,
21 tweets,
14 min read
Read on Twitter
#WeeklyCardioReview AUGUSTUS trial #NeverTooLate #Apixaban in patients requiring DAPT. Two key aspects to discuss here: 1) Should Apixaban 5mg/BID be the only NOAC used with triple therapy? 2) Time to move to NOAC+Clopidogrel dual therapy? enjoy thread and comment! 😉
Summary: AUGUSTUS RCT 4,614 ppl requiring DAPT (ACS and-or PCI) factorial design: Apixa vs Warfarin (NOAC research question), and ASA vs placebo (triple vs dual tx question) for 6 months. Study powered for bleeding outcomes and had guts to assume no interaction, stay tuned
Major or clinically relevant nonmajor bleeding lower in Apixa vs Warfarin HR 0.69 (0.58-0.81; superiority P<0.001), ASA vs placebo 1.89 (1.59-2.24; placebo superiority P<0.001). Apixa Vs Warfa, and ASA vs placebo similar incidence of ischemic events
Population: AF of any kind with an indication of prolonged OAC + indication for DAPT for 6 months (ACS, PCI or both). Excluded: Severe renal dysf and other OAC indications, prior brain bleed (this population better protected with NOAC if any OAC indicated? 🤔)
Intervention and Comparators: Within 14 days randomized (6 days median), stratified by indication (ACS or PCI). Apixa: 5mg BID, 2.5mg BID if 2 or > of >80 years, weight <60 kg, or creatinine >1.5mg/dl. Anti-vitK INR 2.0-3.0. ASA 81mg OD vs placebo
Outcomes: 6-months 1ry major (very important bleedings) or clinically relevant nonmajor bleeding (hospitalization, medical or Sx intervention, unscheduled clinic visit, change in antithrombotic therapy) as ISTH. 2ry: death+hospitalization and death+ischemic events
Tested 4 interaction between OAC-ASA. Didnt find it, so data analyzed as two diff trials (the power of factorial design), @RenatoDLopes1 had guts 💪 bcause if interaction was there, although factorials are the best to test them, likely underpowered to test them precisely? 🤔
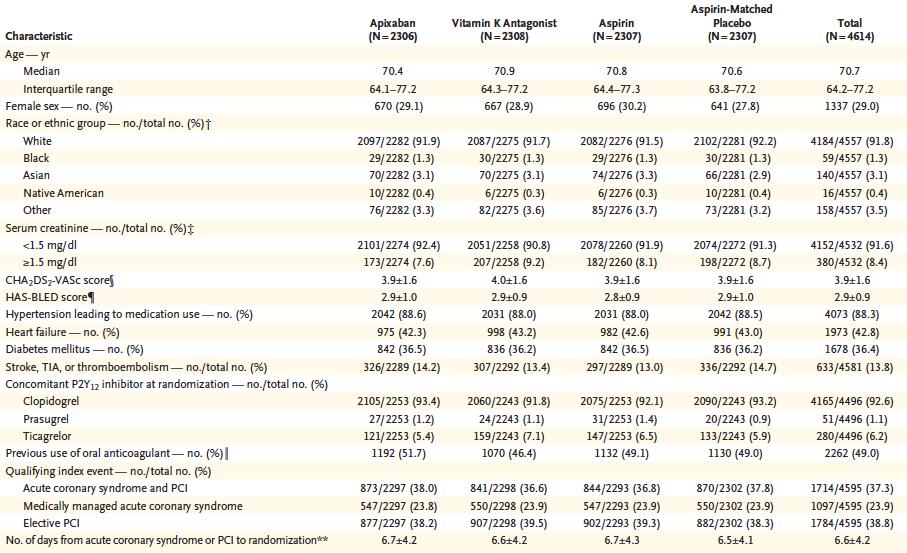
Results: Age 70, 37.3% ACS+PCI, 23.9% MedTx ACS, 38.8% elective PCI. Median CHADSVASc 4 (IQ 3-5), median HAS-BLED 3 (IQ 2-3). Clopidogrel
92.6%, 10.0% received 2.5mg dose. Time in therapeutic range 59%. 12.7% stopped Apixa, 13.8% antivitK 16.9% aspirin and 14.8% stopped placebo
92.6%, 10.0% received 2.5mg dose. Time in therapeutic range 59%. 12.7% stopped Apixa, 13.8% antivitK 16.9% aspirin and 14.8% stopped placebo

1ry outcome bleeding in figures: Apixa superior than AntiVitK, Placebo superior than ASA, and no obvious interaction observed in the last figure, in which Apixa and no ASA lowest risk, and eye-ball steeper benefit dropping ASA than going from AntiVitK to Apixa



Apixa was not associated with increased ischemic events or death, with reasonable 95%CI 0.75-1.16, and reasonable power (154 vs 163 events), lower stroke, while dropping ASA trend in increased ischemic events, in-stent thrombosis and MI


Methods to encourage discussion 1: should we change the wording from constantly calling efficacy=ischemic and safety=bleeding, and adapt to context? if intervention is to drop ASA, efficacy is reducing bleeding, and safety not paying the price of higher ischemic events, agree?
Methods 2: authors say that NNT to avoid bleeding superior to possible NNH dropping ASA supporting dual regimen, but if we take away non-major bleedings and compare mayor bleeding-only vs MI (more comparable events) major bleed 4.7 vs 2.9%, MI 2.9 vs 3.6%, both non-significant...
Same non-statistical trend observed for stent thrombosis. I know that this could be chance, but study underpowered for this patient-important outcomes, and go in the pre-specified direction and is about the safety of a dual regimen, raising concern IMHO rather than reassurance...
Especially because 25% of the patients had no stents placed, and that may be an important diluting factor. On the other hand, Apixaban did not show this trend vs AntiVitK for CV death, MI, stent thrombosis or urgent revasc, with reasonable CIs in some of the individual outcomes
Methods 3: bleeding presented as 100pts/years. The issue I find interpreting is that bleeding hazard not constant over time (highest at the beginning). Look figure 1, around 3/4 of the bleeding events happen within 90 days (1/2 trial), so not very constant and translatable to yrs
U will see that in tables the 100 patient/year estimate is roughly double the absolute 6-month raw %. That is ok if hazard is constant, but here is not the case and after 6 months likely to reach the plateau similar to 90 to 180 days, so 100pts years estimates likely exaggerated
Question 1: is apixaban 5mg/BID the standard when using triple therapy and NOAC preferred? I think yes, given that is the only RCT that did a fair comparison vs triple therapy with AntiVitK with an approved dose for stroke.
Question 2: Is time to move to a dual regimen after PCI and AF? Not IMHO. Unless high-risk of bleeding, think will still recommend no less than a month of triple therapy with NOAC, three to six months if high anatomical risk (bifurcations, LM, etc), then CLOPI + NOAC... opinions?
@threadreaderapp unroll