
,
82 tweets,
27 min read
Read on Twitter
Right ... it’s been 7+ years since I last put on a pair of a scrubs to do a nightshift in a hospital
This is a slightly odd night shift though ...
This is a slightly odd night shift though ...
Welcome to Snow Leopard Ward @EvelinaLondon!
Phase 1 of Snow Leopard, opened in 2016, is our Transitional Care Unit, supporting patients who need Long Term Ventilation as they head from our acute wards to home
Phase 1 of Snow Leopard, opened in 2016, is our Transitional Care Unit, supporting patients who need Long Term Ventilation as they head from our acute wards to home

We’re just about to open Phase 2 of Snow Leopard ... which will include three new dedicated bedrooms as part of our Children’s Sleep Centre

But, before we can admit children into the new facility, we have to test our new sleep equipment ... on sleeping people.
So, tonight I’m having a sleep study in our sleep lab, as part of the equipment testing protocols!
So, tonight I’m having a sleep study in our sleep lab, as part of the equipment testing protocols!

This is one of our sleep bedrooms.
They’re deliberately quite spartan, as we want a low-stimulation environment to try to encourage sleep!
They’re deliberately quite spartan, as we want a low-stimulation environment to try to encourage sleep!

The rooms are kitted out with sensitive video cameras, infrared monitors and microphones, and we can adjust the temperature


The view out the window is out to the Thames (over @KingsCollegeLon medical school building) ... but we have industrial blackout blinds to get the rooms as dark as possible.
We’ve also got increased soundproofing (Big Ben *will* bong again soon...)
We’ve also got increased soundproofing (Big Ben *will* bong again soon...)

And this is the control room where our overnight physiologists can monitor everything that happens as our patients ... me tonight! ... sleep

Absolutely! Most (soon to be all) of our inpatient studies are directly monitored. It allows high-quality studies to be obtained and, for ventilated patients, allows real-time titration to optimise settings
I’m having full polysomnography, which is generally our top-of-the-range sleep study.
It uses limited montage EEG to let us determine what sleep stage I’m in at different points through the night
It uses limited montage EEG to let us determine what sleep stage I’m in at different points through the night


Around my chest and abdomen are RIP (respiratory inductance plethysmography) bands, which allow my breathing movements and pattern to be monitored (this is the key bit to diagnose obstructive sleep apnoea and other sleep disordered breathing problems)

I’m also hooked up to an oxygen saturation monitor, and a transcutaneous carbon dioxide monitor, to assess my gas exchange as I sleep

On my legs there are EMG (electreomyography) leads which allow the tone and movements of my legs to be monitored

And there are ECG leads to monitor my heart rate (and a lead II rhythm)

Meanwhile on my face we’ve added EOG (electrooculography) leads next to my eyes (these help us tell when I enter dream/REM sleep), chin EMG (so we can tell if I grind my teeth!) ... and a throat microphone (to prove I don’t snore ... 😉)

... the nasal cannulae are the opposite to what you’d expect. They’re not delivering oxygen, they’re measuring the flow of air in and out of my nose
We’ve just done biocalibrations - lots of directed movements and breathing to allow Erica (the sleep physiologist on duty tonight) to synchronise our computers to the way I move and breathe
It’s surprising how quickly you get used to it!
And while many of our patients don’t sleep exactly as they would at home, we almost always get enough sleep to get the good quality data we need a
And while many of our patients don’t sleep exactly as they would at home, we almost always get enough sleep to get the good quality data we need a
All the leads connect to a master box by the bed, which then sends the signals to Erica in the control room.
And, with that, I shoud really put my phone down and try to sleep 😁💤
And, with that, I shoud really put my phone down and try to sleep 😁💤

So I slept better than I thought I would ... about 7.5 hours of sleep (and no morning commute to my office, just walking up a flight of stairs!)
This is what all those leads translates to:
This is a 30 second snapshot of data - we call these epochs
This is what all those leads translates to:
This is a 30 second snapshot of data - we call these epochs

At the top there is an overview of the whole night - this shows my oxygen saturation level, heart rate and carbon dioxide level.
For severe cases of sleep disordered breathing, this alone can often be enough to tell us there’s a problem (mine’s fine!)
For severe cases of sleep disordered breathing, this alone can often be enough to tell us there’s a problem (mine’s fine!)

Below that is the detailed data representation
EEG leads show the activity of the brain during sleep.
There are particular patterns associated with different sleep stages that let us determine the type of sleep occurring at any point
EEG leads show the activity of the brain during sleep.
There are particular patterns associated with different sleep stages that let us determine the type of sleep occurring at any point
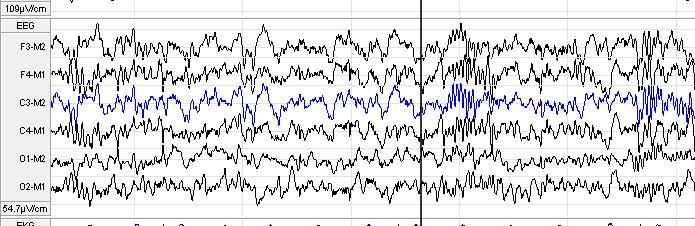
This is the respiratory data, looking at the pattern of respiratory movements and airflow ... and the snore mic

ECG lets us assess heart rate mainly, while the EMG on chin and legs lets us assess muscle tone - we lose tone in REM sleep, which helps us identify that when it arrives.
The limb leads also let us monitor leg movements, in particular looking for periodic limb movements
The limb leads also let us monitor leg movements, in particular looking for periodic limb movements

Detailed analysis of a study like this will take one of our expert physiologists a few hours
They then write a comprehensive report summarising the findings, which then comes to one of the consultant team to add clinical interpretation
They then write a comprehensive report summarising the findings, which then comes to one of the consultant team to add clinical interpretation

Polysomnography (PSG) is our “top-level” study; about 20% of our detailed studies are of this sort
Because we don’t need EEG data to answer many clinical questions, around 75% of our studies are cardiorespiratory studies, which just look at respiratory data
Because we don’t need EEG data to answer many clinical questions, around 75% of our studies are cardiorespiratory studies, which just look at respiratory data

Increasingly we can do these types of cardiorespiratory studies at home - 30% of all our detailed studies were done at home last year.
We use simple kit that families can be taught to put in place and use at home, and get great results - and avoid a night in hospital!
We use simple kit that families can be taught to put in place and use at home, and get great results - and avoid a night in hospital!

Our team are very skilled at helping children tolerate all the sensors ... but if we don’t need to stick glue in their hair (to hold the EEG electrodes in place) we tend to avoid it
(I’m still picking it out of my hair 3 hours after my study stopped!)
(I’m still picking it out of my hair 3 hours after my study stopped!)
(I’ll be talking about how we use PSG in assessment and management of sleep disorders in children at the @LondonPaedResp conference at the beginning of April)

So ... what can we tell from all that data we collected while I slept?
LOTS!
It takes a few hours for one of our skilled and experienced senior sleep physiologists to analyse it, and produce a detailed report.
LOTS!
It takes a few hours for one of our skilled and experienced senior sleep physiologists to analyse it, and produce a detailed report.
At the top is the summary data.
This is my hypnogram, the diagrammatic representation of my trip through sleep’s different stages through the night
W: Wake
R: REM (‘dream’) in red
N1: Transitional sleep
N2: Light sleep
N3: Deep sleep
(The ‘N’ stands for ‘Non-REM’)
This is my hypnogram, the diagrammatic representation of my trip through sleep’s different stages through the night
W: Wake
R: REM (‘dream’) in red
N1: Transitional sleep
N2: Light sleep
N3: Deep sleep
(The ‘N’ stands for ‘Non-REM’)

This is a fairly typical hypnogram, with a normal distribution of sleep stages.
You can see that most of the deep sleep is at the beginning of the night, with light sleep and REM predominating later
It’s not quite textbook (real life is always messier!) but it’s not bad!
You can see that most of the deep sleep is at the beginning of the night, with light sleep and REM predominating later
It’s not quite textbook (real life is always messier!) but it’s not bad!

We can calculate exactly how much sleep I got last night: 7 hours and 11 minutes.
I fell asleep fairly quickly (anything less than 30 minutes is pretty normal)
I fell asleep fairly quickly (anything less than 30 minutes is pretty normal)

Something that often surprises people are those 20 awakenings.
Although I woke several times overnight, they were generally brief - I only remember 2 of them!
We all wake and settle back as we sleep
33 minutes of “wake after sleep onset” sounds a lot but is fairly normal.
Although I woke several times overnight, they were generally brief - I only remember 2 of them!
We all wake and settle back as we sleep
33 minutes of “wake after sleep onset” sounds a lot but is fairly normal.
Sleep efficiency is one way of assessing this: it’s basically the percentage of time spent asleep versus the time spent in bed.
Anything above 85% is fine, and my sleep efficiency of 91% is perfectly respectable.
Anything above 85% is fine, and my sleep efficiency of 91% is perfectly respectable.
We can go a step further, and quantify the time/proportion spent in different sleep stages.
This can be helpful in assessing sleep quality, and can sometimes give us clues about specific diagnoses
This can be helpful in assessing sleep quality, and can sometimes give us clues about specific diagnoses

So - lets have a look at the study itself.
Remember those biocalibrations - this is what that looks like, as we check that our sensors are set up to capture the data we need
Remember those biocalibrations - this is what that looks like, as we check that our sensors are set up to capture the data we need

These are the electrooculography (EOG) inputs ... as I blink, you can see the traces diverging

And here’s the chin electromyography (EMG) input, measuring tone in my jaw muscles as I grind my teeth

Here’s the limb EMG traces - on the left, resting tone, on the right as I wiggle my toes, you can see the muscle activity increase
This lets us gauge events later in the night
This lets us gauge events later in the night

This is me tweeting last night 😁
“Lights out” on the left-hand stickie
“Phone away, Mike trying to sleep” on the right
... demonstrating some suboptimal sleep habits there Dr Sleep Consultant ... 😳
“Lights out” on the left-hand stickie
“Phone away, Mike trying to sleep” on the right
... demonstrating some suboptimal sleep habits there Dr Sleep Consultant ... 😳

This is me awake, starting to think about sleep.
My brainwave activity though is still pretty busy. Under my eyelids, my eyes are starting to gently roll
My brainwave activity though is still pretty busy. Under my eyelids, my eyes are starting to gently roll

A few moments later though, you can see the brainwave activity start to change ...

... and I drift into sleep. 💤

Once asleep we can identify different sleep stages by particular characteristics of EEG, EMG and EOG
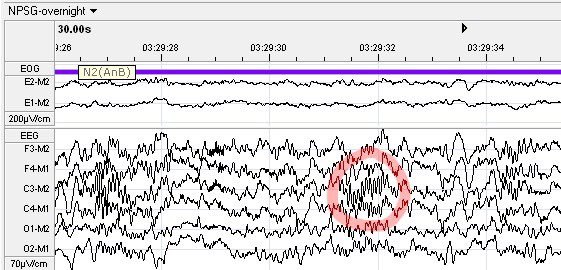
This is N2: light sleep
Inside the red circle is a sleep spindle, one of the features of N2. They’re signs of some of the brain’s processing of learning and memory during sleep
This is N2: light sleep
Inside the red circle is a sleep spindle, one of the features of N2. They’re signs of some of the brain’s processing of learning and memory during sleep
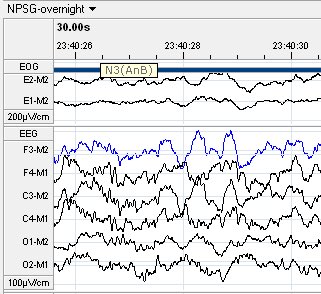
This is N3: deep sleep
We see characteristic slow waves, while lots of the body’s physiology becomes slow and regular.
During N3 we repair and recharge our batteries for the next day
We see characteristic slow waves, while lots of the body’s physiology becomes slow and regular.
During N3 we repair and recharge our batteries for the next day
Lastly this is REM
Brainwave activity looks most like wake
On the EMG, tone reduces significantly - we are paralysed in REM to stop us acting out our dreams, and this is achieved by cutting tone to our voluntary muscles
Brainwave activity looks most like wake
On the EMG, tone reduces significantly - we are paralysed in REM to stop us acting out our dreams, and this is achieved by cutting tone to our voluntary muscles

This is where REM gets its name from: sudden isolated rapid eye movements evident on the EOG leads

Our physiologists go through the study and stage each section of sleep.
We can then start to look at what’s going on
Here’s a reminder of what the whole study looks like (this is 60 seconds of light sleep)
Let’s have a look at what’s happening as I breathe...
We can then start to look at what’s going on
Here’s a reminder of what the whole study looks like (this is 60 seconds of light sleep)
Let’s have a look at what’s happening as I breathe...

These are the respiratory channels:
Nasal flow, measuring airflow in and out as I breathe
Thoracic and abdominal movements, allowing us to assess breathing pattern
This is me holding my breath during biocalibrations: no movements, air flow stops, then I start to breathe again
Nasal flow, measuring airflow in and out as I breathe
Thoracic and abdominal movements, allowing us to assess breathing pattern
This is me holding my breath during biocalibrations: no movements, air flow stops, then I start to breathe again

Normally our breathing effort should be synchronised: in phase.
Our chest and abdomen move together as we breathe in and out
Our chest and abdomen move together as we breathe in and out

If there is any obstruction to airflow, our breathing effort becomes unsynchronised as my muscles try to create more pressure to overcome the obstruction
When it’s mild, like this, we call it “respiratory phase shift”
When it’s mild, like this, we call it “respiratory phase shift”

As obstruction to airflow increases, my muscles move completely out of phase - the chest and abdomen move in opposite directions
We see this pattern - “paradoxical breathing” - in babies with illnesses like bronchiolitis, with chest and tummy looking like a see-saw
We see this pattern - “paradoxical breathing” - in babies with illnesses like bronchiolitis, with chest and tummy looking like a see-saw

If this increased effort still isn’t enough, air stops flowing ... and I have an apnoea, a pause in breathing, even though my breathing muscles are still trying to shift air

As this happens, my oxygen saturation and heart rate drops slightly - and this triggers my brain to briefly rouse to a lighter stage of sleep, which helps overcome the obstruction ... so air flows again
It all sounds very scary, but our brains are very good at keeping us safe!
It all sounds very scary, but our brains are very good at keeping us safe!

We need to see the change in oxygen saturation to be able to score this as an event, something which is affecting the quality of sleep
Occasionally we have normal pauses in our breathing, and these *don’t* affect sleep quality usually ... but ...
Occasionally we have normal pauses in our breathing, and these *don’t* affect sleep quality usually ... but ...
Here’s me having another obstructive apnoea ... but this time I don’t drop my oxygen levels.
If this had been a cardiorespiratory study, without EEG, we would have not been able to comment on this.
However ...
If this had been a cardiorespiratory study, without EEG, we would have not been able to comment on this.
However ...

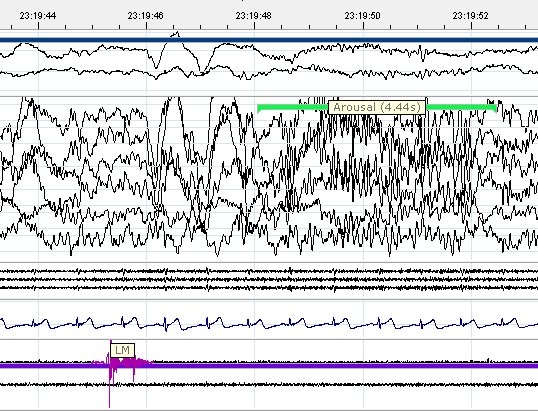
... because I’m hooked up to EEG, we can see that this apnoea triggers what we can an arousal (less saucy than it sounds!)
The apnoea happens during REM sleep, but it triggers me to rouse back to light sleep, meaning my sleep quality HAS briefly been affected by it
The apnoea happens during REM sleep, but it triggers me to rouse back to light sleep, meaning my sleep quality HAS briefly been affected by it

Remember I said we’re all paralysed during dream/REM sleep, to stop us acting out our dreams?
That muscle paralysis also makes our breathing more vulnerable. Most apnoeas happen during REM, and our brain responds by jumping us out of REM to switch off the paralysis. Clever!
That muscle paralysis also makes our breathing more vulnerable. Most apnoeas happen during REM, and our brain responds by jumping us out of REM to switch off the paralysis. Clever!
This is one of the benefits of PSG - it allows a much more sensitive assessment of sleep quality.
We often don’t *need* that level of sensitivity, but it can be helpful in some situations where we are assessing breathing in sleep
We often don’t *need* that level of sensitivity, but it can be helpful in some situations where we are assessing breathing in sleep
A few arousals like that aren’t a problem but if there are lots of them, they cause what we call sleep fragmentation.
The person with the bottom hypnogram is going to wake up feeling pretty unrefreshed as all those arousals mean they haven’t got the full benefit of their sleep
The person with the bottom hypnogram is going to wake up feeling pretty unrefreshed as all those arousals mean they haven’t got the full benefit of their sleep

We count up all the apnoeas (and hypopneas, when the airflow reduces, but doesn’t stop) and divide it by the total time asleep to give us the apnoea/hypopnea index, a measure of how bad the sleep disordered breathing is

My obstructive apnoea/hypopnoea index is 2.6 events/hr 😳
If I were a child, that’d mean I had obstructive sleep apnoea!
However we expect adults to have a few of these per night, and on adult rating scales, this is completely normal ...
(In children, >10 counts as severe!)
If I were a child, that’d mean I had obstructive sleep apnoea!
However we expect adults to have a few of these per night, and on adult rating scales, this is completely normal ...
(In children, >10 counts as severe!)

The other thing that tells us about airflow is really simple: we assess snoring.
Snoring is the sound that air makes as it flows turbulently through the breathing passages
Snoring is the sound that air makes as it flows turbulently through the breathing passages

As it turns out, I do snore ... 😳
Just under 10% of the night, with 48 snoring episodes. They last less than a minute on average, and the longest one is only 3 minutes ... but even that has earned me a few elbows in the ribs over the years! 😁
Just under 10% of the night, with 48 snoring episodes. They last less than a minute on average, and the longest one is only 3 minutes ... but even that has earned me a few elbows in the ribs over the years! 😁

I even managed to snore loudly enough at one point to partially wake *myself* up 😳
... that’s definitely the sort of behaviour that’s earnt me an elbow in the ribs!
... that’s definitely the sort of behaviour that’s earnt me an elbow in the ribs!

As well as this we’re also looking at the oxygen and carbon dioxide (the gas we breathe in and the waste gas we breathe out) levels.
Mine are fine overall so, annoying as my snoring might be, it’s not having a big effect on the job my lungs are doing as I sleep!
Mine are fine overall so, annoying as my snoring might be, it’s not having a big effect on the job my lungs are doing as I sleep!

One last breathing thing: for first half of the night, I slept on my back, and that’s when most respiratory events were.
Sleeping supine on our back also makes our breathing a bit more vulnerable as adults; on my left, I sleep much quieter (which is the usual goal of the elbow!)
Sleeping supine on our back also makes our breathing a bit more vulnerable as adults; on my left, I sleep much quieter (which is the usual goal of the elbow!)

It’s REALLY IMPORTANT though to remember the opposite is true for babies!
For other reasons, they are MUCH safer sleeping on their backs; the “Back To Sleep” campaign significantly cut the number of Sudden Infant Death Syndrome deaths
For other reasons, they are MUCH safer sleeping on their backs; the “Back To Sleep” campaign significantly cut the number of Sudden Infant Death Syndrome deaths
It’s not just breathing that can affect sleep and cause arousals though!
Before Big Ben went silent for a few years, we could regularly see impact of his chimes and *BONG!*s on the quality of sleep of children being studied in our lab
(You can read about it @bmj_latest here)
Before Big Ben went silent for a few years, we could regularly see impact of his chimes and *BONG!*s on the quality of sleep of children being studied in our lab
(You can read about it @bmj_latest here)

And many common medical conditions can lead to arousals and poorer sleep quality: chronic cough, itch, hay fever or pain can all do this, along with many others
Improving sleep often needs some detective work!
Improving sleep often needs some detective work!

There are a few other things that can do it directly from sleep, and limb movements are one of those.
Like snoring, sudden limb movements can just be part of normal sleep
We see them on the EMG leads (and video too if big enough)
Like snoring, sudden limb movements can just be part of normal sleep
We see them on the EMG leads (and video too if big enough)

Occasionally though, like me snoring myself awake, they can trigger an arousal.
Enough of them doing that can really affect sleep quality, and leave you feeling shattered the next day
Enough of them doing that can really affect sleep quality, and leave you feeling shattered the next day
When they occur in particular patterns/sequence, we call these periodic limb movements
These can be normal (I had a few) but if they affect sleep quality they cause Periodic Limb Movement Disorder
Can be difficult to realise you’ve got it; usually needs bed partner to complain!
These can be normal (I had a few) but if they affect sleep quality they cause Periodic Limb Movement Disorder
Can be difficult to realise you’ve got it; usually needs bed partner to complain!
This is where sleep studies help us to work out what’s going on ... and if we identify a specific problem arising from sleep, to treat it.
The foundation of treating any sleep problem though is good attention to core sleep routine and habits
The foundation of treating any sleep problem though is good attention to core sleep routine and habits
Here’s one reason why you shouldn’t sleep with your phone near your bed ... mine was under my pillow last night
At 0630, I woke up, reached for my phone (probably to check the time), was awake for 2-3 minutes ... and then fell back asleep for another 20 minutes!
I don’t really remember doing that...
I don’t really remember doing that...

Phones by beds mean we’re much more likely to check them if we wake in the night ... which can then affect subsequent sleep quality.
And because we may not even remember doing it, we don’t see the problem
So ... phones OUT of bedrooms please!
And because we may not even remember doing it, we don’t see the problem
So ... phones OUT of bedrooms please!

So, that’s a guide to what happens when people have a sleep study, and some of how we interpret and use that information to guide our assessment and treatment
My study had some issues we don’t usually see in the paediatric lab...
My study had some issues we don’t usually see in the paediatric lab...

... we also picked up some sources of interference, which we’ll address before we start seeing patients in the new rooms (one of the reasons why we do test runs with actual sleeping people)

... but otherwise this was a fairly typical example of a study in our lab.

Hope you’ve found at least some of that interesting!
All that’s left to say is ...
All that’s left to say is ...
















