1/ #ListenThread -
My guest appearance on #SigmaNutritionRadio just dropped where I have a very friendly #debate with @NutritionDanny and Alan Flanagan on #LDL #Cholesterol, #ApoB, #Atherosclerosis, #AllCauseMortality & much, much more!
sigmanutrition.com/episode321/
My guest appearance on #SigmaNutritionRadio just dropped where I have a very friendly #debate with @NutritionDanny and Alan Flanagan on #LDL #Cholesterol, #ApoB, #Atherosclerosis, #AllCauseMortality & much, much more!
sigmanutrition.com/episode321/
2/ I did this podcast semi-sleep deprived and between interviews for #TheCCDoc. But I know my main hopes going in were to emphasize:
(1) Why I favor the "Lipid profile-centric" model over the "Lipoprotein-centric" model.
(2) How this is relevant to "the triad" ⬆️LDL⬆️HDL⬇️TG
(1) Why I favor the "Lipid profile-centric" model over the "Lipoprotein-centric" model.
(2) How this is relevant to "the triad" ⬆️LDL⬆️HDL⬇️TG
3/
(3) Why this triad is of particular interest to all of us as it relates to not just cardiovascular disease, but in particular -- all cause mortality (ACM)
I honestly couldn't remember how well I did in getting these core points across, thus relistening now...
(3) Why this triad is of particular interest to all of us as it relates to not just cardiovascular disease, but in particular -- all cause mortality (ACM)
I honestly couldn't remember how well I did in getting these core points across, thus relistening now...
4/ 0:00 @NutritionDanny sets up the episode well.
Discussing the triad, points to myself as a key contributor to raising interest in it (particularly in the #LowCarb community)
However, there is one characterization I'd disagree with, but the assumption is understandable...
Discussing the triad, points to myself as a key contributor to raising interest in it (particularly in the #LowCarb community)
However, there is one characterization I'd disagree with, but the assumption is understandable...
5/ 2:50 "... or that this triad (⬆️LDL+⬆️HDL+⬇️TG) doesn't confer a high risk of cardiovascular disease (CVD), or at least doesn't have a higher risk when compared to one with a lower LDL."
6/ Technically, I agree it is low risk for CVD, but have to revisit whether same (or lower) to low LDL in relative terms. But I think we get into that in the podcast and I hopefully address that distinction....
7/ 4:15 @NutritionDanny compliments me as having conducted myself in a very civil manner and points out it is rare in the nutrition space.
I certain want to emphasize that I felt likewise with both Danny and Alan. They were extremely professional and very courteous.
I certain want to emphasize that I felt likewise with both Danny and Alan. They were extremely professional and very courteous.
8/ If you take only one thing from this podcast, you can disregard all the biggest points I make and just hold on to the importance of civil and productive debate. This podcast was truly a model example, IMO.
9/ 8:25 Danny lets me set up and kick off the discussion.
(a) I intro "Atherogenic Dyslipidemia" (⬇️HDL+⬆️TG+⬆️sdLDL)
(b) Many going #LowCarb see the reverse of this, which is what I usually refer to when I say "triad" (⬆️LDL+⬆️HDL+⬇️TG)
(a) I intro "Atherogenic Dyslipidemia" (⬇️HDL+⬆️TG+⬆️sdLDL)
(b) Many going #LowCarb see the reverse of this, which is what I usually refer to when I say "triad" (⬆️LDL+⬆️HDL+⬇️TG)
10/ 10:40 I get into distinguishing the "lipoprotein-centric" model vs the "lipid profile-centric" model.
Aside: Really, really glad I did this right off the bat. This is so incredibly key to understanding where I'm coming from and the concept of "systemic atherogenicity"
Aside: Really, really glad I did this right off the bat. This is so incredibly key to understanding where I'm coming from and the concept of "systemic atherogenicity"
11/ 11:40 I quote Alan from the last podcast in his comment that the objections raised by myself and others are "...that all the nuances they put forward are inherently accounted for in the totality of the evidence base."
(This is certainly something I strongly disagree with)
(This is certainly something I strongly disagree with)
12/ 12:00 I ask on Alan's example of inflammation in the last podcast where he points to studies where they stratify for low CRP and find lowering LDL to be beneficial for heart disease risk, and he points to the recent study by Storey...
Possibly this?: ncbi.nlm.nih.gov/pubmed/29146277
Possibly this?: ncbi.nlm.nih.gov/pubmed/29146277
14/ 19:20 — I bring in the distinction of looking at LDL vs ApoB — which, btw, I cover in this thread here as well:
15/ Me --> "And thus the easy way to determine if ApoB is independently atherogenic is to subtract remnants to determine how much LDL particle count actually plays a part in it. And this is one of the advantages of looking at triglycerides especially..."
16/ ... "If triglycerides are low, but there's very high ApoB, there's probably very low remnants because of course they tend to be very triglyceride-rich."...
17/ ... "And that's why a lot of the stratifications I've been doing, especially with NHANES, was to take ApoB -- particularly high levels of ApoB -- but against this triad of high HDL and low triglycerides."
"And what I find is quite astonishingly against all cause mortality.."
"And what I find is quite astonishingly against all cause mortality.."
18/ ... "It's the reverse of what you'd expect it would be. A very low ApoB, yet high HDL and low triglycerides tend to have worse mortality outcomes than those with very high ApoB and high HDL and low triglycerides."
19/ ... "...the best combination of those three markers are not actually just high HDL and low triglycerides, but specifically *high* ApoB as opposed to *low* ApoB, at least as far as the association goes."
20/ If I can pause for a moment -- I'm really glad I laid that out.
This association I'm discussing above is effectively unaddressed. It is assumed to be "reverse causality", but without supporting evidence to that assertion, which we could easily obtain via longitudinal data...
This association I'm discussing above is effectively unaddressed. It is assumed to be "reverse causality", but without supporting evidence to that assertion, which we could easily obtain via longitudinal data...
21/ Yet it's an inescapable reality that at every point I've come to thus far where I can look at a age-paritied, unadjusted head count on the triad vs any other combination lipid profile, it associates with longevity -- and this includes low LDL vs high LDL in the same context.
22/ While I bring this up often, I'm never sure if it is more my not articulating it well or simply not emphasizing it enough that results in it being passed by so many on the pro LDL-lowering side of the divide.
Again (as always), I welcome further nuance and rebuttal...
Again (as always), I welcome further nuance and rebuttal...
23/ But at the end of the day, if I tell you the raw data supports those with high LDL where matched with their age groups of low LDL will be clocking in as "alive" in 10 or 15 years in greater proportions, you'd likely care about that.
At a minimum, you'd want to know why.
At a minimum, you'd want to know why.
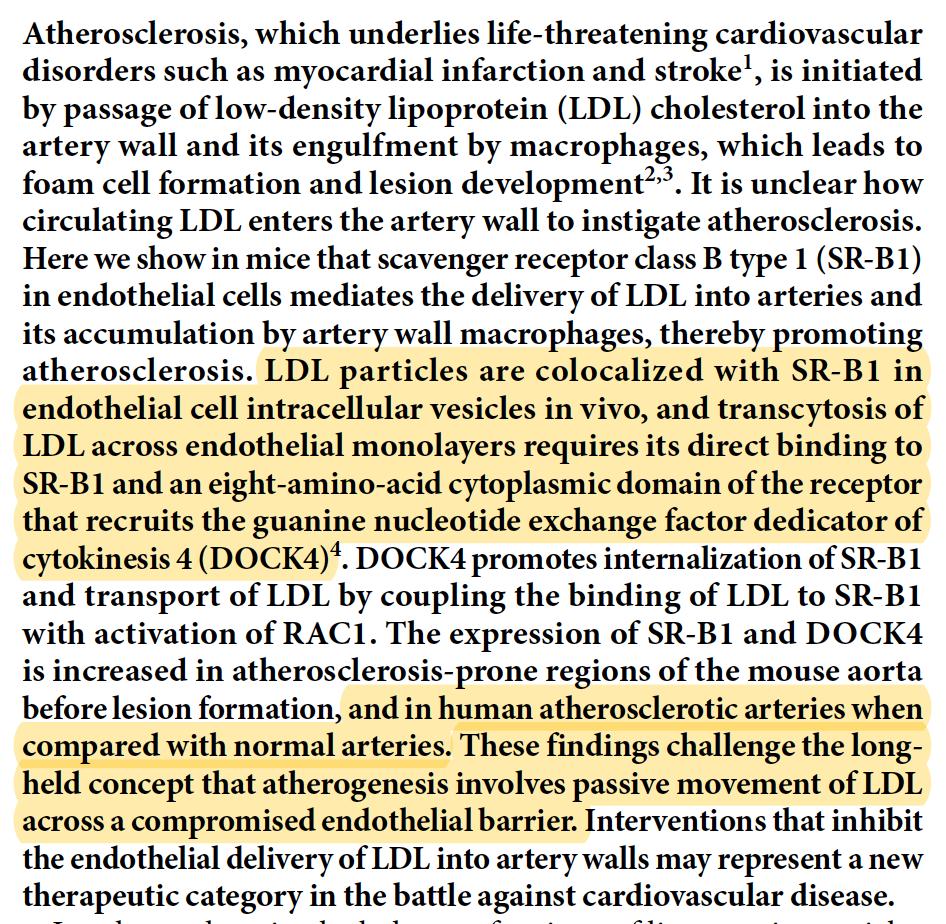
24/ 21:50 — I also discuss how there are other ways in which LDL particles gain entry into the subintimal space, including transcytosis and as potentially in part where there is a site of inflammation during which junctions between endo cells become intentionally porous
25/ But to be fair, I think I misunderstood Alan's original point in that he was discussing how LDL particles *leave* the extracellular space (catching it on the re-listen).
(Though I am glad I still discussed the other common means of entry anyway, as is relevant to athero)
(Though I am glad I still discussed the other common means of entry anyway, as is relevant to athero)
26/ 23:50 - Alan discusses HDL and how interventions to alter haven't translated to clear benefit.
27:50 I follow up discussing how well this fits in with the lipid profile-centric vs lipoprotein-centric models, discussing CETPi, and why I think it was a poor outcome...
27:50 I follow up discussing how well this fits in with the lipid profile-centric vs lipoprotein-centric models, discussing CETPi, and why I think it was a poor outcome...
27/ ... I go on to describe why modifying packets in a network would be analogous, but I'm not sure if I did a good job on that given we were already well into Geek Territory by that point.
28/ 30:50 - I get into the Framingham Offspring study with regard to the Odds Ratio on CVD comparison.
But I also mention how I wish they would've captured and reported All Cause Mortality.
ahajournals.org/doi/full/10.11…
But I also mention how I wish they would've captured and reported All Cause Mortality.
ahajournals.org/doi/full/10.11…
29/ 32:10 - I then discuss the Jeppesen study showing high relevance to HDL+TG and low relevance to LDL when combining all three for comparison.
ncbi.nlm.nih.gov/pubmed/11176761
ncbi.nlm.nih.gov/pubmed/11176761
30/ 33:24 -- here I begin talking about why All Cause Mortality (ACM) is super relevant when considering how LDL particles are participants in the immune response.
This is an extremely critical consideration to the larger question of risk and the lipid profiles themselves...
This is an extremely critical consideration to the larger question of risk and the lipid profiles themselves...
31/ "I have a long list of studies [with regard to the immune response]..."
Important to emphasize right now that my long list is due to the tireless work of @siobhan_huggins and easily one of the best reads on this topic found at our site here: cholesterolcode.com/lipoprotein-po…
Important to emphasize right now that my long list is due to the tireless work of @siobhan_huggins and easily one of the best reads on this topic found at our site here: cholesterolcode.com/lipoprotein-po…
@siobhan_huggins 32/ 33:53 — Ack! I misspeak here and call alpha tocopherol “vitamin D” when it is of course “vitamin E”. But given my follow up on ROS, etc, it’s pretty clear what I meant.
Still... this deserves three facepalms 🤦♂️🤦♂️🤦♂️
(Note to self: stop guesting while sleep-deprived)
Still... this deserves three facepalms 🤦♂️🤦♂️🤦♂️
(Note to self: stop guesting while sleep-deprived)
@siobhan_huggins 33/ 34:23 - Alan correctly points out with the Framingham Offspring that the lower LDL had a lower relative OR (which is the case -- 0.6 for LDL < 100 vs 0.7 for both LDL ≥ 100 and LDL ≥130)
And this is a key point we should return to later and why I wanted to see ACM as well.
And this is a key point we should return to later and why I wanted to see ACM as well.
@siobhan_huggins 34/ 39:12 — After listening to Alan’s last point, I restate his position to see if I’m understanding it accurately with regard to LDL conferring risk in any context toward all cause mortality. And he agrees, yes, it is independently causal toward risk...
35/ Me -- "You'd feel LDL is kind of like smoking. In the sense that whatever two groups [you compared], even if one group is healthier in having a higher HDL and lower triglyceride -- that said, comparing that group with low LDL that's identical in virtually every other way..."
36/ "... The first group is at lower risk, overall. Towards death, period. Towards all cause mortality."
Alan - "Yes, that's what I'm saying..."
This is important, because it's a very clear divide in our hypotheses for outcomes...
Alan - "Yes, that's what I'm saying..."
This is important, because it's a very clear divide in our hypotheses for outcomes...
37/ Which relates again to the longevity point I make above.
Again, I'm happy we covered this coming at it from a different direction, but getting back to the same central point.
Again, I'm happy we covered this coming at it from a different direction, but getting back to the same central point.
38/ So to state it simply:
Will we generally see those with ⬆️LDL+⬆️HDL+⬇️TG generally live longer than those ⬇️LDL+⬆️HDL+⬇️TG?
-Me, I think that's what we'll see
-Alan would expect we'd see the opposite
So far, NHANES appears to support this, but we need more data to compare
Will we generally see those with ⬆️LDL+⬆️HDL+⬇️TG generally live longer than those ⬇️LDL+⬆️HDL+⬇️TG?
-Me, I think that's what we'll see
-Alan would expect we'd see the opposite
So far, NHANES appears to support this, but we need more data to compare
39/ 40:10 Me:
"I would actually agree with you if that's what the evidence showed....That basically if we could look at high and low LDL in every possible cohort group at scale and it shows that those people with high LDL are dying more than those likewise cohorts of low LDL..."
"I would actually agree with you if that's what the evidence showed....That basically if we could look at high and low LDL in every possible cohort group at scale and it shows that those people with high LDL are dying more than those likewise cohorts of low LDL..."
40/ "... Then it's comparable to smoking. That you're just better off having lower LDL."
Alan: "But to my mind, that's what the Framingham Offspring study somewhat showed in terms of risk. I know mortality wasn't an outcome if I remember correctly..."
Alan: "But to my mind, that's what the Framingham Offspring study somewhat showed in terms of risk. I know mortality wasn't an outcome if I remember correctly..."
41/ Me: "No, it shows it with cardiovascular disease, and that's the 'what' you die of, not the 'when'. So looking at a particular stratification of a particular outcome is not something I'm as interested in as I am in all cause mortality."
42/ From here we dive deeper into All Cause Mortality as Alan wants me to expand on it further.
- I discuss comparisons with LDL vs smoking when looking at likewise cohort outcomes with ACM
- How I was looking at the beginning with LDL assoc with longevity
- I discuss comparisons with LDL vs smoking when looking at likewise cohort outcomes with ACM
- How I was looking at the beginning with LDL assoc with longevity
43/
- Is it reverse causation? But I couldn't find any studies that showed a longitudinal change given a long enough duration of exclusion, for example.
- I mention the Framingham 18 year assoc with low LDL and cancer onlinejacc.org/content/59/13_…
- Is it reverse causation? But I couldn't find any studies that showed a longitudinal change given a long enough duration of exclusion, for example.
- I mention the Framingham 18 year assoc with low LDL and cancer onlinejacc.org/content/59/13_…
44/ "... And this is why I brought up immunity, and the immune response, and how much LDL is associated with it and what there already is in the literature..."
45/ "If we look only at how you can die of one particular disease, then we have to feel confident that that intervention or that change isn't affecting other possible endpoints, other possible ways one can die..."
46/ "...And I don't think we're anywhere close to determining how much lipoproteins -- especially LDL -- has engagement with the immune response. And the immune response touches almost all major diseases."
47/ [Now pausing for a break as I'll be interviewing @FatEmperor for #TheCCDoc and need to do some prep, etc
I'll return to this thread in a bit... crazy to think I'm only through 46m with still 72m to go!]
I'll return to this thread in a bit... crazy to think I'm only through 46m with still 72m to go!]
48/ 46:11 — Me: “To steel man argument this, I think you and Alan would rightly say, ‘okay, whatever evidence is out there that does show [the triad associates with below average CVD risk], it is still in *relative terms* higher than a likewise cohort that has lower LDL chol.”...
49/ Danny: “Correct, correct, right”
Me: “And this is where I have to say this, and I don’t say this to be contrarian, but here’s the one problem. The one problem is saying that you’re dying less of Disease X is exactly equivalent to I’m dying more of Disease Non-X.”
Me: “And this is where I have to say this, and I don’t say this to be contrarian, but here’s the one problem. The one problem is saying that you’re dying less of Disease X is exactly equivalent to I’m dying more of Disease Non-X.”
50/ “So we have to be able to determine — and it’s hard to do — that those things a population is dying of that is not Disease X didn’t change timelines on us, didn’t possibly move up in timelines, does that make sense?”
(Not my best articulation, but hopefully got the gist 😂)
(Not my best articulation, but hopefully got the gist 😂)
51/ I’m worried listening up to this point in the podcast that I might not have pressed on the specific aspects of LDL that are relevant toward consideration of benefit from the immune perspective and probably should’ve approached that at a more basic level earlier on.
52/ 47:58 I’m clarifying regard to LDL involvement in atherosclerosis while also pointing to other immune agents such as macrophages...
53/ Me: “The question isn’t whether they are a part of the process, the question is whether they are the initiator of the process and/or... they are the progressor of the process.”
54/ “And that’s the key distinction we’re kind of breaking down... This predates us by a lot, this goes back to the 70s. Is this Response to Retention, or is this Response to Injury?”
“I certainly feel I’m leaning much more into the camp of Response to Injury...”
“I certainly feel I’m leaning much more into the camp of Response to Injury...”
55/ “You guys would say you’re leaning much more toward the Response to Retention, would that be accurate?”
Alan: “Personally, I feel that’s too crude a delineation. I’ve seen those arguments of [RtI vs RtR], and for the biological systems we’re talking about...”
Alan: “Personally, I feel that’s too crude a delineation. I’ve seen those arguments of [RtI vs RtR], and for the biological systems we’re talking about...”
56/ Alan goes on to point to his feeling it is indeed both, technically speaking.
“Retention is a big part of the process, sure, but so too is the initial injury.”
“Retention is a big part of the process, sure, but so too is the initial injury.”
57/ 51:26 Alan: “When we look at populations above 65, 70, 75 — which is where I see uniformly the idea of LDL being protective or associated with longevity comes from. Populations that have already gotten to that stage.”
58/ Alan: “We’re then taking a snapshot at that point at that life stage and saying this relates. There’s two issues for me with that. One is that it doesn’t speak to levels over the course of a lifetime. Two, what we know about... all chronic lifestyle diseases...”
59/ Alan: “...particularly cardiovascular disease is that it is the cumulative life long exposure, and this is point we were really going out of our way to make with the Sigma Statements. It’s not that you have a steak and your LDL goes through the roof.”
60/ Alan: “It’s a cumulative integrated exposure over the course of a lifespan...” He discusses evidence showing early atherosclerosis from studies young soldiers in Vietnam and Korea.
61/ Alan: “So I think a problem when you start to look at populations that are 70 plus is that for the most part people have atherosclerotic cardiovascular disease are going to be in and around about dead by then, for the most part.”
62/ Alan minutes later: “... The data that [skeptics] use to show that there’s a lack of a net benefit to lowering LDL is also in this age demographic. They’re generally studies in the 60s, 70s, 75 plus where... interventions to lower risk are not necessarily that effective.”
63/ Alan: “But that’s a reflection of this cumulative lifelong exposure. And it’s a reflection of the fact that cardiovascular disease is already so advanced, that the net benefit of treatment at that stage is essentially too little too late.”
64/ I want to pause here and discuss this specific point Alan is making because it may be our single largest difference with regard to mechanistic expectation.
While I did transcribe a lot of this above, I’d want you to instead listen to the actual podcast for full context.
While I did transcribe a lot of this above, I’d want you to instead listen to the actual podcast for full context.