How could you use IV to analyze #CABANA? I haven't seen the publication (is it published?) and am going mostly on what people have tweeted. But if most of the crossover happened early, before patients experienced endpoints, then it could be pretty straightforward...
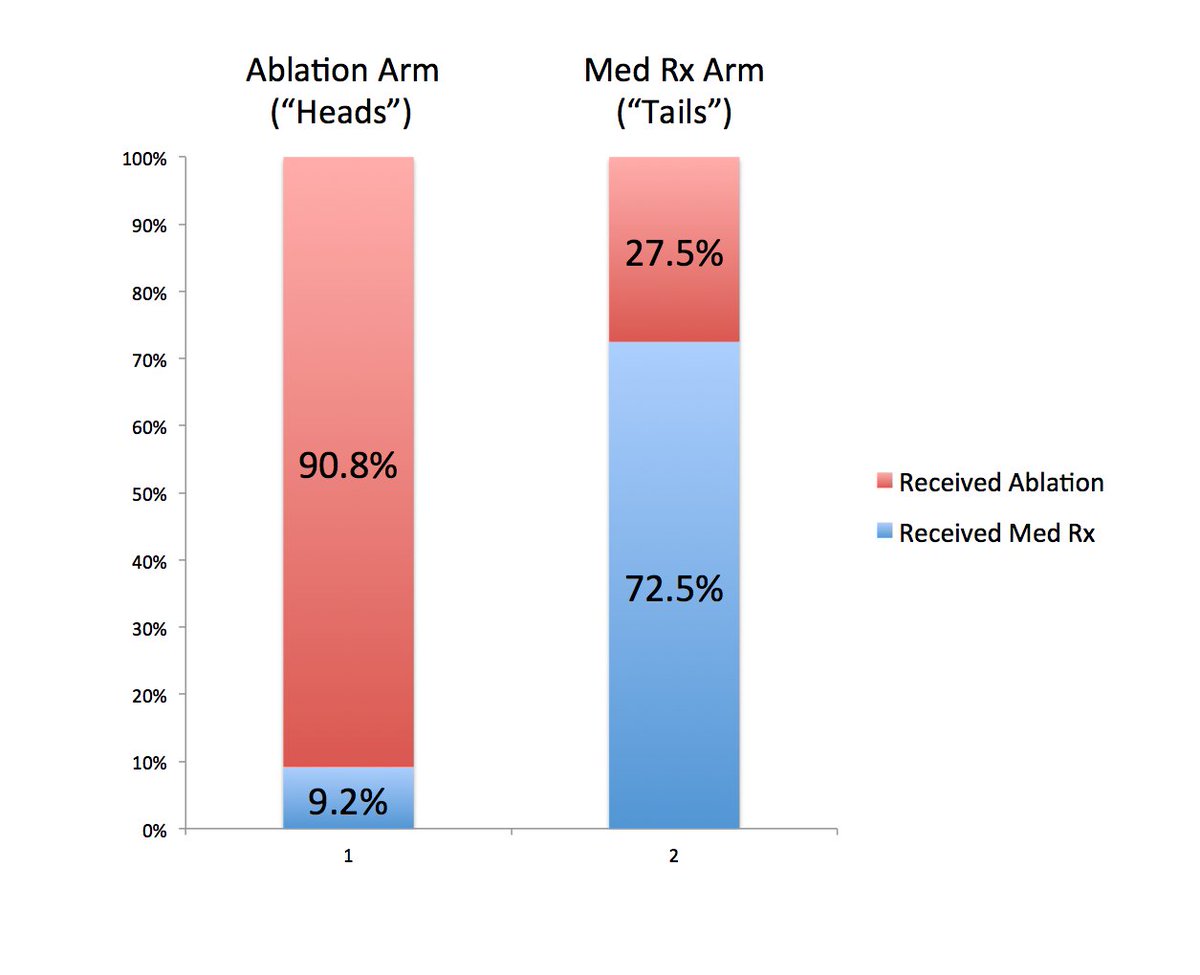
Getting randomized to ablation in the trial meant that you were very likely to get it, but not in all cases. Similarly, getting med Rx meant very likely to get med Rx, but not in all cases. So the breakdown is something like below. 
If you imagine that the populations in both arms are identical (which is true on average), then for every patient in one arm, there is his/her equivalent doppleganger who is identical in all ways, except got randomized to the other arm.
We can now divide up this twin population into 3 groups. Those that no matter what arm they were assigned received ablation ("Always ablation"), those that did not receive ablation no matter what the arm ("Never ablation"), and those where each twin received Rx that was assigned
It would look something like this for CABANA. The middle group - those that would go along with whatever was assigned - is the one that informs the entire treatment effect observed. They are the "compliers" or in econ speak, the "marginal" population.
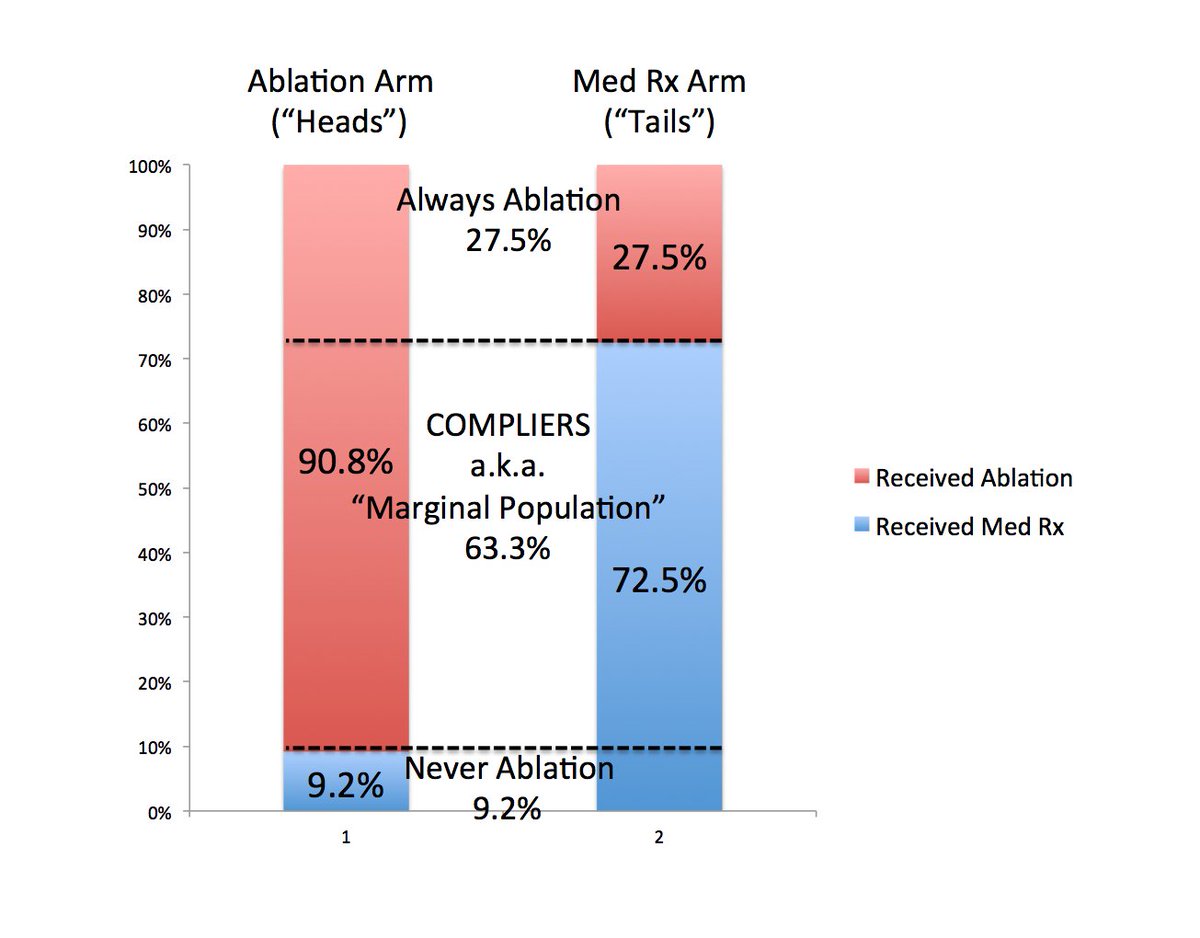
A very rough back of the envelope way to estimate a treatment effect then is to just divide the observed effect by 0.63 which is the proportion of compliers in the study population. In other words, the true effect is larger than the ITT. (If HR < 1, then multiply by 0.63).
Formally, we would predict the likelihood of each participant receiving ablation vs med Rx based on their randomization arm (aka the instrumental variable) and their other characteristics. The variable being "instrumented" is the actual treatment received.
So each patient in the ablation arm would have a high probability of receiving ablation, but not 100%. And vice versa for the Med Rx arm. Patients in the ablation arm would have values centered around 0.91 with some variation; patients in the med Rx would have values around 0.28.
You can then use regression to estimate the the association between this variable (representing "instrumented" receipt of ablation) which ranges from 0 to 1 with your outcome of interest.
The coefficient of this variable represents the effect of going from 0 to 1 on the predicted probability of receiving ablation: in other words, it is the treatment effect of not receiving vs. receiving ablation among the compliers in the study.
Make sense?
Make sense?
asks: So what does ITT mean relative to IV? ITT is what you get ignoring the non-compliance. It gives the effect of being randomized to one arm vs. another among the entire RCT sample. IV gives the effect of being randomized among the compliers in the study.
The degree to which ITT and IV depart is directly proportional to the degree of non-compliance/crossover in the study. If everyone did what they were told, they would be identical.
Good ?s here. @mirvatalasnag
For IV, this doesn’t introduce a “bias” but rather influences the generalizability. Crossovers don’t contribute any information, so the Rx effect is only applicable to the non-crossovers. On the other hand, Xover DOES bias per protocol analyses in the situation you describe.
2) if xover is random, then higher vs lower xover only affects precision (CIs) of IV and not the point estimate. If Xover is not random, then higher crossover makes rx effect less generalizable if Xover is higher. In most cases, more Xover leads to more bias to the null.
Bias to the null is not strictly a bias in this case, but rather you are measuring the effect in a population where there may truly be less benefit.
? here.
It’s like doing a propensity score. Take sample, use regression, outcome is Rx received and primary predictor is randomized treatment arm. We tend also to include all the patient covariates as well. From this model you can generate a predicted probability, similar to a prop score