
,
54 tweets,
16 min read
Read on Twitter
Have just looked at the terms of reference website for Victorian Mental Health Royal Commission & wanted to share some thoughts about the proposed priorities & what I see as some gaps. I’ll make a thread here. engage.vic.gov.au/royal-commissi… #MentalHealthRC #SpringSt
Perhaps I should start by saying that just about everyone in Australia will have spoken, or will speak, to a health professional or counsellor about mental distress, so this is not a fringe issue or something relating only to those with severe mental health conditions.
Alternatively, most or all will support someone in mental health crisis, or indirectly experience the impacts effective or poorly-functioning services during encounters with neighbours, friends, schoolmates, workmates, etc.
Why a Royal Commission? It’s generally agreed that Vic has distinct problems in MH services. Eg in 2015/16 Victoria had the lowest number of full-time equivalent staff with only 121.5 per 100,000 population compared with the national average of 132.9. sciencedirect.com/science/articl…
Part of the logic of those advocating for a Royal Commission is that it will bring attention to these discrepancies and – hopefully – attract institutional resources.
Others raise concerns that despite significant boosts in funding for research, policy-making and services over the past two decades, the statistics reveal that Australians are not enjoying improved mental health (as @helendoggett explained so well here: insidestory.org.au/do-it-better-o…)
Anyway, back to the terms of reference (or TOR). There are several proposed priorities (which people have until Jan 27 to rank), incl: suicide, accessibility of the system, prevention and early intervention, community mental health services, and so on. Seems totally reasonable.
Some veer to policy-speak (one concerns ‘deliverable reform to improve outcomes for people…’) and others seem to mash together multiple issues, e.g. one single priority combines ‘social isolation, depression, anxiety and trauma’.
Maybe they need to be that broad to cover the many issues. In any case, the priorities would - I'd imagine - seem important to most people who’ve engaged with mental health services at some point, and they’d probably seem reasonable to the average Victorian who hasn’t.
My main concern isn’t what’s included in the TOR but what is not: there is currently nothing on user-input for system design, nor on the use of compulsory powers and restrictive interventions, including potential harms experienced by people using services.
Consider @VMIAC, Victoria’s primary service user advocacy organisation. VMIAC promoted two main issues in their election advocacy last year: addressing harms experienced by those using services, incl through coercion, & promoting user-design of services
…neither of these issues appear as a proposed priority in the TOR. It's hard to imagine any other Royal Comm – on Indigenous issues, bushfire-affected communities, farming etc – where the concerns of the peak organisation of affected persons were not included in the proposed TOR
But for this thread, I want to focus on coercive/restrictive interventions, an area I’ve been researching for a few years. Victoria has distinct problems with coercion compared to the rest of Oz & I’ll try and show why I think the issues deserve consideration by the Commission.
Most people who experience mental health conditions can seek help on a voluntary basis. But in certain circumstances, mental health legislation authorises detention in mental health facilities and compulsory treatment regardless of a person’s wishes and preferences.
Under mental health legislation, involuntary treatment and psychiatric detention can only be imposed on people who are found to be severely unwell who are deemed to be a risk of harm to themselves or others, but it happens probably more often than many people think.
The @AIHW reported that in 2016-17, 45.4% of cases where a person is admitted for a mental health crisis to specialised psychiatric care were for people made involuntary under law. aihw.gov.au/getmedia/9e2e1…
In other words, there is nearly a one in two chance that a person hospitalised in a public hospital for a mental health crisis will be detained and treated involuntarily, meaning they cannot refuse certain interventions (e.g. administering of medication, detention in psych ward).
In residential mental health services, about 1 in 5 'service contacts' (or 19%) were for people deemed involuntary; in community mental health services, the figure was about 1 in 10 (or 13.8% of service contacts).
These stats suggest that coercion or restrictive intervention – whatever you term it – is not a minor element of mental health services—it’s a central part of what hospitals, non-hospital providers, psychiatrists, social workers and others do in mental health services.
Just to be clear, regardless of one’s views as to whether coercive practices are a ‘necessary evil’ in some circumstances, it is generally agreed that they are damaging for people in crisis, and also for the staff who impose them.
According to a WHO report, coercive practices are generally counter-therapeutic, impede people’s recovery and re-traumatise those who have previously experienced sexual and physical abuse, who appear to be the majority of people in mental health services. apps.who.int/iris/bitstream…
A recent World Psychiatric Association and @TheLancetPsych ’s Commission on the Future of Psychiatry, stated: the ‘Use of compulsion needs to be seen as a system failure’
Other senior UN figures, incl the Special Rapporteur on the Rights of Persons with Disabilities, and the Special Rapporteur for the Right to Health, and the Committee on the Rights of Persons with Disabilities, argue that these are clear human rights violations that need to stop.
This is all, of course, highly controversial (as I’ve **shameless plug** explored in my book) and its probably best to set those controversies aside for the minute.
What’s really important to point out here is that Vic has higher rates of several types of coercive interventions. Involuntary treatment outside the hospital, for example, in people’s homes – which is referred to as ‘community treatment orders’ (or CTOs) – are particularly high.
One study found that 5,675 Victorians were subject to CTOs in 2012, with year-on-year figures rising. This gave Victoria the highest rate of CTOs recorded nationally (eg Vic was 98.8 per 100,000 people, compared to, say, 30.2 per 100,000 in Tasmania). ncbi.nlm.nih.gov/pubmed/23136187
…but also, and more worryingly, the research suggested that Victoria has the highest rates of community treatment order-use recorded in the world.
There is some evidence, produced by Ruth Vine et al, that the use & duration of compulsory treatment in the community has reduced since the 2014 Mental Health Act was introduced. journals.sagepub.com/doi/abs/10.117…
But they also identified an increase in involuntary hospitalisations of people previously under CTOs since the Act came in. Victoria has other problems compared to the rest of Oz...
Recent @AIHW stats on the use of seclusion in mental health services suggest that Vic has far & away the highest rates of physical restraint (in which a person is overpowered by someone else, typically mental health staff). aihw.gov.au/reports/mental…
This figure was more than double the national average (Table RP.5). Surely this graph alone warrants the attention of the #MentalHealthRC 
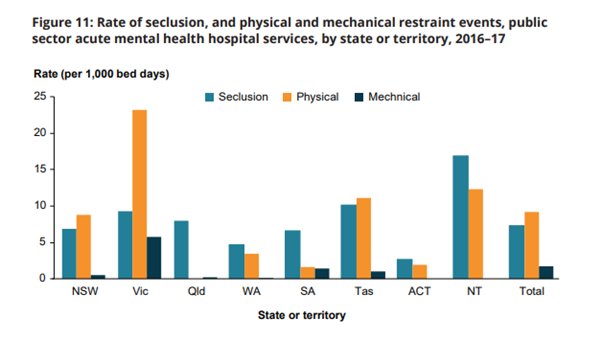
(BTW note the NT’s disturbingly high rates of seclusion). As you can see, Victoria seems to have highest rates of mechanical restraint (though this seems to conflict with Table RP.5, which puts South Australia in front).
(A quick note to @AIHW, that table I just posted seems to reflect the 2015-16 stats, not the 2016-17 figures).
When it comes to seclusion, the Vic public sector acute hospitals reportedly had the highest average duration of seclusion in the country. aihw.gov.au/reports/mental…
The average time a person in Vic spent in seclusion in public sector acute mental health hospital services was reportedly 10 hrs – again, the highest rate in Oz. (Disturbingly, national averages suggest these incidents mostly occurred in child & adolescent services) [Table RP.3].
Victoria also had the 3rd highest rates of seclusion per capita, and the second highest proportion of mental health-related hospital admissions that resulted in seclusion. aihw.gov.au/reports/mental…
Unfortunately, data doesn’t seem to be publicly available on the rates of seclusion/restraint used in SPECIFIC Victorian hospitals – as it is for NSW & other states. A Royal Commission would be in an ideal position to make this information public and improve reporting standards.
Some advocates, who have expressed the hope that the Royal Commission will attract much-needed funding to Vic services, may be reluctant to draw attention to the troubling issue of coercion in mental health services, or the harms they can cause.
(I also want to add that there have been some ad hominem attacks against advisors to the #MentalHealthRC, which seem unhelpful to me, shutting down rather than opening up debate. Also, MH services raise deeply personal issues for many, meaning debates get personal very quickly).
Perhaps some leading figures don’t see compulsion as a problem, or perceive that drawing attention to coercion is just ‘not good press’.
But I’m pretty sure most Victorians would agree that leading the country on rates at which we physically overpower distressed people, force medicate them in their homes, and lock them into seclusion rooms for the longest periods… is just plain bad.
Perhaps it’s even the case that Victoria’s higher rates of restrictive practice are CAUSED by the lower investment in staff compared to other states and territories, but if so, isn’t this precisely what a Royal Commission should identify?
Vic has a unique human rights apparatus compared to other parts of Oz. Rights are supposed to offer people both a sword & a shield; a sword to make rightful claims for a share of support, & a shield to prevent interference by the state & other individuals.
The focus needn’t be on one at the expense of the other. Citizenship rights require both: access to support (health, housing, and so on) and freedom from intrusion on bodily and physical integrity.
And it’s not just about rights, there’s lots of research that challenges the claim that coercive practices even achieve what they’re designed to do (as **2nd shameless plug** I explore in my book).
I certainly don’t think the issues I’ve listed here should be the sole or even main focus of the inquiry, but I hope those stats convince you that they deserve consideration. (If so, I’d encourage you to submit your thoughts to the Commission website)
For a more detailed report on alternatives to coercive practices, and initiatives to reduce and eliminate them, see this co-authored report written by myself and my colleagues @bmcsherr @croper2104 @flick_grey socialequity.unimelb.edu.au/news/latest/al…
One final point (and I’m really testing the platform w the length of this thread!): I’ve been reading @nikolasrose’s book, ‘Our Psychiatric Future’, which is a must read for anyone interested in psychiatry, psychology & the general future of how societies deal with mental health.
He encourages people not to dwell on the ‘hard cases’ or the pointy end of coercion (though he doesn’t suggest we ignore them either), instead inviting people to view to the broader array of services and social responses to distress and mental health crisis.
.@nikolasrose also argues that service user involvement in the development and operation of services, but also in the type of research to inform social and political responses to distress, can help address power imbalances that result in harmful practices.
Groups of service users, or people who have felt interfered with by services, have made well-founded criticisms of the actual practices of care experienced by those living with a psychiatric diagnosis, and articulate alternative forms of knowledge of mental distress.
If the #MentalHealthRC is to achieve its aims – to understand why people don’t seem to be enjoying improved mental health despite significant boosts in research, policy-making and service funding in recent decades – surely it should bring public attention to those voices.
Again, if you haven’t already, you may wish to share your views during the current public consultation on the terms of reference for the Commission. engage.vic.gov.au/royal-commissi… ... anyway, time for me to stop procrastinating and get back to my summer grant writing!
May be of interest.... ping @Oz4mentalhealth @johno0910 @PatMcGorry @LisaMBrophy @SANEAustralia @NMHC @sonialaw_aus @CroakeyNews @MelPetrakis @imhavic @IndigoDaya






