,
20 tweets,
10 min read
Read on Twitter
I'm going to go outside of my regular comfort zone a bit today, and try out a #tweetorial/#medthread a bit more applicable to #medtwitter in general. So here goes....
A beginner's guide to the use of #PREDNISONE!
#MedEd #FOAMEd #dermtwitter #dermatology PC:@dermnetnz
1/
A beginner's guide to the use of #PREDNISONE!
#MedEd #FOAMEd #dermtwitter #dermatology PC:@dermnetnz
1/
Ah, prednisone. One of the most frequently used drugs in our specialty, and in many across the board in medicine. Useful for quick suppression of an overactive immune system, whether that be because of autoimmunity, or acute infection. But how does it work?
2/
2/
The point is that there are so many potential mechanisms, that it's hard to point at one particular enzyme or pathway to explain all its effects. This paper address many of them, but my main takeaway is that we don't know everything! ncbi.nlm.nih.gov/pmc/articles/P…
3/
3/

But what do we need to remember? The many side effects of course! While there are certainly a ton, these are the few I always harp on:
- Increased risk of infection
- Effect on soft tissues (including bone and skin)
- Effects on BP, blood sugar, mood, gut
4/
- Increased risk of infection
- Effect on soft tissues (including bone and skin)
- Effects on BP, blood sugar, mood, gut
4/
So let's talk about infection. In residency, I was taught to start prophylaxis for pneumocystis by the "20 x 20 rule" (20 mg for >20 days). Since then, I've come to realize that's probably too aggressive. Everyone has a different rule, what's yours?
5/
5/
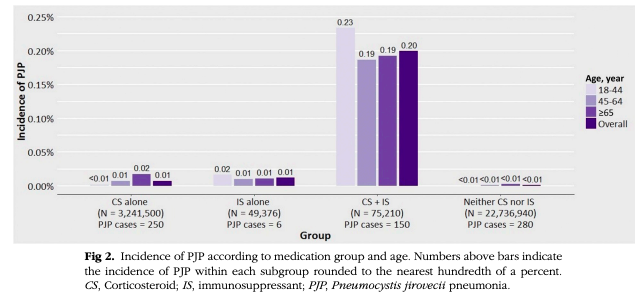
Let's go to the literature! From a #derm POV, this study (jaad.org/article/S0190-…) found that the incidence of PCP pneumonia was increased mainly in the group that received steroids WITH another immunosuppressant. While still low, they argue the bad effect of PCP warrants ppx.
6/
6/
So that is my practice - to start PCP ppx when my pts are on combination immunosuppression. & despite my dermatology training that's beaten the terrors of TMP-SMX into me, I still use it for this (I like SS daily). But that's just me! Other's may do something different!
7/
7/
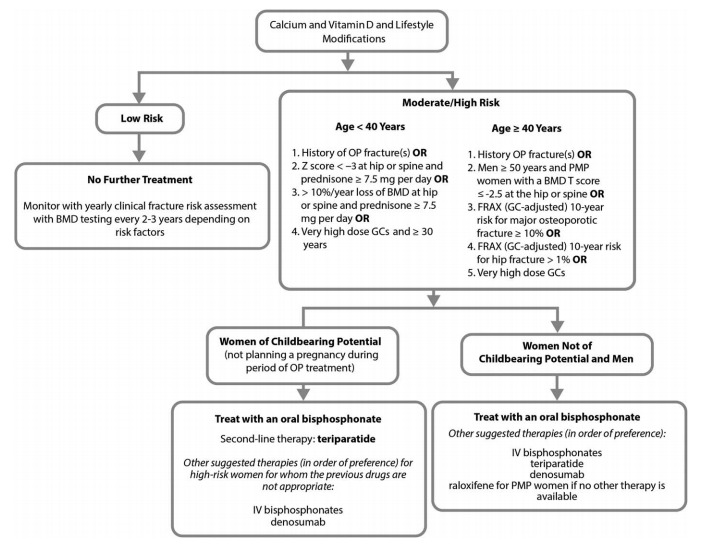
What about the effect on bone health? This is a complicated topic so I'm going to discuss the general principles here. Anyone who is going to get a "prolonged course" of prednisone (usually meaning >3 mo) gets Calcium (>1200 mg) and Vit D (>800 IU). I may get a BMD as well.
8/
8/
Pts with a high risk of fracture likely will need a bisphosphonate with their steroid therapy. I usually use alendronate. That said, the guidelines are rather dense and complicated. If you're up for a nice bedtime read, take a gander here: rheumatology.org/Portals/0/File…
9/
9/
What about the psychiatric effects? Prednisone seems to be able to cause insomnia, delirium, mania at almost any dose, and I'm certainly more cautious in the elderly. That said, true psychosis seems to occur with doses in excess of 20 mg daily.
10/
10/
GI effects are magnified with concurrent NSAID usage. I don't routinely ppx for GI issues like gastritis, but will often warn my patients about it so that I know to start an acid medication when necessary. Don't forget more serious effects like bowel perforation can occur!
11/
11/
And let's chat about blood sugar. We know prednisone can increase blood sugar in a dose dependent way, but for a patient to develop diabetes from prednisone is really uncommon. That said, diabetics on prednisone can see a magnified effect!
12/
12/
Combined with the glucose effect, we should think about the CV effects as well. We know of the fluid retention that prednisone can cause, but arrythmias, potential hyperlipidemia, and independent atherosclerotic disease are all possible! The list just keeps going!
13/
13/
& this wouldn't be a proper #dermtwitter #tweetorial w/o a tweet about the skin effects. Stretch marks (pic1), easy bruising (pic2), fragile skin (pic3) & steroid acne (pic4) are all typical of prolonged prednisone usage!
(Steroid acne looks different b/c it's monomorphic!)
14/
(Steroid acne looks different b/c it's monomorphic!)
14/




And while weight gain usually is limited to those over 5 mg/day doses for a long time, the cushingoid effects (buffalo hump, moon facies) can be seen at any dose after a while.
Notably, the weight gained is really hard to lose (at least in my patients' experience)!
15/
Notably, the weight gained is really hard to lose (at least in my patients' experience)!
15/

There's obviously more, but lets move on to how we dose it!
Everyone's different, but depending on the diagnosis, I'm reaching for a different dose.
Things like DRESS will usually require 1mg/kg/day of prednisone, whereas things like contact dermatitis might need less.
16/
Everyone's different, but depending on the diagnosis, I'm reaching for a different dose.
Things like DRESS will usually require 1mg/kg/day of prednisone, whereas things like contact dermatitis might need less.
16/
So when I start it, I'm asking the pt about their comorbidities, taking their age & other issues into account, and coming up with a plan that seems appropriate to them. They all get our direct number in case an issue arises so we can troubleshoot over the phone if possible.
17/
17/
And let's talk about our patients on a long slow taper. Once they get to 5 mg, I'm going very slowly out of concern for adrenal insufficiency. I'm not doing a cort-stim on these pts. I advise them of the sxs to expect. If they get them, I just bump the pred back up to 5.
18/
18/
And I'll end on my favorite mnemonic from residency:
H&P to the MD: 20, 5, 4, 1.
Hydrocortisone 20 mg =
Prednisone 5 mg =
Methylprednisolone 4 mg =
Dexamethasone 1 mg
Great for (approximately) converting doses!
19/
H&P to the MD: 20, 5, 4, 1.
Hydrocortisone 20 mg =
Prednisone 5 mg =
Methylprednisolone 4 mg =
Dexamethasone 1 mg
Great for (approximately) converting doses!
19/
I hope this was helpful! Apologies this may have been #dermatology centric! To recap:
- Caution with prednisone!
- PCP ppx with dual immunosuppression (which is what I do).
- Slow slow taper to avoid adrenal insufficiency.
- Check out guidelines for detailed protocols!
20/20
- Caution with prednisone!
- PCP ppx with dual immunosuppression (which is what I do).
- Slow slow taper to avoid adrenal insufficiency.
- Check out guidelines for detailed protocols!
20/20