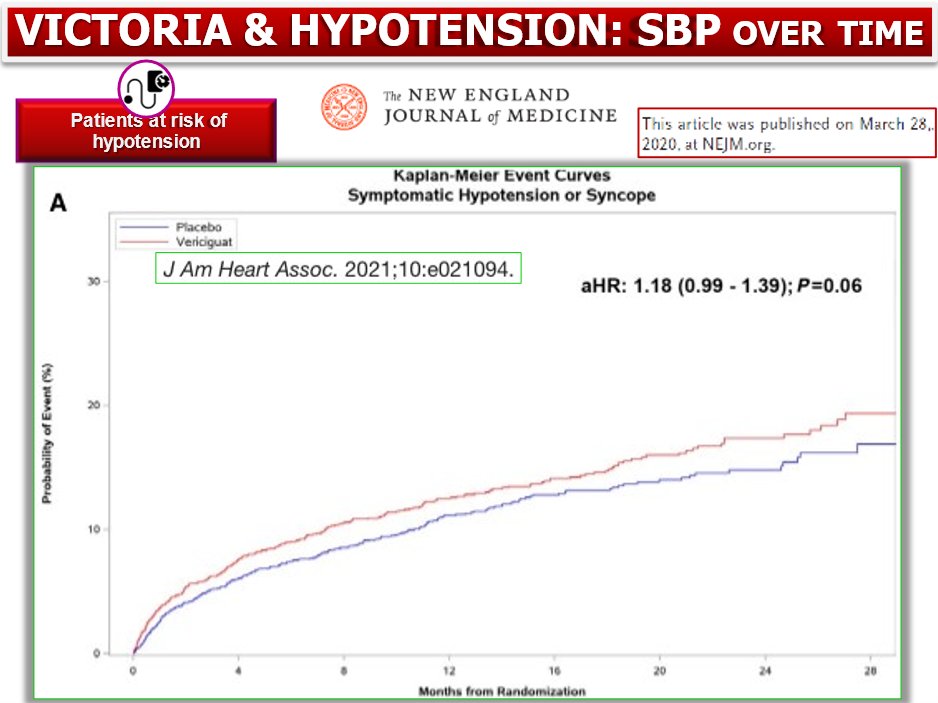
27) Furthermore, there were no significant differences in #SystolicBP between the 2 groups during the #VICTORIA follow-up. The #vericiguat dose has been managed as follows: If SBP≥100, ⬆️; if SBP ≥90 <100, maintain, if SBP<90 & no symptoms, ⬇️, if SBP<90 + symptoms, stop


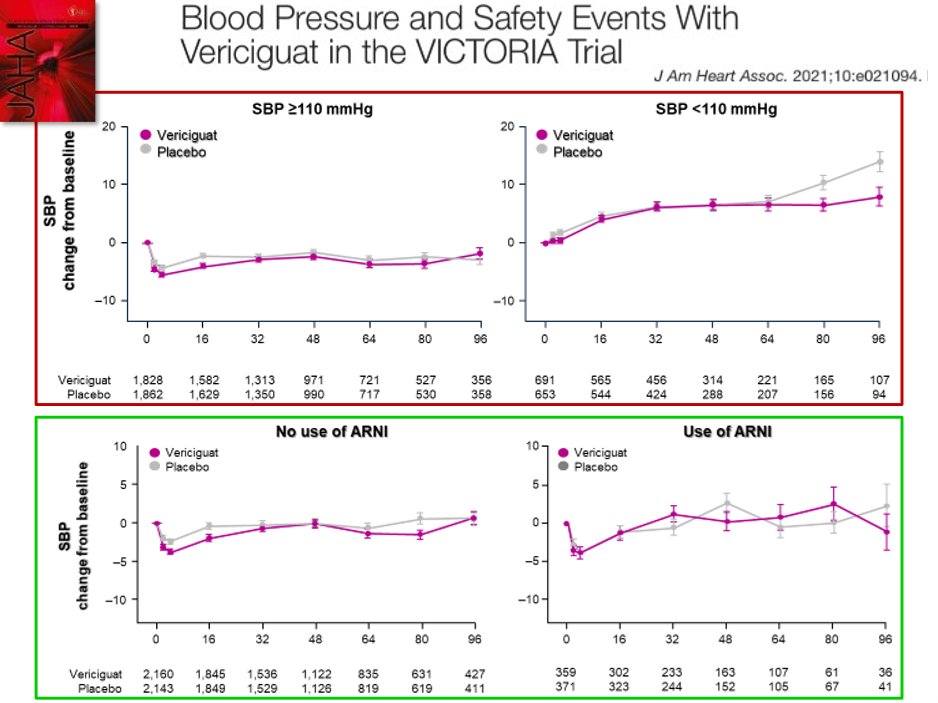
28) This analysis shows no significant differences between #vericiguat & placebo even in pts with hypotension (SBP<110 mmHg but ≥100 mmHg). #Vericiguat has no significant impact on #SBP even in pts on #ARNI. Finally, the lower the #SBP the higher the ⬇️of primary #EP

29) #Vericiguat was safe in terms of renal function. Indeed, there were no significant differences on the #eGRF & #creatinine between the 2 groups. Remarkably #VICTORIA enrolled pts with a more compromised renal function i.e. 52% with a #eGFR<60 & included #eGFR>15 ml/min/1.73m2


30) #Vericiguat was safe also regarding potassium levels. Indeed, there was no significant impact of #vericiguat in this population that is often at risk of hyperkalemia because of concomitant #CKD & RAASi use (ACE-i/ARB/ ARNI + MRA).

31) #Vericiguat showed a ⬆️safety profile in the #VICTORIA RCT regarding hypotension & syncope, renal function & risk of hyperkalemia. Therefore #vericiguat combines good efficacy + very good safety in a population with severe #HFrEF & #WorseningHF characterized by⬆️mortality

32) So what have you learned? #Vericiguat showed to be safe even when used in a particularly sick population of pts with #HFrEF. What were the areas of safety?
33) The answer is d. #vericiguat showed to be a safe drug even when used in a sick #HF population in terms of hypotension & syncope risk, renal impairment and hyperkalemia risk.
34) #Vericiguat showed in #VICTORIA that can change the trajectory of #HFrEF pts if started after a 1st #WorseningHF event preventing further episodes of hospitalization or further worsening and progression to #AdvancedHF.


35) #Vericiguat has currently a IIb/2b indication in #HFrEF after a 1ST #WorseningHF event across all the principal international guidelines on #HF (ESC/HFA + AHA/ACC/HFSA + CCS/CHFS)


36) #Vericiguat combines efficacy and safety in a specific high-risk group of #HFrEF pts. Moreover, it has a unique mechanism of action which is complimentary to the other #HFrEF #GDMT

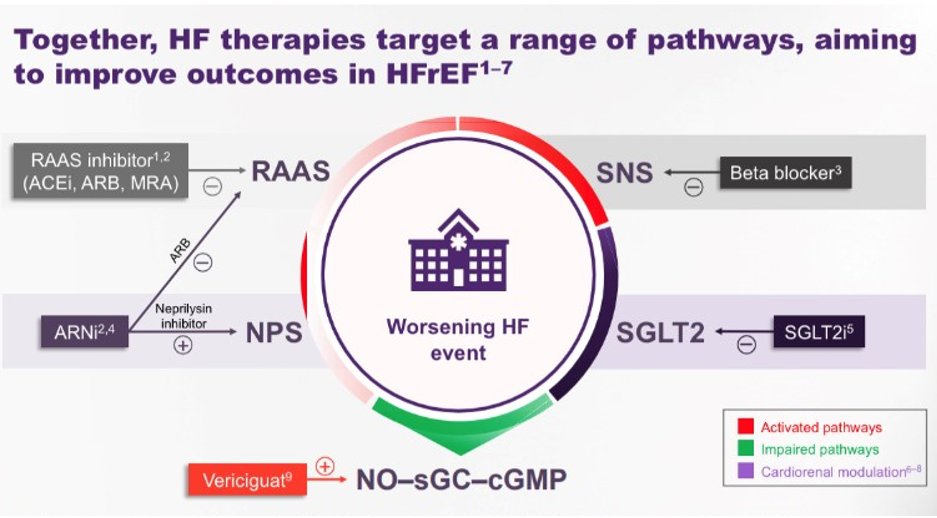
37) #Vericiguat selectively acts on soluble #GC while #ARNI have a partial activity on particulate #GC. After decades of neurohormonal modulation (ACEi/ARB/ARNI,MRA) we are finally moving beyond & targeting 🫀 with new molecules as #SGLT2i, #Vericiguat & #OmecamtivMecarbil


38) The #VICTOR trial (which is ongoing) will confirm the benefit of #vericiguat in a population of #HFrEF without a recent #WorseningEvent

39) Thanks for following along!!
👍@GoggleDocs @DrMarthaGulati @mmamas1973 @HanCardiomd @SeguraCardio @ValleAlfonso @gcfmd @purviparwani @hvanspall @mirvatalasnag @gbiondizoccai @SABOURETCardio
👍@GoggleDocs @DrMarthaGulati @mmamas1973 @HanCardiomd @SeguraCardio @ValleAlfonso @gcfmd @purviparwani @hvanspall @mirvatalasnag @gbiondizoccai @SABOURETCardio
40) Now go to cardiometabolic-ce.com/cardiorenal30/ and collect your 🆓CE/#CME, and FOLLOW US HERE for more #accredited #tweetorials--the ONLY such programs in the #cardiometabolic space! I am @GiuseppeGalati_
• • •
Missing some Tweet in this thread? You can try to
force a refresh









