
,
19 tweets,
5 min read
Read on Twitter
In light of recent discussion, I wanted to share brief primer on prescribing methadone maintenance for those interested. It will largely be drawing from the following article on Safe Methadone Induction & Stabilization, as well as clinical experience. 1/
drive.google.com/file/d/0Byheg1…
drive.google.com/file/d/0Byheg1…
First off, I was troubled but not surprised by my informal Twitter poll that showed the vast majority of medical trainees have little to no exposure to methadone prescribing for opioid use disorder. Outside of dose verifications for admitted patients, experience was limited. 2/ 

So to start at beginning. A patient has moderate to severe OUD > 1 year & would like to enroll in methadone maintenance. Patient has struggled to stop using & has experienced significant negative consequences of use. Patient heard MMT can reduce mortality, risk of HIV, etc. 3/
Patient presents to an OTP & is evaluated for by medical team for enrollment. Diagnois confirmed. Patient is in withdrawal & is given methadone 30 mg. After few hours (peak effect at 2 hours), patient feels significantly better. Patient plans to return next day for next dose. 4/
Patient shows up next day & doesn’t feel great. Reports withdrawal symptoms that began few hours ago & woke patient from sleep. Also has severe cravings to use. Patient gets another 30 mg and again feels better. Plan is made to up-titrate the dose by 5 or 10 mg every 4-5 days. 5/
Patient then asks you a few important questions.
First, how will I know when I am at a therapeutic dose? You answer that an optimal methadone dose will not over-sedate you, and will achieve the following goals:
6/
First, how will I know when I am at a therapeutic dose? You answer that an optimal methadone dose will not over-sedate you, and will achieve the following goals:
6/
An optimal maintenance methadone dose will prevent w/d symptoms for at least 24 hours, decrease cravings & block effect of exogenous opioids, all while not over-sedating patient.
For our patient, the 30 mg dose treated their acute w/d symptoms. Are they at an optimal dose? 7/
For our patient, the 30 mg dose treated their acute w/d symptoms. Are they at an optimal dose? 7/
Our patient is not at an optimal maintenance methadone dose because they have breakthrough w/d symptoms, cravings and would not have blockade if they used heroin, so dose should be increased. But why must we be careful early in titration to not increase dose too quickly? 8/
From a pharmacokinetic standpoint, methadone is complex. It’s variably metabolized by liver & stored in fat to varying degrees. Interpersonal variation is immense. OD death risk is highest early in treatment, often due to difficulty assessing tolerance & ⬆️ dose too quickly. 9/
Quick aside, here are three most common scenarios in which we see OD when Rx’ing methadone maintenance (ie, not for pain).
✖️Single Large Dose
✖️Accumulated Toxicity (induction)
✖️Combined effect w/ other drugs
More details below extracted from article at top of thread. /10
✖️Single Large Dose
✖️Accumulated Toxicity (induction)
✖️Combined effect w/ other drugs
More details below extracted from article at top of thread. /10

So we have to balance importance of retaining people in care (if we go too slow, or dismiss symptoms — people will walk), with the need to titrate slowly to safely arrive at a stable, therapeutic dose. This is not easy. 11/
So, what dose is considered the optimal methadone dose for a patient? In other words, what is our target dose?
/12
/12
There really is no target dose for patients. As noted above, goals are to prevent w/d symptoms, reduce cravings & achieve opioid blockade — all while not sedating patient. That said, blockade thought to be more likely at doses > 80 mg. Dose to reduce cravings more variable. /13
What sort of risk do we counsel around and assess for during titration?
Generally, these fall into two categories.
1️⃣ Sedation
2️⃣ Cardiac risk
A big component of both is potential drug-drug interactions. /14
Generally, these fall into two categories.
1️⃣ Sedation
2️⃣ Cardiac risk
A big component of both is potential drug-drug interactions. /14
Regarding sedation, we of course counsel around avoiding use w/ other sedatives, taking dose as prescribed, etc. But drug-drug interactions also critical here. Biggest challenge I have encountered is Dilantin, but there are others. /15
Dilantin increases metabolism of methadone, so if added to regimen the patient will be uncomfortable, and will likely request a dose increase. If they then *stop* the Dilantin, they will likely be over-sedated. So we review med list and counsel around these risks. /16
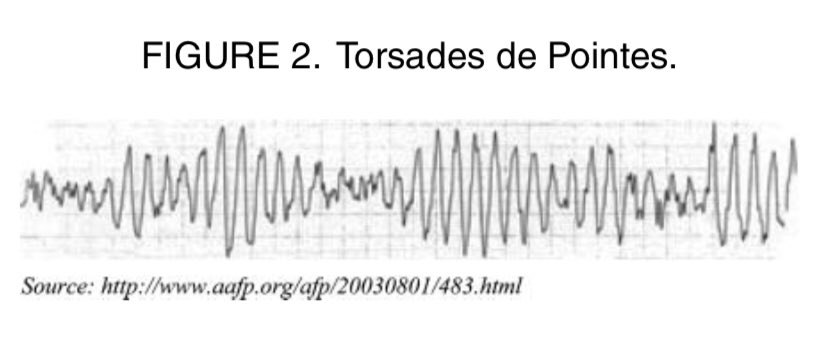
The 2nd big category is cardiac risk. Methadone seems to have dose-dependent relationship w/ QTc & prolonged QTc a/w Torsades — a serious & potentially fatal cardiac arrhythmia. That said, role of EKG screening is debated — and there’s no consensus. /17
drive.google.com/file/d/1gP9tb1…
drive.google.com/file/d/1gP9tb1…
So we generally explore history of structural heart disease, family history of sudden cardiac arrest & concurrent use of other meds that prolong QTc. We may check an EKG in these cases to inform counseling w/ stronger counseling re: possible dose reduction for QTc > 500 ms. /18

There’s lot more to methadone Rx’ing than covered here. How do we dx & manage fast metabolizers (peak/trough serum level, split dose), how do we assess for take-homes & how do we support people who want to taper or switch to Bupe (microdosing?), but hope basic primer helpful! /19










