
,
27 tweets,
10 min read
Read on Twitter
This month I revisit #COURAGE. The ultimate conversation starter among @JAMAInternalMed readers and interventional cardiologists. #CQOSpotlight
Quick someone tweet a concerning angiogram cine and ask if anyone else would refer a specific stable CAD patient to OMT!!
Quick someone tweet a concerning angiogram cine and ask if anyone else would refer a specific stable CAD patient to OMT!!

𝗕𝗮𝗰𝗸𝗴𝗿𝗼𝘂𝗻𝗱: The #COURAGE investigators provide longer survival follow-up on subset of the original study cohort to evaluate how the number of coronary lesions vs. amount of ischemia is prognostic for patients with stable CAD. ahajournals.org/doi/10.1161/CI…
The subset of patients received both quantitative coronary angiograms (QCA) and stress (SPECT) perfusion imaging.
A similar publication with long-term #COURAGE follow-up was published in the @nejm in 2015, but did not focus on the number of lesions or quantifying severity of ischemia on prognosis. nejm.org/doi/full/10.10…
And there has not been any evidence from any trial that treating stable CAD with an initial strategy of PCI over optimal medical therapy improves mortality or reduces events in the short or long-term.
However, there is increased risk for events for those with more severe CAD or more severe ischemia. So this study was meant to test if we can any important prognostic or treatment differences related to disease severity.
𝗠𝗲𝘁𝗵𝗼𝗱𝘀: The study cohort includes 60% of the original RCT (1379/2287 with both QCA and SPECT MPI and a subset with extended follow-up data, 33.5% (767/2287) linked to National Death Index as of Dec 2012.
The extended f/u was primarily VA clinical sites. Canadian patients were not included for extended f/u per the Canadian IRB protocol. Median follow-up in primary paper was 4.6 years. This analysis extended the observational period to median 7.9 years (0-15 year range).
For those in the extended f/u, survival was defined to December 31, 2012 (last available date for complete National Death Index data).
Number of significant coronary lesions were quantified as 1, 2, 3 from QCA. 6-segement model MPI results were dichotomized as No/Mild (0-2) or Mod/Severe (≥3). #dichotomania 👀
Analytically, the authors wanted to describe long-term survival based on these characteristics and evaluate predictors of mortality when accounting for both QCA/MPI results and randomized treatement PCI vs. OMT.
𝗥𝗲𝘀𝘂𝗹𝘁𝘀: A comparative table describing the characteristics of the full cohort and sub-cohorts is provided in Table 1. Overall, there are some differences in race, sex and minimal differences in other characteristics.

Table 2 is interesting and describes characteristics stratified by number of coronary lesions vs. ischemic burden (dichotomized). We see some more CCS 3 angina with more coronary lesions and not much symptom difference based on ischemia classification.

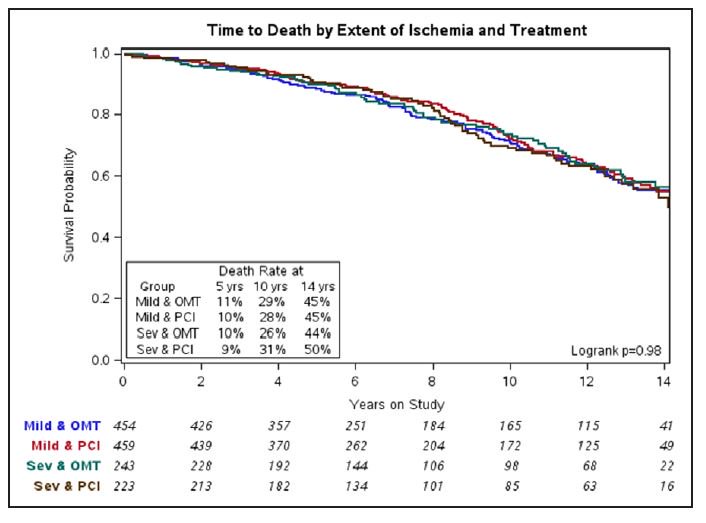
Figure 2 is a bit dense, but overall no real survival modulation based on randomized treatment.

KM curves based on number of diseased vessels look worse for 3-vessel disease. However, these are not adjusted curves so they don't account for age.

When looking at MPI results, no observed differences are noted on unadjusted KM curves.
Alright, our final table is of the actual adjusted results. How does intention-to-treat and baseline factors influence long-term survival ... .🥁
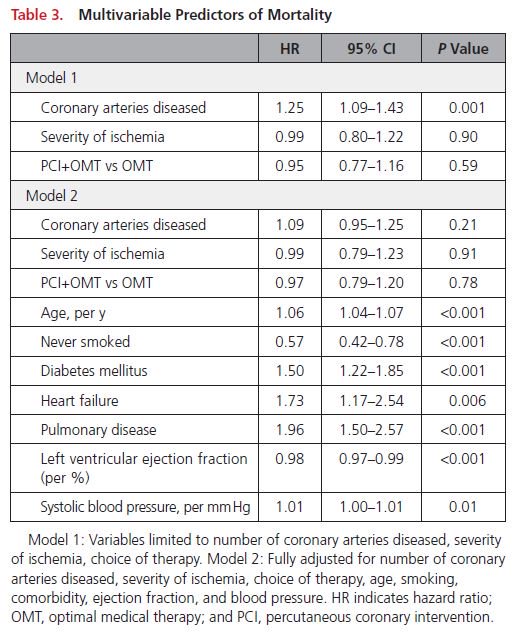
Model 1 only adjusts for coronary lesions, MPI ischemia, and intention-to-treat PCI vs. OMT. The number of coronary lesions is associated with mortality hazard. (no age adjustment or other low cost information)
Model 2 adjusts Model 1 with age (finally!!), smoking status, comorbidities, LVEF, and SBP. Here we see that coronary anatomy & ischemia, initial treatment strategy (up to 15 years ago 🧐) really don't predict long-term mortality.
𝗗𝗶𝘀𝗰𝘂𝘀𝘀𝗶𝗼𝗻: The authors conclude that based on their findings: "... we
observed that the severity of CAD as assessed by QCA predicted long-term mortality whereas the extent and severity of ischemia as assessed by SPECT MPI did not."
observed that the severity of CAD as assessed by QCA predicted long-term mortality whereas the extent and severity of ischemia as assessed by SPECT MPI did not."
Well, that's a pretty generous conclusion. Because it's basically a univariate association, since Model 1 didn't control for many basic facts we would know about a patient. In Model 2, we see that both QCA/Spect are not associated with mortality when adjusting for other factors.
Given that ~1/3 of patients crosssed over in #COURAGE and the primary analysis did not show a mortality advantage, a longer-term study is unlikely to observe any effect. This why we are anticipating results from the #ISCHEMIA trial. @GreggWStone
While it may be interesting to evaluate the relationship between coronary lesions and ischemic burden on survival, in a primarily negative RCT, we should not expect heterogeneity of treatments effects. Which some wonderful recent threads discuss!!! @f2harrell & @ProfHayward
Well, hope you enjoyed this month's #CQOSpotlight. @jaygirimd wrote a wonderful perspective. ahajournals.org/doi/10.1161/CI…
Although, @CircOutcomes it is time to drop "statistically significant" phrases in the near future.
And for those interested in how cross-over interacted with symptom in burden in #COURAGE. There's this earlier paper from the investigator group. ORBITA of course was run to address the non-blinded issues regarding randomization. @rallamee @ProfDFrancis ahajournals.org/doi/full/10.11…
@threadreaderapp unroll








