All right #dermtwitter & #medtwitter, it's time for the...
@MedDermSoc & @DermHospitalist Mini-Symposium on #COVID19 & #dermatology!!
I will be attempting to #livetweet the Zoom meeting!
Join along if you'd like. I will be using the h/t #COVIDDerm!
@RoxanaDaneshjou @dschless
@MedDermSoc & @DermHospitalist Mini-Symposium on #COVID19 & #dermatology!!
I will be attempting to #livetweet the Zoom meeting!
Join along if you'd like. I will be using the h/t #COVIDDerm!
@RoxanaDaneshjou @dschless
Let's get started!!!!
Your cohosts are super excited to have you join. To give a little background, this meeting was planned in ~1 week, and we have over 500 RSVPs!
@MishaRosenbach now kicking us off with #COVIDDerm!
Your cohosts are super excited to have you join. To give a little background, this meeting was planned in ~1 week, and we have over 500 RSVPs!
@MishaRosenbach now kicking us off with #COVIDDerm!

.@DrEstherFreeman is speaking and reminding us all to register our #COVID19 #dermatology cases in the @AADskin #COVID registry!
Reminder to do so here:
aad.org/covidregistry
#COVIDDerm
Reminder to do so here:
aad.org/covidregistry
#COVIDDerm
Next up, we will be discussing skin signs of #COVID19. Doctors Joanna Harp, Helena Pasieka, and Lindy Fox will be presenting!
Powerhouse of #dermatologists!
#COVIDDerm
Powerhouse of #dermatologists!
#COVIDDerm
Dr. Helena Pasieka from @Georgetown and @MedStarWHC is discussing published cases thus far, which include:
#COVID Toes
Urticaria
Morbilliform
Vesicular rash
Livedo reticularis
and more!
#COVIDDerm
#COVID Toes
Urticaria
Morbilliform
Vesicular rash
Livedo reticularis
and more!
#COVIDDerm
Only 0.2% of patients of #COVID19 patients in China were reported to have any #dermatologic manifestation.
Once the disease hit Italy, we saw our first report because #dermatologists were redeployed to the front lines which allowed for better characterization.
#CovidDerm
Once the disease hit Italy, we saw our first report because #dermatologists were redeployed to the front lines which allowed for better characterization.
#CovidDerm
No photos were allowed in this paper by recalcati et al because phones weren't allowed.
18/88 patients (~20%) had a skin manifestation.
Here's the paper: joidairouso.com/bb/img/207_2.p…
#COVIDDerm
18/88 patients (~20%) had a skin manifestation.
Here's the paper: joidairouso.com/bb/img/207_2.p…
#COVIDDerm
Soon thereafter, #COVIDToes began getting reported by Italian dermatologists via Whatsapp.
Later on, a case series from Wuhan showed 7 critically ill COVID19 patients with distal ischemia (much more severe than just the toes, with frank necrosis).
#COVIDDerm
Later on, a case series from Wuhan showed 7 critically ill COVID19 patients with distal ischemia (much more severe than just the toes, with frank necrosis).
#COVIDDerm
This paper from @JAADjournals further helps synthesize all the published material. Basically breaks down #COVID19 rash down to those that are:
1 - virally mediated
2 - consequence of drug or other systemic disease
#COVIDderm
jaad.org/article/S0190-…
1 - virally mediated
2 - consequence of drug or other systemic disease
#COVIDderm
jaad.org/article/S0190-…
HOT OFF THE PRESSES!
A Spanish paper with prospective data!
47% "maculopapules"
19% covid toes
9% vesicular (small monomorphic)
6% livedo or necrosis
19% urticarial
also - sickest patients had livedo, & most mild cases were pseudochilblains. maculopapules in btw.
#COVIDDerm
A Spanish paper with prospective data!
47% "maculopapules"
19% covid toes
9% vesicular (small monomorphic)
6% livedo or necrosis
19% urticarial
also - sickest patients had livedo, & most mild cases were pseudochilblains. maculopapules in btw.
#COVIDDerm
Now we're going to focus in on #covidtoes with @lindyfox1 for our #COVIDDerm symposium!
Could this be thrombotic? vasculitic? inflammatory? some mixed picture?
This paper from @JAADjournals is referenced, with mean duration of rash to be 8.7 days.
jaad.org/article/S0190-…
Could this be thrombotic? vasculitic? inflammatory? some mixed picture?
This paper from @JAADjournals is referenced, with mean duration of rash to be 8.7 days.
jaad.org/article/S0190-…
#covidtoes can be papular, vesicobullous, some without even erythema.
Notably, #COVID19 PCR was negative in the majority of those tested (very few tested). This was the case in 3 case series being presented.
#covidderm
Notably, #COVID19 PCR was negative in the majority of those tested (very few tested). This was the case in 3 case series being presented.
#covidderm
#dermatopathology from #covidtoes from @JAADjournals seems to not show any frank LCV or thrombosis, but rather just lymphocytic vasculitis.
Seems to look like regular pernio, per @lindyfox1.
#COVIDDerm
Seems to look like regular pernio, per @lindyfox1.
#COVIDDerm
Summary from @lindyfox1
#covidtoes seem to be:
- in young healthy patients
- CAN have respiratory/other sxs
- Seems to be a later finding. Can have +PCR, but usually not. Should we worry about infectious poss?
- Most Ab testing has been negative
#COVIDDerm
#covidtoes seem to be:
- in young healthy patients
- CAN have respiratory/other sxs
- Seems to be a later finding. Can have +PCR, but usually not. Should we worry about infectious poss?
- Most Ab testing has been negative
#COVIDDerm
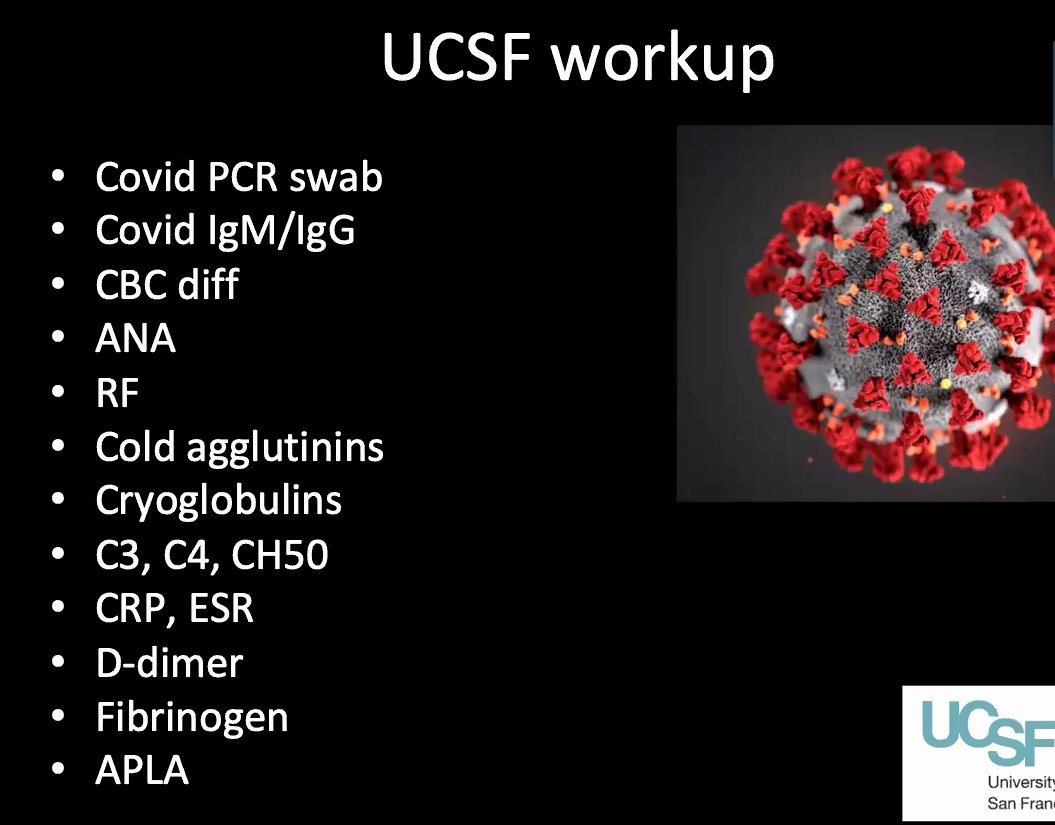
Work up for #covidtoes at @UCSF #dermatology below.
My personal take: I might avoid sending the entire work up if it's not going to change management.
HOWEVER - if it affects a patient's ability to return to work, or potentially donate plasma etc, I might send more.
#COVIDDerm
My personal take: I might avoid sending the entire work up if it's not going to change management.
HOWEVER - if it affects a patient's ability to return to work, or potentially donate plasma etc, I might send more.
#COVIDDerm
All pts at @UCSF #dermatology have been pcr negative after presenting with #covidtoes.
Some patients seem to have disease course that is much longer than the published ~9-13 days.
#COVIDDerm
Some patients seem to have disease course that is much longer than the published ~9-13 days.
#COVIDDerm
Since Ab testing has been negative in most cases of #covidtoes, this means that perhaps these patients aren't even truly getting immunity despite potentially getting infected by #covid19!
#COVIDDerm
#COVIDDerm
Moving to Dr. Joanna Harp from @WeillCornell to discuss #dermatology and #COVID19 in the inpatients who are unfortunately afflicted with a much more severe case of #COVID!
#COVIDDerm
#COVIDDerm
In the sicker #COVID19 patient population, not seeing #covidtoes. Morbilliform eruption is late and likely from drugs.
Instead, acral livedo racemosa has been the most frequent finding!
#COVIDDerm
Instead, acral livedo racemosa has been the most frequent finding!
#COVIDDerm
Almost all of the acral livedo racemosa patients had a rash appear after being ventilated for over a week!
Skin bx was performed in 6 pts. all 6 had a pauci-inflammatory thrombogenic vasculopathy.
4/6 had arterial thrombosis!
3 of 4 died from thrombosis! (Stroke, PE)
#COVIDDerm
Skin bx was performed in 6 pts. all 6 had a pauci-inflammatory thrombogenic vasculopathy.
4/6 had arterial thrombosis!
3 of 4 died from thrombosis! (Stroke, PE)
#COVIDDerm
All these patients with livedo racemosa acrally had very high D-Dimers, most (5/6) had coagulopathy!
Perhaps this skin finding can help warn about soon to come coagulopathy!
#medtwitter #dermtwitter #COVIDDerm
Perhaps this skin finding can help warn about soon to come coagulopathy!
#medtwitter #dermtwitter #COVIDDerm
These thrombotic processes seem to occurring a lot acrally and on the buttocks.
This fits with the many thrombotic complications seen on autopsy, and all the clotting seen by the intensivists and #hospitalists!
Notably, these aren't patients going into DIC.
#COVIDDerm
This fits with the many thrombotic complications seen on autopsy, and all the clotting seen by the intensivists and #hospitalists!
Notably, these aren't patients going into DIC.
#COVIDDerm
Proposed mechanisms for this thombotic process:
- ?complement activation and deposition
- ?endothelial cell infection and endotheliitis
- ?antiphospholipid?
#COVIDDerm
- ?complement activation and deposition
- ?endothelial cell infection and endotheliitis
- ?antiphospholipid?
#COVIDDerm
Take home points from #inpatient #COVID19 #dermatology care by Dr. Joanna Harp:
- livedoid pattern may likely be a manifestation of systemic coagulopathy, especially if high d-dimer
- partner with #hematology, especially re: anticoagulation
#COVIDDerm
- livedoid pattern may likely be a manifestation of systemic coagulopathy, especially if high d-dimer
- partner with #hematology, especially re: anticoagulation
#COVIDDerm
Now moving to urgent #dermatology consults by Drs. Rob micheletti from @PennMedicine and Dr. John Trinidad from @OhioStateMed!
#COVIDDerm
#COVIDDerm
When urgent #dermatology consults are required, important to think about whether we can do something through #telemedicine in hopes of preserving PPE & minimizing risk
Need to have ongoing dialogue with primary teams to make sure they understand our changed workflows
#COVIDDerm
Need to have ongoing dialogue with primary teams to make sure they understand our changed workflows
#COVIDDerm
@OhioStateMed, inpatient derm is joined virtually by residents & faculty to improve educational offerings!
Important to recognize that in-person evaluation is the gold standard.
#telemedicine has made in person eval much more efficient, making it easier to plan.
#COVIDDerm
Important to recognize that in-person evaluation is the gold standard.
#telemedicine has made in person eval much more efficient, making it easier to plan.
#COVIDDerm
For inpt #teledermatology, need to think about ethical considerations to make sure we are still providing the best care.
Also need to think about billing! Unclear if time spent on the consult (even not face to face) is the only factor for billing. Good to keep track.
#COVIDDerm
Also need to think about billing! Unclear if time spent on the consult (even not face to face) is the only factor for billing. Good to keep track.
#COVIDDerm
As non #COVID19 patients return, we're expecting inpatient #dermatology consults to pick up and become higher in volume! A lot of our "normal" consults are not happening b/c hospitals have been emptied out for #COVID. A wave may be coming! Get ready @DermHospitalist!
#COVIDDerm
#COVIDDerm
Next up: @JosephMerolaMD will be discussing management of #immunosuppression for our #dermatology patients in the setting of #COVID19!
Most importantly - lack of data! So a lot of judgement is required!
#COVIDDerm
Most importantly - lack of data! So a lot of judgement is required!
#COVIDDerm
We are extrapolating our safety discussion from clinical trials, other viral epidemics, and #COVID19 specific data.
Important to have shared decision making process.
#COVIDDerm
Important to have shared decision making process.
#COVIDDerm
Things to consider when thinking about immunosuppression:
- severity of underlying condition
- potential need for emergency care increasing risk of exposure if stopping immunosuppression.
- job exposures
- need for lab monitoring
- relative level of immunosuppression
#COVIDDerm
- severity of underlying condition
- potential need for emergency care increasing risk of exposure if stopping immunosuppression.
- job exposures
- need for lab monitoring
- relative level of immunosuppression
#COVIDDerm
Remember that when managing immunosuppression, our patients already have an increased baseline risk of infection with their underlying disease processes! So truly a risk benefit discussion!
#COVIDDerm
#COVIDDerm
Now looking at clinical trials safety data when thinking about immunosuppression management in the #COVID19 era:
Many biologics for #psoriasis show that biologic URI risk is similar to placebo. Based on paper from lebwohl in the @JAADjournals
#COVIDDerm
Many biologics for #psoriasis show that biologic URI risk is similar to placebo. Based on paper from lebwohl in the @JAADjournals
#COVIDDerm
What about #methotrexate?! There is a mild increase risk of infx compared w/ placebo.
Paper from @JosephMerolaMD's group in @JAADjournals showed that azathioprine, prednisone, and mycophenolate are higher risk than methotrexate!
#COVIDDerm
jaad.org/article/S0190-…
Paper from @JosephMerolaMD's group in @JAADjournals showed that azathioprine, prednisone, and mycophenolate are higher risk than methotrexate!
#COVIDDerm
jaad.org/article/S0190-…
Extrapolating from transplant lit that immunosuppression increases viral illnesses like adeno, influenza, rhino, and RSV, BUT coronavirus seems to not occur more frequently.
BUT, new paper showed higher rate of ventilation with kidney transplant pts who get #covid19
#COVIDDerm
BUT, new paper showed higher rate of ventilation with kidney transplant pts who get #covid19
#COVIDDerm
A @NEJM correspondence showed that biologic use in the #rheumatology population did not seem to increase risk of #COVID19.
Check it out yourself, with encouragment from @JosephMerolaMD to check out the supplement!
#COVIDDerm
nejm.org/doi/full/10.10…
Check it out yourself, with encouragment from @JosephMerolaMD to check out the supplement!
#COVIDDerm
nejm.org/doi/full/10.10…
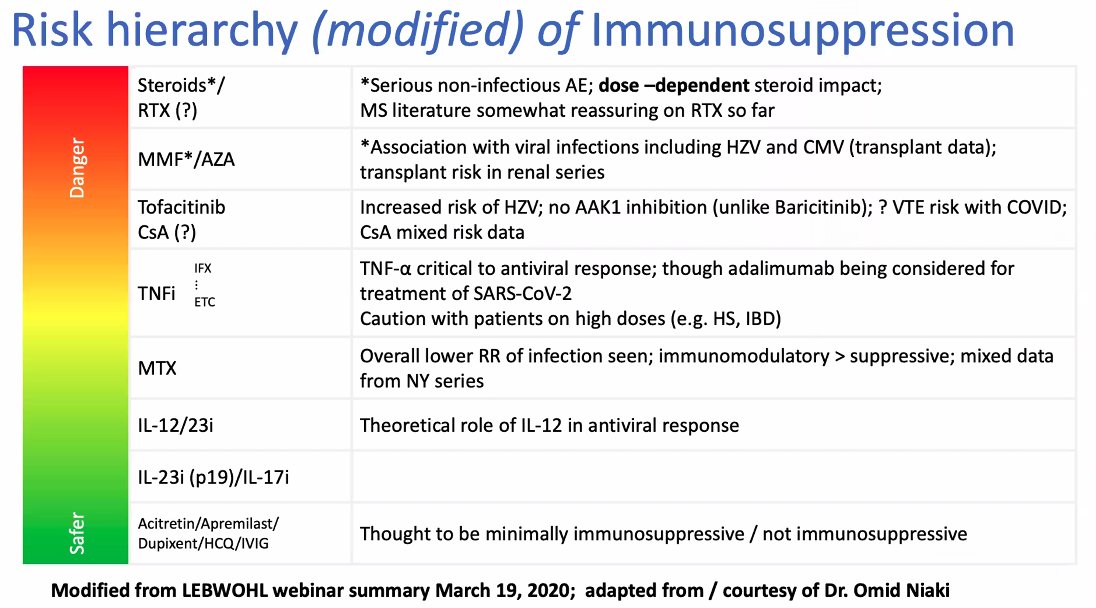
Could our immunosuppressive medications might even help patients by preventing a cytokine storm? Don't know because not enough data!
Lots more to study! Here's a slide regarding risk hierarchy edited by @JosephMerolaMD
#COVID19 #COVIDDerm #medtwitter #dermtwitter
Lots more to study! Here's a slide regarding risk hierarchy edited by @JosephMerolaMD
#COVID19 #COVIDDerm #medtwitter #dermtwitter